His bundle pacing in a patient with complete atrioventricular block and congenitally corrected transposition of the great arteries: potential of the use of extended reality and cardiac electrical activity projected into a 3-dimensional heart model

 CC BY 4.0
CC BY 4.0
His bundle pacing in a patient with complete atrioventricular block and congenitally corrected transposition of the great arteries: potential of the use of extended reality and cardiac electrical activity projected into a 3-dimensional heart model
We present a case of a 57‑year‑old man with congenitally corrected transposition of the great arteries (ccTGA), enlarged left atrium, systemic morphologically right ventricle with ejection fraction of 51% and nonreduced left (subpulmonic) ventricular ejection fraction on cardiac magnetic resonance imaging. The patient had permanent atrial fibrillation and third‑degree atrioventricular block with predominant junctional rhythm of mean 41 (min‑max, 32–65) bpm (Figure 1A), frequent ventricular contractions, and decreased exercise tolerance. Spiroergometry was stopped after 2.47 minutes (4.6 metabolic equivalents) at 40 seconds of exertion due to exaggeration of ventricular arrhythmias to a nonsustained ventricular tachycardia episode. Oxygen consumption at peak exercise reached 11.7 ml/kg/min. Coronary computed tomography angiography showed an anomalous aortic origin of the left coronary artery (Figure 1B).
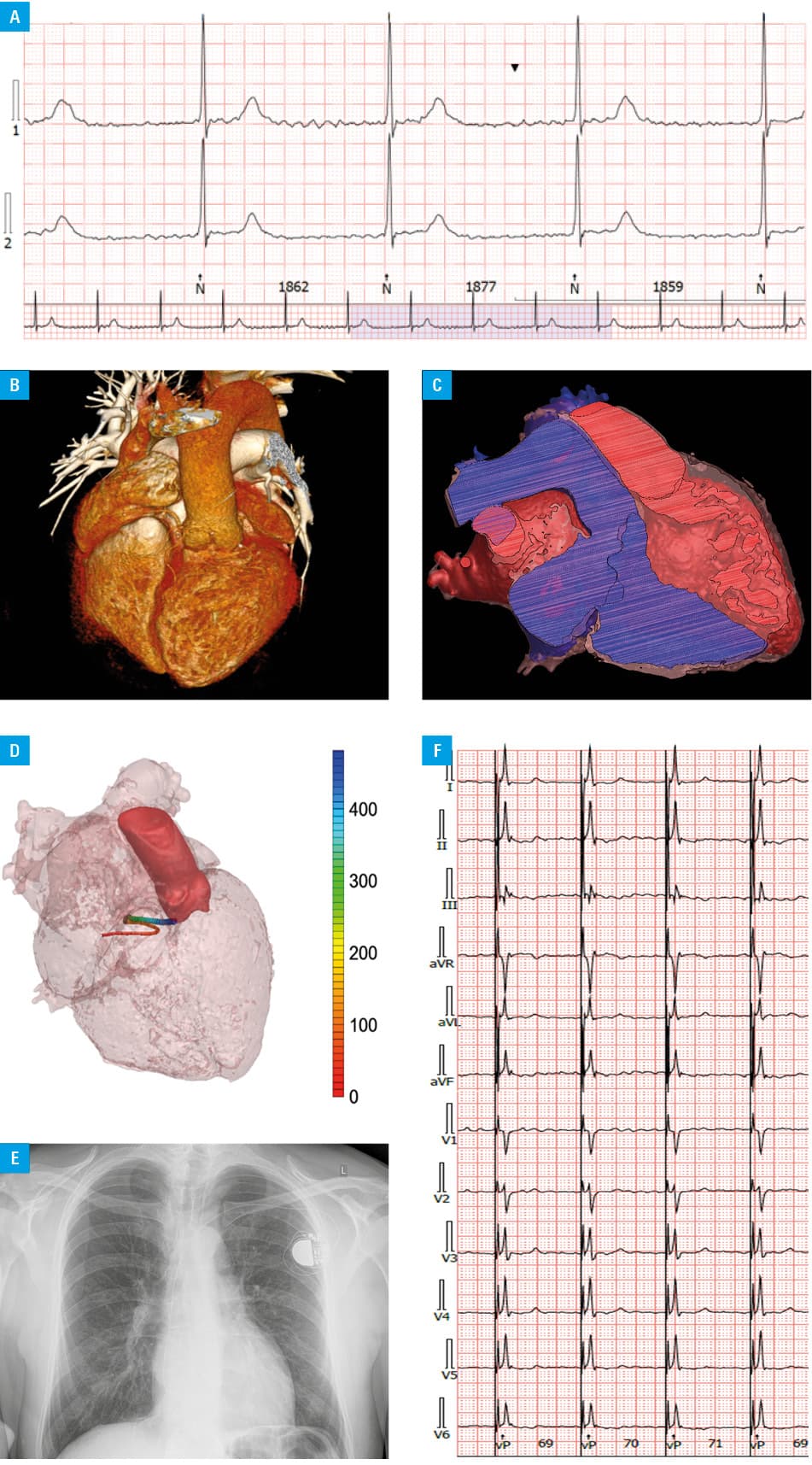
After multidisciplinary assessment, taking into account anticipated high ventricular pacing percentage, the patient was scheduled for conduction system pacing.1 Potentially abnormal positions of the atrioventricular node, the bundle of His (anterior and lateral displacement) as well as left bundle branches in ccTGA were taken into account.2,3 Considering the rare clinical setting and complex cardiac anatomy, to increase the effectiveness and safety of the procedure, we performed 3‑dimensional (3D) visualization of the heart using HoloLens 2 technology (Microsoft Corp., Redmond, Washington, United States; Figure 1C). Moreover, we assessed the CineECG computed anatomical pathway of the electrical activity of the heart, also superimposed on the personalized cardiac model (Figure 1D; Supplementary material, Additional information).4 The procedure was uneventful, resulted in optimal electrical parameters of the implanted His bundle pacing (HBP) lead (SelectSecure MRI SureScan Model, 3830–69 cm; Medtronic, Inc., Minneapolis, Minnesota, United States) as well as low total fluoroscopy (3.53 min) time (Figure 1E and 1F; Supplementary material, Figure S1). Twelve‑lead electrocardiograms and the electrical pathway of the heart before and during HBP indicated selective (isoelectric line in all 12 leads)5 and nonselective (after transition from selective HBP increase in QRS amplitudes in I, II, and V6 and the presence of a pseudodelta wave which leads to QRS prolongation, lead V6 R‑wave peak time <100 ms, lack of slurring, notching and / or plateaus in leads I, V1, V4–6)5 HBP, and showed resembling anatomical pathways of the electrical activity of the heart when superimposed over the cardiac model, as compared to endogenous QRS complexes (Supplementary material, Figures S2A–S2C). This was in contrary with the electrical activity observed during probable junctional rhythm with episodic right bundle branch block (RBBB) or escape ventricular rhythm with RBBB QRS morphology observed in this patient (Supplementary material, Figures S2D and S3D). The patient reports improved exercise tolerance with 97.3% of HBP, and electrical parameters of the HBP lead are optimal (408 ohms; bipolar sensing, 2.8–4 mV; pacing threshold, 0.75 V/0.4 ms) after over 1‑year follow‑up.
To the best of our knowledge, this is the first use of this minimally‑invasive personalized approach before conduction system pacing procedure and showing cardiac electrical activity of the heart projected into a 3D heart model before and during selective and nonselective HBP in a patient with complex cardiac anatomy.
- Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021; 42: 3427‑3520.
- Baumgartner H, De Backer J, Babu‑Narayan SV, et al. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J. 2021; 42: 563‑645. | Crossref
- Moore JP, Gallotti R, Shannon KM, et al. Permanent conduction system pacing for congenitally corrected transposition of the great arteries: a Pediatric and Congenital Electrophysiology Society (PACES) / International Society for Adult Congenital Heart Disease (ISACHD) Collaborative Study. Heart Rhythm. 2020; 17: 991‑997. | Crossref
- Boonstra MJ, Brooks DH, Loh P, et al. CineECG: a novel method to image the average activation sequence in the heart from the 12‑lead ECG. Comput Biol Med. 2022; 141: 105128. | Crossref
- Szotek M, Kula W, Malik A, et al. His bundle pacing in a patient with atrioventricular conduction abnormalities, persistent atrial flutter at high thromboembolic and bleeding risk after hybrid coronary revascularization and left atrial appendage closure ‑ case report. Bulg Cardiol. 2023; 29: 82‑88. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION