How to treat patients with thrombotic antiphospholipid syndrome in 2024?
Key words: antiphospholipid syndrome, arterial thrombosis, direct oral anticoagulants, hydroxychloroquine, venous thromboembolism

 CC BY 4.0
CC BY 4.0
How to treat patients with thrombotic antiphospholipid syndrome in 2024?
Antiphospholipid syndrome (APS) encompasses a range of clinical conditions, particularly thrombotic or obstetrical manifestations, associated with the presence of antiphospholipid antibodies. Managing thrombotic APS in daily clinical practice can be challenging and requires thorough risk stratification and tailored treatment strategies. Primary prophylaxis focuses on correcting the traditional thrombotic risk factors and, in certain situations, may include low‑dose aspirin and / or prophylactic anticoagulants (eg, low‑molecular‑weight heparin). Treatment of thrombotic APS primarily involves long‑term anticoagulation with vitamin K antagonists (VKAs). In some cases, a combination of VKAs and low‑dose aspirin, increased doses of VKAs with an international normalized ratio target greater than 3, or a switch to therapeutic doses of low‑molecular‑weight heparin might be employed. The use of hydroxychloroquine is essential in patients with secondary systemic lupus erythematosus and may be considered in individuals with recurrent thrombosis. In other selected situations, the use of immunomodulatory agents can be considered.
Introduction
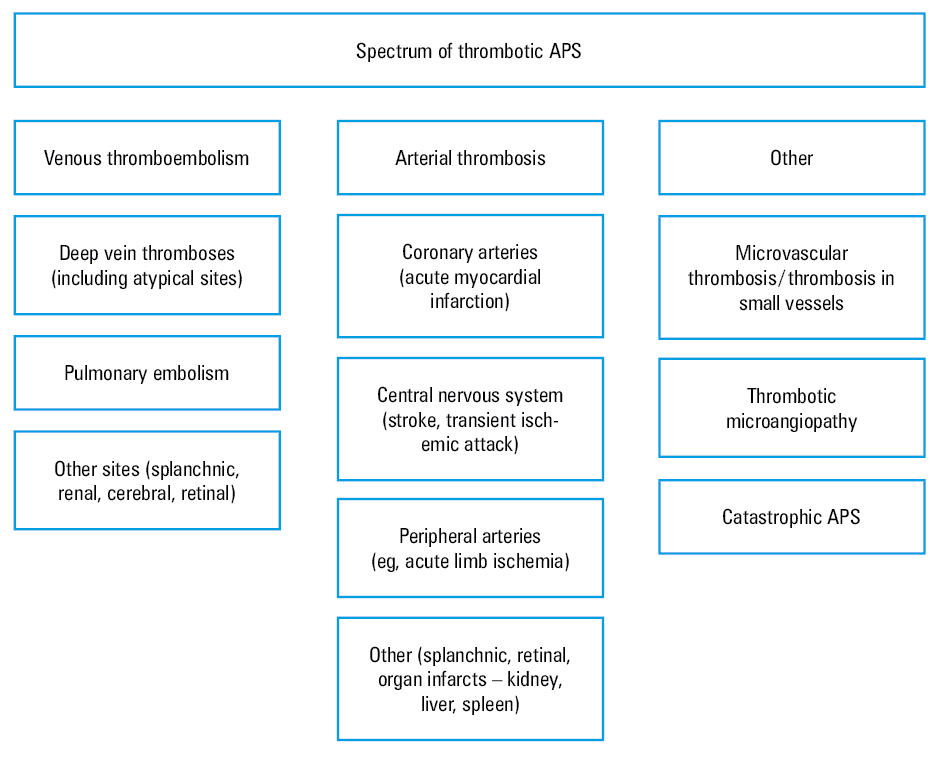
Antiphospholipid syndrome (APS) encompasses a range of clinical conditions, particularly thrombotic or obstetrical manifestations, associated with the presence of antiphospholipid antibodies (aPL). Given their frequency and prognostic impact, thrombotic manifestations are a major clinical feature in patients with APS, and thus have been included in all previous and the most recent sets of classification criteria.1,2 In daily clinical practice, patients with at least 1 thrombotic manifestation are considered to have thrombotic APS. However, this population is heterogeneous, varying significantly depending on the vascular bed involved (ie, macro and / or microcirculation, arterial or venous), which is associated with different risk factors for the occurrence of thrombosis and requires different risk stratification processes and treatment measures. The spectrum of thrombotic APS is detailed in Figure 1. Catastrophic APS is a distinct clinical scenario and will not be discussed here. In this paper, we aim to review the current knowledge on and recommendations for the management of macrovascular thrombotic APS.
