Syndrome of a truly broken heart: the first report of left ventricular rupture in a patient with recurrent takotsubo syndrome

 CC BY 4.0
CC BY 4.0
Syndrome of a truly broken heart: the first report of left ventricular rupture in a patient with recurrent takotsubo syndrome
Takotsubo syndrome (TTS) is an acute, potentially reversible clinical syndrome characterized by transient left ventricular dysfunction.1 It is usually considered a relatively benign condition with a favorable prognosis. However, recent studies have shown that the mortality rate in patients with TTS is comparable to that observed in individuals with acute coronary syndrome (ACS),1 and complications are observed in half of TTS patients.2
An 83‑year‑old woman was admitted to a hospital with anterior wall ST‑segment elevation myocardial infarction (STEMI). Coronary angiography was immediately performed; no lesions were found in the epicardial arteries, however, a slow‑flow phenomenon in the left coronary artery was observed (Figure 1A and 1B).3 Simultaneously, left ventriculography presented a pattern of segmental contractility abnormalities characteristic of apical TTS (Figure 1C). Echocardiography showed an akinetic apex and periapical segments, with hyperkinetic basal segments of the left ventricle and global left ventricular ejection fraction (LVEF) of 35% (Figure 1D and 1E). The patient denied the occurrence of emotional or physical triggers. The InterTAK Diagnostic Score was 37, with a 2.3% probability of TTS. The diagnosis of TTS was confirmed by cardiac magnetic resonance imaging. The course of the hospitalization was uncomplicated. Follow‑up echocardiography examinations showed a gradual improvement of left ventricular contractility with LVEF of 45%, and the patient was discharged after a few days.
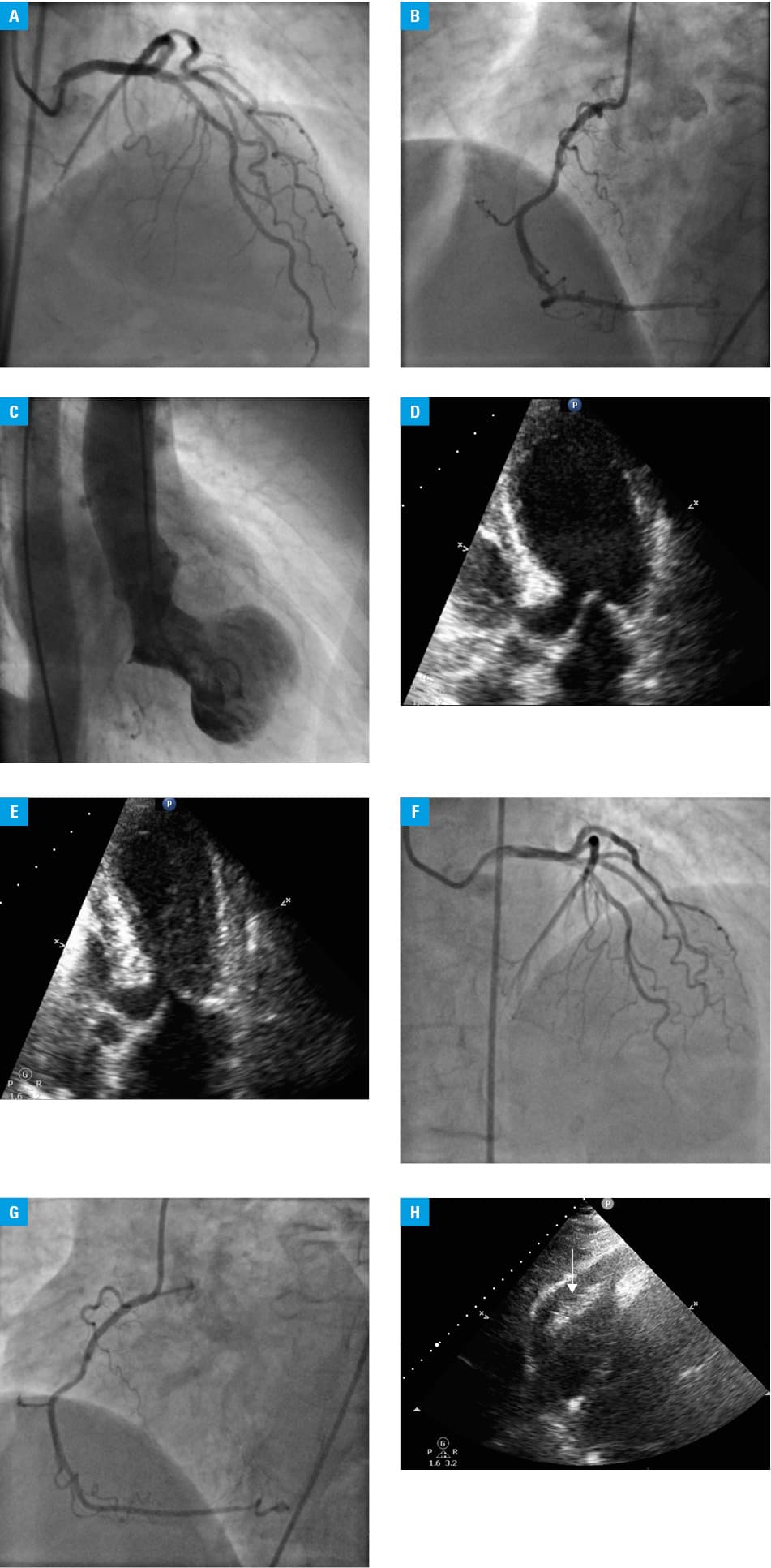
Four years later, she was readmitted due to similar, acute chest pain with STEMI. As before, coronary angiography showed no significant narrowing in the coronary arteries, with a clearly visible slow‑flow phenomenon (Figure 1F and 1G).3 Transthoracic echocardiography demonstrated a ballooning apex and akinetic periapical segments of the left ventricle with LVEF of 35% (Figure 1D and 1E). Similarly to the previous admission, no emotional or physical triggers were identified during in‑depth history‑taking, and the same result was obtained on the InterTAK Diagnostic Score. Recurrence of TTS was diagnosed, and conservative treatment was applied.
