Medical history–taking is a fundamental part of the diagnostic process. The skill of obtaining an accurate medical history is something doctors learn throughout their entire career. While paraclinical methods are essential, they are sometimes insufficient to establish a diagnosis. Nurses, who spend more time with patients than physicians, often gather information that may be helpful in making a diagnosis.
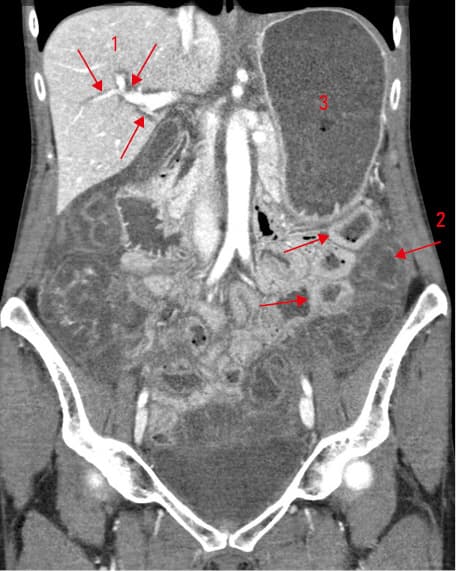
A 54‑year‑old woman with a history of epilepsy was admitted to an emergency department in the late evening due to suspected gastrointestinal bleeding. She complained of abrupt, severe abdominal pain lasting for approximately 10 hours, accompanied by vomiting and bloody, watery diarrhea. She denied having consumed unusual food products and had no history of pre‑existing medical conditions. On physical examination, the patient appeared exhausted, with blood pressure of 80/45 mm Hg. Prolonged capillary refill and tenderness in the right mesogastrium were observed. Her stool was watery and pinkish. Laboratory investigations showed elevated levels of aminotransferases (alanine transaminase, 14.8 µkat/l; reference range [RR], 0–0.57 µkat/l; aspartate aminotransferase, 21.1 µkat/l; RR, 0–0.52 µkat/l; alkaline phosphatase, 2.8 µkat/l; RR, 0.77–2.03 µkat/l), leukocytosis (19.9 × 109/l; RR, 4–10 × 109/l), and signs of hemoconcentration. Amylase levels were normal. Abdominal X‑ray showed no signs of ileus or pneumoperitoneum. The patient was admitted to the intensive care unit with a diagnosis of acute gastroenteritis with dehydration, likely of infectious origin. The elevation of transaminase levels was attributed to hypotension. To rule out hepatic vessel obstruction, computed tomography of the abdomen was performed, which excluded intra‑abdominal ischemia and venous occlusion (Figure 1). The differential diagnosis became complicated by additional findings: gastrectasia, periportal cuffing, and swelling of the gallbladder bed and intra‑abdominal fat, along with signs of acute colitis, such as thickening of the colon wall. The admitting physician still suspected acute infectious gastroenteritis. The patient was rehydrated and treated with piperacillin / tazobactam and oral vancomycin. Blood pressure normalized by the morning, but intense abdominal pain (7–9 points on the visual analogue scale) persisted, along with pink watery diarrhea. An atypical course of infectious gastroenteritis was suspected. The doctors were puzzled by the sudden onset of hemorrhagic diarrhea, accompanied by unusually intense abdominal pain and liver damage, in an otherwise healthy individual with a negative epidemiological and drug history. The presence of intra‑abdominal edema, particularly around the portal vein, remained unexplained. Cuffing can accompany acute viral hepatitis (which was ruled out the next day) or cholangitis, but these conditions do not typically manifest with hemorrhagic diarrhea. It has been decided to retake the patient’s medical history to identify the triggering cause. The symptoms started abruptly. Epidemiological history was negative. The patient had not consumed anything unusual except for baked zucchini with bread. She took no medications. The physicians wondered what they might have overlooked, as the cause remained obscure. The nurse who had been attending the patient suggested that the issue could be related to the zucchini. Having spent more time with the patient, she learned that the zucchini tasted unusually bitter, but the patient did not consider this fact important enough to report. The nurse added that bitter zucchini should not be consumed, although she did not know why. Based on information obtained from ChatGPT and online resources, a diagnosis of cucurbitacin poisoning was proposed. The suspicion was confirmed by the Czech Toxicological Information Center in Prague. Infectious diarrhea was ruled out the next day. The patient was practically symptom‑free on the third day since admission, and aminotransferase levels normalized within 5 days. In cooperation with the Institute of Forensic Medicine and Toxicology in Prague, we planned to confirm the presence of cucurbitacin in blood using gas chromatography. Unfortunately, the sample could not be found as the cleaning staff mistakenly considered it waste.
Cucurbitacins constitute a diverse family of organic compounds, all belonging to highly oxygenated tetracyclic triterpenes.1 There are over 12 categories of cucurbitacins.2 They are found in edible plants of the genus Cucurbita, present worldwide, including zucchini, pumpkin, cucumber, and others. These plants produce cucurbitacins in response to environmental stress, such as poor growing conditions, and levels of these compounds decrease during maturation. According to in vivo studies, the reported toxicity of cucurbitacins ranges from 2 to 12.5 mg/kg.3 The symptoms of poisoning can be severe, but a lethal course is rare.4 In a study of 353 individuals from Europe, over 95% of patients experienced mild poisoning. Symptoms typically appear within minutes to hours following ingestion,5 and predominantly involve gastrointestinal complaints, such as nausea, vomiting, abdominal cramps, and diarrhea. Hematemesis and melena manifest in approximately a quarter of cases. Hypotension is evident in half of the patients. Our patient exhibited a typical clinical course of cucurbitacin poisoning. Given the abrupt symptom onset, it is challenging to differentiate it from acute infectious diarrhea, which may delay proper diagnosis.
Diagnosis relies mostly on clinical presentation, with crucial emphasis on careful history‑taking. Physicians should consider cucurbitacin toxicity in patients presenting with symptoms shortly after ingesting plants from the Cucurbitaceae family. It is important to ascertain whether the plant tasted unusually bitter.5
A nonspecific but common finding is the presence of edema in the intestinal wall and adjacent intra‑abdominal organs (including the pancreas). Consistent with this, we observed periportal cuffing, which was initially challenging to interpret. There is no specific antidote available, and treatment is symptomatic. Abdominal pain and diarrhea may persist for several days.4
This case shows that a properly taken medical history is crucial in the diagnostic process, especially in unclear situations.
- Kaushik U, Aeri V, Mir SR. Cucurbitacins – an insight into medicinal leads from nature. Pharmacogn Rev. 2015; 9: 12‑18. | Crossref
- Chen JC, Chiu MH, Nie RL, et al. Cucurbitacins and cucurbitane (CUC) glycosides: structures and biological activities. Nat Prod Rep. 2005; 22: 386‑399. | Crossref
- Grace N, Njoroge GN, Leonard EN. Edible and poisionous species of cucurbitaceae in the central highlands of Kenya. J East Afr Nat Hist. 1994; 83: 101‑115. | Crossref
- Indian Council of Medical Research Task Force. Assessment of effects on health due to consumption of bitter bottle gourd (Lagenaria siceraria) juice. Indian J Med Res. 2012; 135: 49‑55. | Crossref
- Ho CH, Ho MG, Ho SP, Ho HH. Bitter bottle gourd (Lagenaria siceraria) toxicity. J Emerg Med. 2014; 46: 772‑775. | Crossref
ARTICLE INFORMATION