New classification criteria
The recently released 2023 American College of Rheumatology / European League Against Rheumatism (ACR / EULAR) APS classification criteria2 refined the spectrum of thrombotic manifestations in patients with APS.2 Two specific domains were dedicated to macrovascular clinical manifestations: venous thromboembolism (VTE) and arterial thrombosis (AT). Moreover, for each of these domains, a different weight was allocated depending on the presence or absence of a high‑risk cardiovascular profile for VTE or AT, respectively, with individuals presenting a high‑risk profile receiving a lower score.
Diagnosis of APS is based on the identification of suggestive symptoms, such as macro- or microthrombotic events, along with the presence of persistently positive aPL. Of note, the classification criteria are not intended to be used for diagnostic purposes and should not replace clinical reasoning in daily clinical practice; however, they might have direct clinical relevance and guide our decision‑making.
How can the new American College of Rheumatology / European League Against Rheumatism criteria impact clinical practice?
First, in patients who experience a thrombotic event, whether venous or arterial, it is crucial to review all potential contributing factors, particularly traditional risk factors, to determine if the thrombosis is unexplained / unprovoked. The new set of criteria provide detailed and useful tools for this assessment (Figure 2).2 Second, in patients with definite thrombotic APS, it is mandatory to address and mitigate other possible thrombotic risk factors to minimize the frequency of recurrence, utilizing risk stratification principles.2
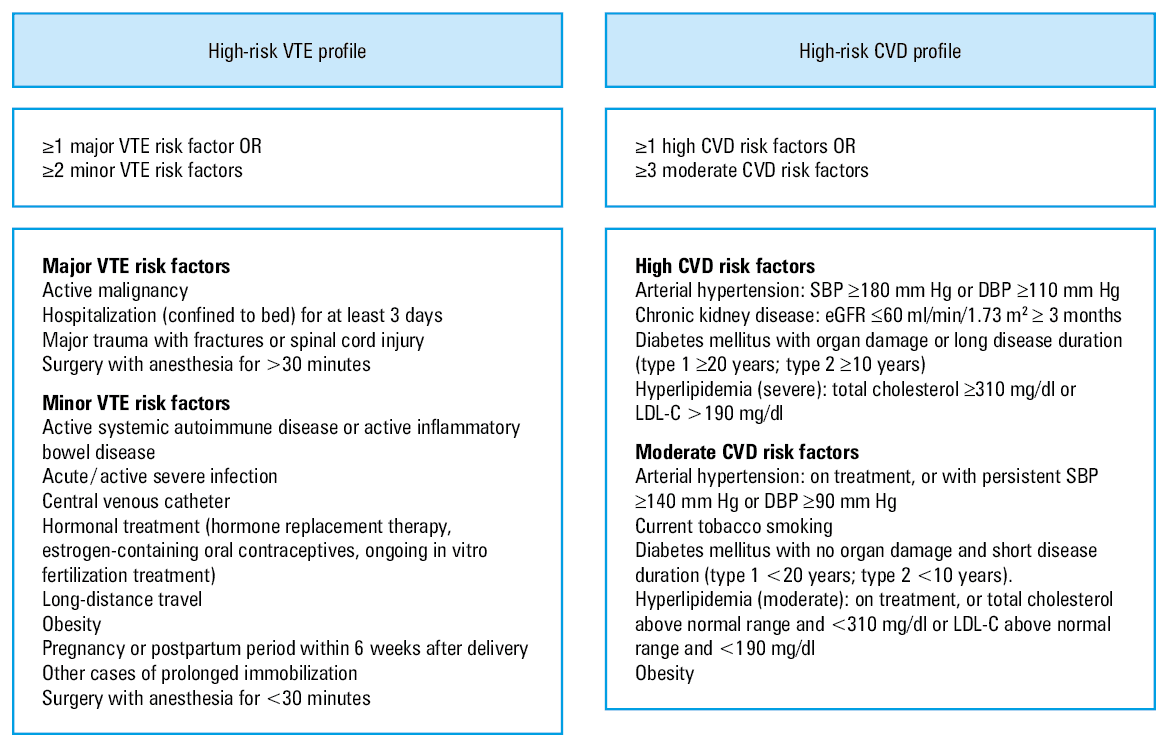
Abbreviations: CVD, cardiovascular disease; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; LDL‑C, low‑density lipoprotein cholesterol; SBP, systolic blood pressure; VTE, venous thromboembolism
Nevertheless, exploring the impact of the updated laboratory criteria on the management of patients with APS is beyond the scope of this review.