The next night, the patient’s condition suddenly deteriorated, as she developed hypotension followed by sudden cardiac arrest with pulseless electrical activity. Point‑of‑care transthoracic echocardiography showed cardiac tamponade with features of left ventricular free‑wall rupture (Figure 1H). Cardiopulmonary resuscitation was immediately initiated and pericardiocentesis involving aspiration of 500 ml of blood was performed. Unfortunately, it was not effective due to persistent active bleeding. Despite intensive treatment, a lack of sufficient hemodynamic response was observed, and the patient died.
Patients with TTS are at a risk of recurrence. According to the GEIST (German‑Italian‑Spanish Takotsubo) registry,4 the recurrence rate was 4%, and pulmonary edema was more frequent in the recurrence group (13.3% vs 4.9%; P = 0.04). Most recurrences occur within 5 years of the index TTS episode.4 Although rare, left ventricular rupture is the most serious complication of TTS, associated with an extremely high risk of death. In a recent systematic review, 35 such cases have been reported.5 To our knowledge, this is the first report of left ventricular rupture in an individual with recurrent TTS.
Patients with recurrent TTS might be at a risk of death due to left ventricular rupture in the region of recurrent myocardial necrosis.
- Ghadri JR, Wittstein IS, Prasad A, et al. International expert consensus document on takotsubo syndrome (part I): clinical characteristics, diagnostic criteria, and pathophysiology. Eur Heart J. 2018; 39: 2032‑2046. | Crossref
- Schneider B, Athanasiadis A, Schwab J, et al. Complications in the clinical course of takotsubo cardiomyopathy. Int J Cardiol. 2014; 176: 199‑205. | Crossref
- Stępień K, Nowak K, Karcińska A, et al. Coronary slow‑flow phenomenon in takotsubo syndrome: the prevalence, clinical determinants, and long‑term prognostic impact. Int J Mol Sci. 2024; 25: 1297. | Crossref
- El‑Battrawy I, Santoro F, Stiermaier T, et al. Incidence and clinical impact of recurrent takotsubo syndrome: results from the GEIST registry. J Am Heart Assoc. 2019; 8: e010753. | Crossref
- Zalewska‑Adamiec M, Bachórzewska‑Gajewska H, Dobrzycki S. Cardiac rupture – the most serious complication of takotsubo syndrome: a series of five cases and a systematic review. J Clin Med. 2021; 10: 1066. | Crossref
ARTICLE INFORMATION