Bloodless, lytic-free, large-bore mechanical thrombectomy for the treatment of acute pulmonary embolism: the first Polish experience with the FlowTriever system
1,3



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Bloodless, lytic-free, large-bore mechanical thrombectomy for the treatment of acute pulmonary embolism: the first Polish experience with the FlowTriever system
Catheter‑directed mechanical thrombectomy (CDMT) is an emerging therapeutic option for patients with severe acute pulmonary embolism (PE). It can provide immediate clinical and hemodynamic stabilization and has a favorable safety profile.1-3 The recently introduced FlowTriever system, equipped with large‑bore catheters (Triever16, Inari Medical Inc, California, United States), 20 and 24 French [F]) and a large‑bore aspiration syringe, enables rapid evacuation of obstructive clots. It features a unique FlowSaver Blood Return System designed to reduce blood loss by filtering the aspirated blood from thrombi prior to its reinfusion into the patient. The efficacy and safety of the FlowTriever system have been shown in a registry study.4
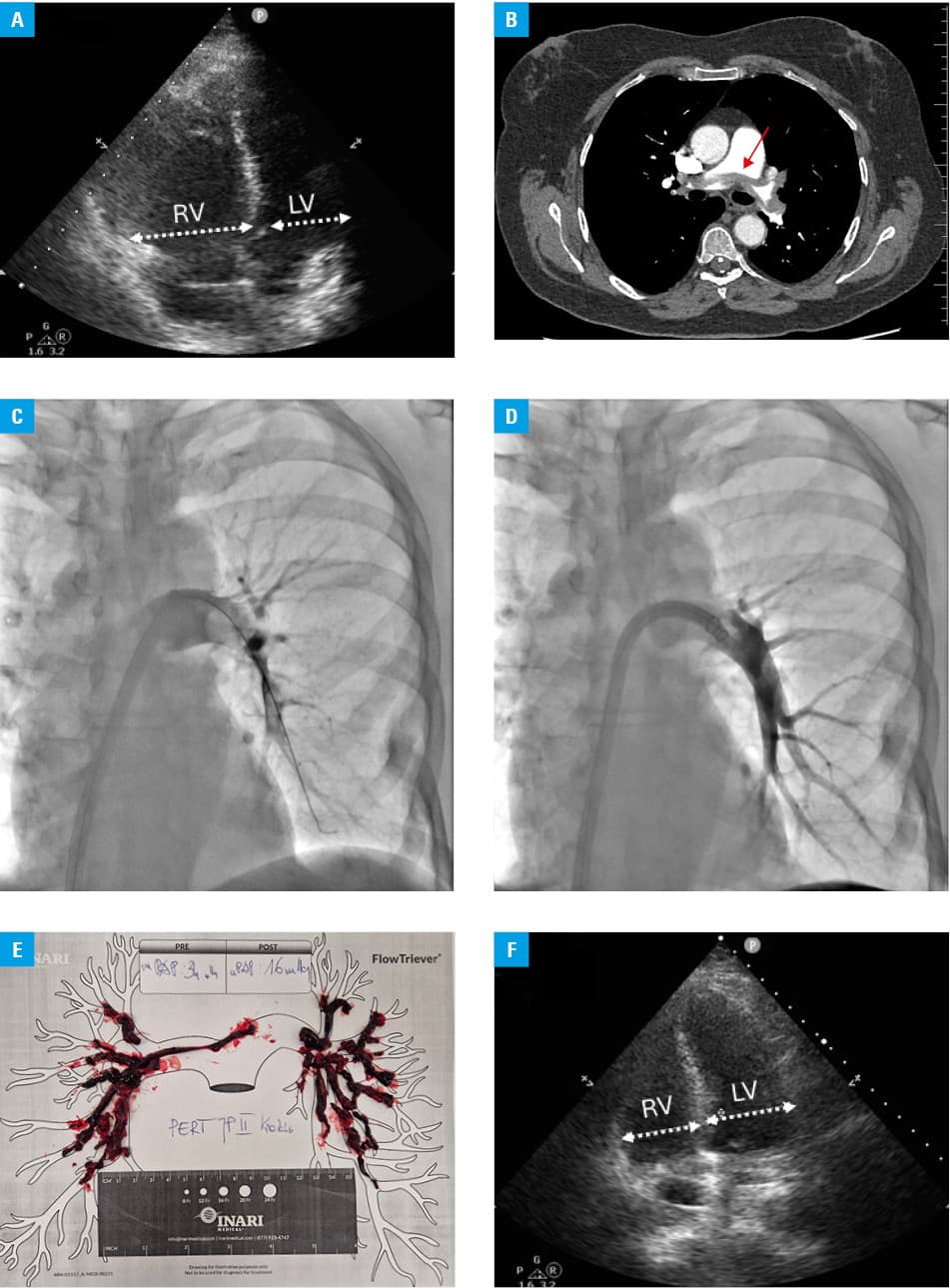
We report a case of a 61‑year‑old woman who experienced acute PE after being immobilized due to a left knee injury. She was transferred from a peripheral hospital with progressive dyspnea, chest pain, and dizziness despite 2 days of anticoagulation with 1 mg/kg subcutaneous enoxaparin twice daily. On admission, she was normotensive (140/100 mm Hg) with a heart rate of 90 bpm on a β-blocker, 5 mg bisoprolol, which had been unnecessarily administered in the peripheral hospital in response to initial tachycardia of 120–130 bpm, and was stopped immediately on admission to our center. Her oxygen saturation was 88% on room air, rising to 95% with supplemental oxygen at 3 l/min. Echocardiography showed right ventricular (RV) overload with a RV‑to‑left ventricular (RV/LV) ratio of 1.35 (Figure 1A). Computed tomography pulmonary angiography showed PE with a saddle thrombus and bilateral proximal clot masses (Figure 1B). An elevated level of cardiac troponin T was also detected (104 ng/l, reference range <14 ng/l). Given the persistence of symptoms, ongoing RV overload, and significant proximal clot burden, the pulmonary embolism response team (PERT) decided to proceed with a catheter‑directed reperfusion intervention using the FlowTriever system. The procedure was performed via the right femoral vein, using a dedicated 24‑F introducer and Triever24 and 16 catheters (Figure 1C and 1D). Large clots were sequentially removed from the right and left pulmonary arteries (Figure 1E), and the filtered blood was reinfused into the patient, leading to a minimal blood loss of less than 50 ml. The fluoroscopy time was 25 minutes, which was shorter than the median time (35 minutes) for the other CDMT systems used in our center. There was a significant reduction in the right atrial pressure (from 12 to 2 mm Hg) and mean pulmonary arterial pressure (from 34 to 16 mm Hg), with an increase in the cardiac index from 1.96 to 2.26 l/min/m2. The patient experienced symptom relief, increase in oxygen saturation to 95%, and normalization of the RV function immediately after the procedure (Figure 1F). Direct oral anticoagulant treatment was initiated on the first postoperative day, and the patient was discharged home on postoperative day 4 in a good clinical condition, without any exercise limitation.
This report describes the first use of the FlowTriever in Poland. We demonstrated that this system is a highly effective treatment option for severe PE. As compared with other CDMT systems, the FlowTriever facilitates highly controllable removal of large obstructive clots with minimal blood loss. Contacting the local PERT may help qualify a patient for such a procedure.
- Kopeć G, Araszkiewicz A, Kurzyna M, et al. Role of catheter‑directed therapies in the treatment of acute pulmonary embolism. Expert opinion of the Polish PERT Initiative, Working Group on Pulmonary Circulation, Association of Cardiovascular Interventions, and Association of Intensive Cardiac Care of the Polish Cardiac Society. Kardiol Pol. 2023; 81: 423‑440. | Crossref
- Sławek‑Szmyt S, Stępniewski J, Kurzyna M, et al. Catheter‑directed mechanical aspiration thrombectomy in a real‑world pulmonary embolism population: a multicenter registry. Eur Heart J Acute Cardiovasc Care. 2023; 12: 584‑593. | Crossref
- Stępniewski J, Magoń W, Podolec P, Kopeć G. The PENUMBRA Lightning 12 system for treatment of acute intermediate‑high pulmonary embolism. Initial experience in Pulmonary Circulation Center Krakow, Poland. Postepy Kardiol Interwencyjnej. 2022; 18: 314‑316. | Crossref
- Toma C, Bunte MC, Cho KH, et al. Percutaneous mechanical thrombectomy in a real‑world pulmonary embolism population: interim results of the FLASH registry. Catheter Cardiovasc Interv. 2022; 99: 1345‑1355. | Crossref
ARTICLE INFORMATION