When to suspect antiphospholipid syndrome in the context of thrombotic manifestations
A cornerstone in the management of APS is the diagnostic process. Thus, in the context of a thrombotic event, clinicians should consider an APS diagnosis in certain clinical scenarios (ie, unprovoked / mildly provoked VTE, young age) or in the presence of additional features (eg, prolonged activated partial thromboplastin time [aPTT], thrombocytopenia, systemic lupus erythematosus [SLE] or other inflammatory rheumatic diseases, a history of pregnancy morbidity compatible with APS, livedo reticularis, cardiac valve abnormalities, etc.). In these patients, prompt laboratory screening for the identification of aPL should be performed to ensure appropriate management. The general diagnostic principles, especially imaging modalities, are similar to those applying to the general population, and should follow the local or international recommendations.
Risk stratification and primary prevention of thrombotic manifestations
In patients with aPL, risk stratification should be performed in 2 specific contexts: primary and secondary prevention.
Primary prevention
In patients with isolated positive aPL without a thrombotic history, the risk for thrombosis should be evaluated and minimized. In some patients, the use of prophylactic drugs (ie, low‑dose aspirin [LDA], anticoagulants) might be recommended, depending on the risk of developing thrombotic manifestations in follow‑up. In daily clinical practice, several complementary tools for assessing the thrombotic risk are available; therefore, all parameters should be carefully analyzed.
First, we should evaluate the general thrombotic risk using the principles available for the general population. Each patient should be assessed for the presence of general risk factors for VTE and cardiovascular conditions that increase the risk for developing arterial events, respectively. With respect to arterial events, the risk stratification scores used in the general population can be considered, that is, the Framingham score,3 the Systematic Coronary Risk Evaluation (SCORE) system proposed by the European Society of Cardiology,4 along with the risk stratification system proposed in the recently published classification criteria.2 The EULAR guideline on cardiovascular risk management in patients with rheumatic and musculoskeletal diseases states that the general cardiovascular risk should be accurately and completely evaluated in patients with APS, without suggesting any particular scoring system for the assessment.5 A new variant of the adapted Global Anti‑Phospholipid Syndrome Score (aGAPSS) specific for cardiovascular disease, incorporating traditional cardiovascular risk factors and APS‑specific features, might be a promising tool, but it needs further validation using large, longitudinal, prospective trial data.6 Evaluation of structural vessel wall abnormalities using ultrasonography could provide additional information about the general arterial cardiovascular risk in patients with APS.7 Similarly, when assessing the VTE risk factors, we can use the principles applicable to the general population or the risk stratification system proposed in the recent classification criteria guideline.2
The second element that should be considered when assessing the thrombotic risk is the aPL profile: it is well known that patients with multiple positive aPL test results (particularly triple‑positive patients) have a higher risk of developing clinical manifestations than individuals with other aPL profiles (ie, single‑positive, lower titers, etc.).8 In daily clinical practice, we can use the simple principle suggested by the guidelines for the management of APS, according to which high‑risk patients are those with positive lupus anticoagulant (LA), a double- or triple‑positive profile, or high titers of aPL.8
The third method for assessing the thrombotic risk is the use of APS‑specific scores developed for risk stratification in this population. Otomo et al9 developed the Antiphospholipid Score, a multiparametric score based on results of laboratory tests related to the aPL profile (anticardiolipin, anti-β2‑glycoprotein I [anti-β2‑GPI], and antiphosphatidylserine / prothrombin [anti‑PS/PT] antibodies) and LA coagulation parameters evaluated using different laboratory techniques (aPTT, kaolin clotting time, dilute Russell viper venom time), with each of these items being assigned a score derived from the statistical analysis. Furthermore, Sciascia et al10 developed the GAPSS, a risk evaluation system based on positive aPL test results (LA, anticardiolipin, anti-β2‑GPI, and anti‑PS/PT) combined with the presence of other cardiovascular risk factors, such as hyperlipidemia and arterial hypertension. Taking into account the potentially limited availability for anti‑PS/PT, a variant of GAPSS was created (aGAPSS).11 Analysis of pooled data from 10 cohort studies showed that GAPSS and aGAPSS values are increased in individuals with a history of thrombotic events, and that these scores could be used for thrombotic risk stratification in patients with APS.12
The fourth factor that should be taken into account during thrombotic risk stratification in patients with APS is the presence of an associated disease, such as SLE, as well as disease activity of secondary autoimmune conditions and the concomitant pharmacotherapy (ie, immunosuppressants and glucocorticoids). In such patients, achieving a low activity of the secondary autoimmune disease as well as using the lowest possible doses of glucocorticoids might improve the overall cardiovascular risk.5
The basic recommendations for primary prevention are the same as for the general population: good hydration, avoidance of prolonged immobilization, weight control, and avoidance of drugs that increase the VTE risk (eg, estrogens). For AT prophylaxis, clinicians should aim at the correction of traditional cardiovascular risk factors, such as smoking, diabetes, hypertension, and high cholesterol and triglyceride levels.
In special circumstances (ie, surgery, postpartum period, assisted reproduction, prolonged immobilization, etc.), primary prevention of VTE with prophylactic doses of low‑molecular‑weight heparin (LMWH) should be recommended according to the existing guidelines, taking into account the high risk of VTE in these patients.13
Several studies support the use of LDA (75–100 mg/day) for primary prevention of thrombotic events in aPL patients. Arnaud et al14 pooled data from 5 international cohort studies in a meta‑analysis and reported a positive effect of LDA for the prevention of the first thrombosis (hazard ratio, 0.43; 95% CI, 0.25–0.75). The protective effect was significant for arterial but not for venous thrombosis, in patients with SLE and asymptomatic aPL carriers when subgroup analysis was performed.14 This topic was further explored in the ALIWAPAS study,15 which compared thromboprophylaxis with LDA vs LDA plus low‑intensity warfarin in patients positive for aPL. This prospective, multicenter, open, randomized controlled trial showed no differences in the number of thrombotic episodes between the groups. An unfavorable safety profile was reported for the combination of LDA plus low‑intensity warfarin, and the authors concluded that this therapeutic regimen is not suitable for the primary prevention of thrombosis in patients with aPL.15
The EULAR guidelines8 recommend primary prophylaxis with LDA in asymptomatic aPL‑positive patients without thrombotic or obstetric manifestations who have a high‑risk aPL profile, independently of the presence of other risk factors, and in individuals with SLE and a high‑risk aPL profile. However, in patients with SLE and a low‑risk aPL profile, prophylactic use of LDA may also be considered.8 In individuals with a low‑risk aPL profile, with or without SLE, the risk stratification and the decision for implementing the LDA treatment could be based on risk scores, such as the APS score or the GAPSS/aGAPSS, and on the general risk assessed according to the recommendations for the general population. In patients with obstetric manifestations but no history of thrombotic events, LDA is recommended after careful evaluation.8 In these patients, refining the risk stratification based on APS scores, the aPL profile, and general risk assessment could guide the decision for implementing the LDA treatment.
Secondary prevention
In patients with thrombotic APS, clinicians should evaluate the risk for recurrent thrombotic events. Patients should be assessed using secondary prevention tools, as in the case of primary prevention. After the first thrombotic event, clinicians should revise the thrombotic risk assessment considering general risk factors, the aPL profile, and coexistence of other autoimmune diseases, such as SLE. Also, the specific APS risk scores should be calculated to obtain a global perspective of the thrombotic risk. All these measures should be complemented with antithrombotic treatment that will be discussed in the subsequent paragraphs.
Treatment of thrombotic antiphospholipid syndrome
While there are some differences with respect to the general principles for the management of venous and arterial thromboses, the treatment of thrombotic APS is mainly based on antithrombotic therapy: anticoagulants (mainly vitamin K antagonists [VKAs]), LDA, and, in some cases, a combination of the two. In some patients, additional therapies (ie, hydroxychloroquine [HCQ]) can be considered (Figure 3).
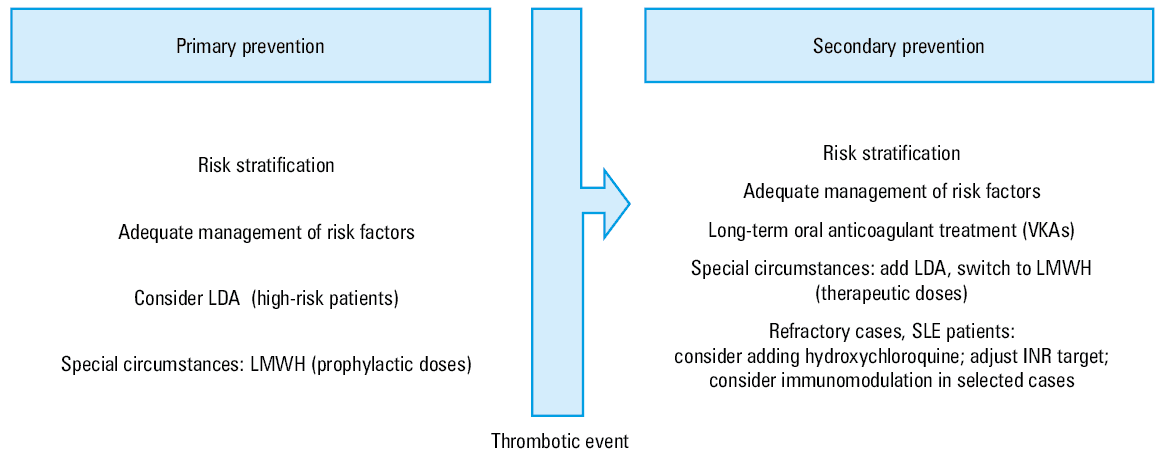
Abbreviations: INR, international normalized ratio; LDA, low‑dose aspirin; LMWH, low‑molecular‑weight heparin; SLE, systemic lupus erythematosus; VKA, vitamin K antagonist
Venous thromboembolism
Treatment of acute VTE is based on the use of unfractionated heparin (UFH) or LMWH in therapeutic doses, followed by indefinite long‑term anticoagulation with VKA with a target international normalized ratio (INR) of 2 to 3.8 Due to increasing availability, ease of administration, and low bleeding risk, and based on the recommendations of new guidelines on pulmonary embolism and deep vein thrombosis, direct oral anticoagulants (DOACs) are used more and more often in the acute‑phase treatment of VTE,16 before a diagnosis of APS is ruled out. However, clinicians should be careful if the suspicion of APS is high, and avoid DOACs as the first‑choice treatment in such cases. Moreover, because of laboratory interferences with the anticoagulant treatment, testing for LA should be performed, if possible, before the initiation of anticoagulation.17 In patients with spontaneously increased aPTT, suspicion of APS should be raised, and aPTT cannot be used for UFH treatment monitoring. In such cases, LMWH should be chosen instead. Correction of additional risk factors for VTE should always be carefully assessed, and evaluation of the bleeding risk should be performed at each follow‑up visit.
In the cases of recurrences under VKA therapy despite a target INR range, the EULAR guidelines for the management of APS suggest one of the following: increased doses of VKA with an INR target of 3 to 4, addition of LDA to the therapy, or a switch to therapeutic doses of LMWH.8 Before implementing any of these changes, clinicians should assess adherence to the treatment and schedule a more frequent monitoring of INR to obtain and maintain a correct therapeutic range.8
In the particular situation of provoked VTE, the EULAR guidelines recommend a limited duration of anticoagulant treatment.8 Duration of anticoagulation might be extended in the case of a high‑risk aPL profile and when other established risk factors for recurrence are present.8 However, the decision for an extended or long‑term anticoagulation after an episode of provoked VTE is challenging in daily clinical practice and should be individualized.
Arterial thrombosis
In patients with AT, clinicians can choose between VKA, LDA, and a combination of these 2 treatments.8 However, the EULAR guidelines recommend treatment with VKA over LDA alone, taking into account the risk of recurrences and individual bleeding risk.8 In some high‑risk cases, a combination treatment (VKA + LDA) should be considered. In clinical practice, there are 2 possible scenarios: patients with “pure” AT, in whom VKA should be the first‑choice treatment, and patients with “mixed” AT (thrombosis and structural atherosclerotic lesions on the vessel wall), in whom a combination of VKA and LDA is often used.18 A correct assessment of the general atherosclerotic risk profile of the patient is mandatory, and the impact of the traditional risk factors should be minimized. Statins should be prescribed according to the total cholesterol and low‑density lipoprotein cholesterol levels, and the target values of these parameters should be reached.
Direct oral anticoagulants
Direct oral anticoagulants are now the standard treatment in most patients with VTE. However, evidence against the use of DOACs in patients with APS has been reported. These results were incorporated into the recent recommendations for the management of VTE.16,19 Most of the available data in APS refer to the use of Xa inhibitors (xabans).
Some clinical case reports and small case series reporting the use of DOACs in thrombotic APS raised concerns about the efficacy of these drugs in secondary prophylaxis of thrombosis. Triple‑positive testing for aPL, concomitant SLE, and a history of arterial events were associated with a high risk for thrombosis recurrences in the context of DOAC treatment.20
The RAPS (Rivaroxaban in Antiphospholipid Syndrome) study21 was one of the first randomized, controlled, open‑label, phase 2/3, noninferiority trials that compared VKA and rivaroxaban in patients with previous VTE, with a laboratory parameter as a primary outcome (endogenous thrombin potential). At day 42 after randomization, the primary outcome was not reached (noninferiority threshold), and no thrombotic event was recorded in either arm at the end of the study. The authors concluded that rivaroxaban did not increase the overall thrombotic risk, but the short duration of the study made it difficult to reach a clinically relevant conclusion.21
The TRAPS (Trial on Rivaroxaban in AntiPhospholipid Syndrome) trial22 was designed to assess the efficacy and safety of rivaroxaban vs warfarin in high‑risk (triple aPL‑positive) patients with thrombotic APS. The trial was terminated prematurely because of a high number of events, including thromboembolic events (ischemic stroke, myocardial infarction), among patients in the rivaroxaban arm. A supplementary analysis of data from the TRAPS trial was published at 2‑year follow‑up, and a high rate of recurrences was reported in the DOAC group (33.3%), as compared with the warfarin group (5.7%).23
Ordi‑Ros et al24 reported the results of an open‑label, noninferiority trial evaluating the efficacy of treatment with rivaroxaban vs warfarin in patients with thrombotic APS. A high number of recurrent thromboses, especially strokes, occurred in the rivaroxaban arm. Interestingly, an increased risk for recurrent thromboses in the rivaroxaban group was noted in the patients with previous AT, livedo racemosa, or cardiac valvular abnormalities related to APS.24 Similarly, Martinelli et al25 reported a high incident rate of recurrent thromboses (especially AT; all patients with recurrences were triple‑positive for aPL) in the group of patients treated with rivaroxaban vs VKA, in a real‑life cohort of VTE patients. The hazard ratio for recurrent thrombosis in the patients on rivaroxaban vs VKA was 7.53 (95% CI, 0.84–67.6).
The efficacy and safety of apixaban in thrombotic APS was evaluated in the ASTRO‑APS (Apixaban for Secondary Prevention of Thromboembolism Among Patients with Antiphospholipid Syndrome) trial.26 A high number of thrombotic events (strokes) was noted in the apixaban group, and the study was terminated early.26
A post hoc analysis of pooled data from studies on dabigatran in VTE (RE‑COVER, RE‑COVER II, and RE‑MEDY)27 showed that in the subgroup of patients with APS there was no difference in the rate of VTE or VTE‑related death between dabigatran and warfarin. Recently, Nikolopoulos et al28 reported a different transcriptomic profile in patients with arterial and venous APS and individuals with SLE. Based on these results, the authors described different mechanisms for the occurrence of thrombosis in these 2 vascular beds and suggested that inhibition of factor IIa (ie, dabigatran) might be more effective than inhibition of factor Xa (ie, rivaroxaban, apixaban) for the treatment of thrombotic APS.28
Recent studies reported a therapeutic profile of DOACs in patients with single or double positivity for aPL. Liu et al29 presented data from a retrospective study evaluating treatment with DOACs (apixaban or rivaroxaban) vs warfarin following an acute thrombotic event in APS patients. At a median follow‑up of 54 months, the recurrence rate was similar in both subgroups, with no differences in event‑free survival. In a retrospective study, Williams et al30 reported that single- and double‑positive aPL patients with APS and VTE treated with DOACs (rivaroxaban in 90% of cases) had a higher rate of recurrences than the patients treated with warfarin; however, the difference was not significant(15.4% vs 5.3%, respectively; P = 0.15).
Although the recently released or updated guidelines are supported by a general consensus, they are not exactly identical. For instance, in the 2019 guidelines for the diagnosis and management of pulmonary embolism, issued by the European Society of Cardiology in collaboration with the European Respiratory Society,16 the use of all DOACs for the treatment of APS is strictly contraindicated. According to the 2019 EULAR recommendations for the management of APS in adults,8 rivaroxaban should not be used in the context of triple aPL positivity and in patients with AT. The same guideline suggests that DOACs could be considered in patients with difficulties achieving the target INR despite good adherence to the treatment, or in patients with contraindication (allergy or intolerance) to VKAs.8 Other recommendations suggest that DOACs could be taken into consideration in the case of single- or double‑positive aPL testing.31,32 The decision should always be made in collaboration with the patient.
Hydroxychloroquine
Some studies reported the antithrombotic and immunomodulatory properties and positive effects of HCQ on traditional cardiovascular risk factors; therefore, it seems reasonable to consider this drug for the treatment of selected patients with thrombotic APS.33 For instance, there is evidence that treatment with HCQ in individuals with primary APS was associated with a significant reduction in the levels of immunoglobulin (Ig) G anticardiolipin and IgG / IgM anti-β2‑GPI.34 Furthermore, in a small, prospective, nonrandomized study, Schmidt‑Tanguy et al35 reported a positive effect of adding HCQ to the standard oral anticoagulant therapy in patients with venous thrombotic APS. The efficacy and safety of HCQ in the prevention of recurrences in patients with thrombotic APS were evaluated in a pilot open‑label randomized prospective study.36 The addition of HCQ to the standard care was associated with a lower incidence rate of thrombosis, as compared with the standard care alone, without safety concerns.36 According to these results, HCQ could be prescribed for secondary prevention of thrombosis in some patients with primary APS, especially those who experience recurrences despite appropriate antithrombotic treatment. Patients with concomitant SLE and APS should receive HCQ independently of the presence of any APS‑related thrombosis as one of the essential therapeutic options.37
A randomized controlled trial investigating the efficacy of HCQ in the primary prevention of thrombosis in aPL‑positive patients was terminated early because of a low recruitment rate.38 In a meta‑analysis by Arnaud et al,14 no independent protective effect of HCQ in the primary prevention of thrombotic events in patients positive for aPL was found. Thus, the possible protective role of HCQ in the primary prevention of thromboses in aPL‑positive patients needs further investigation. Until such results are available, HCQ should only be used (in the absence of contraindications) in SLE patients with or without positivity for aPL.
Other immunomodulatory approaches, including intravenous immunoglobulin and biological treatments (anti–B‑cell depletion therapies, anti–B‑cell activating factor) have been suggested, but their use is supported only by anecdotal reports or nonrandomized studies39,40 (Table 1).
Therapeutic option | Mechanism of action | Examples of indications | Target patient groups |
Hydroxychloroquine | Immunomodulation, platelet aggregation inhibition | Adjunctive therapy, especially in patients with SLE | APS patients with SLE |
Corticosteroids | Broad immunosuppression | Severe thrombocytopenia, CAPS | Acute management of CAPS (short‑term) |
Intravenous immunoglobulin | Modulation of immune response | CAPS, severe thrombocytopenia, refractory cases | CAPS, refractory thrombocytopenia |
Rituximab | Anti‑CD20 monoclonal antibody | Refractory thrombocytopenia, noncriteria manifestations | APS with noncriteria manifestations, refractory cases, refractory thrombocytopenia |
Plasmapheresis | Removal of circulating autoantibodies | CAPS, severe refractory cases | Acute management of CAPS |
Eculizumab | Anticomplement therapy | CAPS, severe refractory cases | Acute management of CAPS, microvascular APS |
Belimumab | B‑lymphocyte stimulator inhibition | SLE‑associated APS, refractory cases | APS with associated SLE, refractory cases |
Cyclophosphamide | Alkylating agent | Severe, refractory CAPS | CAPS, particularly severe cases |
Mycophenolate mofetil | Inhibition of lymphocyte proliferation | Nonthrombotic manifestations, refractory APS | Nonthrombotic APS, especially with SLE |
Azathioprine | Immunosuppression, inhibition of purine synthesis | Nonthrombotic APS manifestations, SLE‑associated APS | APS with SLE, refractory nonthrombotic manifestations |
Statins | Anti‑inflammatory effect, thrombotic risk reduction | Adjunctive therapy to reduce thrombotic risk | APS patients at a high cardiovascular risk |
Tacrolimus | Calcineurin inhibition | Refractory APS, especially with SLE | Severe, refractory cases, particularly with SLE |
Pragmatic ideas for daily clinical practice
The first step in the correct management of APS is its diagnosis. Additionally, in patients with a history of thrombotic events, clinicians should consider a possibility of this etiology. In an emergency setting, the main features associated with a high suspicion of APS should be kept in mind, and appropriate laboratory tests should be ordered to confirm or exclude the condition. Confirming positivity for aPL, especially if detected for the first time in an acute phase, is highly recommended (eg, after >12 weeks). When LA is positive, the possible interferences (systemic inflammation, anticoagulant treatment) should be considered for a correct interpretation of the test.17 If in doubt, the results should be discussed with the specialist laboratory staff. If APS is suspected, DOACs should not be used for acute or chronic treatment of thrombotic APS. At each visit, clinicians should revise and adjust the management of the risk factor for thrombosis other than aPL positivity. Moreover, the bleeding risk should be balanced with the thrombotic risk and managed accordingly. Complex clinical cases (ie, multiple recurrent thrombotic events despite the correct antithrombotic treatment) should be referred to expert centers or discussed in multidisciplinary teams or dedicated international networks (eg, the European Reference Network on Rare and Complex Connective Tissue and Musculoskeletal Diseases).
Conclusions
The management of APS might be challenging in daily clinical practice. Clinicians should perform an extensive evaluation of the thrombotic risk, taking into account not only the aPL profile but also the overall cardiovascular risk. Treatment is generally based on long‑term anticoagulation with VKA, while DOACs should be avoided, especially in patients with a high‑risk aPL profile. A combination of LDA and VKA or treatment with increased doses of VKA with an INR target greater than 3 can be considered for the management of AT. HCQ might be a therapeutic option in patients with refractory thrombotic APS. All individuals with APS should undergo a long‑term follow‑up.
- Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006; 4: 295‑306. | Crossref
- Barbhaiya M, Zuily S, Naden R, et al. 2023 ACR/EULAR Antiphospholipid syndrome classification criteria. Ann Rheum Dis. 2023; 82: 1258‑1270.
- D’Agostino Sr RB, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008; 117: 743‑753. | Crossref
- Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur Heart J. 2021; 42: 3227‑3337.
- Drosos GC, Vedder D, Houben E, et al. EULAR Recommendations for cardiovascular risk management in rheumatic and musculoskeletal diseases, including systemic lupus erythematosus and antiphospholipid syndrome. Ann Rheum Dis. 2022; 81: 768‑779. | Crossref
ARTICLE INFORMATION