Three fatal consequences of one guiding catheter maneuver during primary percutaneous angioplasty in ST-segment elevation myocardial infarction

 CC BY 4.0
CC BY 4.0
Three fatal consequences of one guiding catheter maneuver during primary percutaneous angioplasty in ST-segment elevation myocardial infarction
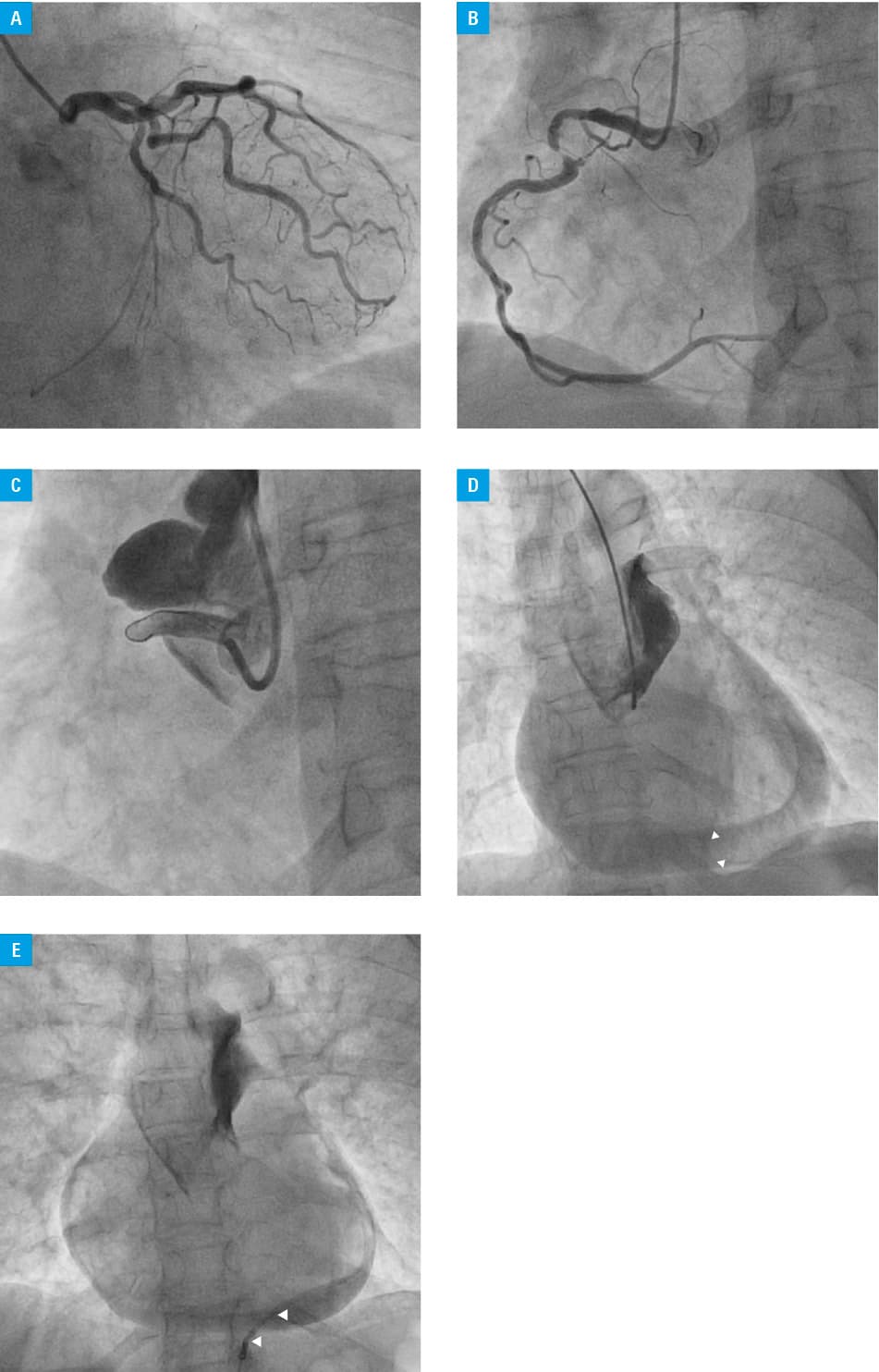
A 69‑year‑old woman with no previous history of coronary artery disease was admitted to an emergency department due to severe chest pain. Owing to ST‑segment elevation present in the II, III, and aVF leads, the patient was qualified for immediate coronary angiography, which showed no significant lesions in the left coronary artery (Figure 1A), and a subtotal (95%) stenosis in the middle segment of the right coronary artery (RCA) with (TIMI) 3 flow (Figure 1B). Due to a tortuous course of the RCA, a 6F Amplatz AL 1.0 guiding catheter (Medtronic, Minneapolis, Minnesota, United States) was chosen to provide sufficient support. After delivering the catheter to the RCA, initial contrast administration exposed a severe, extensive dissection and total occlusion of the RCA with TIMI 0 flow (Figure 1C). The dissection could not be passed either with Balanced Middleweight or Whisper MS guide wires (Abbott Cardiovascular, Plymouth, Massachusetts, United States). The patient developed cardiogenic shock caused by the aortic dissection as well as cardiac tamponade confirmed on angiography (Figure 1D). Pericardiocentesis and drainage of 100 ml of blood (Figure 1E) restored hemodynamic stability. Percutaneous coronary intervention was not continued, and the patient was transferred to an intensive care unit. Her condition gradually worsened despite vasopressor infusion. Due to hemodynamic instability, a transfer to a cardiac surgery center was impossible, and the patient was disqualified after a consultation. Subsequent echocardiography showed severely hypokinetic right ventricle and no significant tamponade. After several hours, cardiac arrest occurred as a consequence of pulseless electrical activity, followed by asystole, which led to the patient’s death despite resuscitation.
Coronary artery tortuosity is one of the factors significantly impeding percutaneous coronary interventions, and it is most commonly associated with the lesion location in the RCA,1 which is also the most common infarct artery in patients with ST‑segment elevation myocardial infarction (STEMI), both in multivessel disease2 and in general.3 Maintained flow in STEMI caused by a culprit lesion in the RCA is not associated with a better long‑term outcome in comparison with a totally occluded artery.3 Intervention difficulties in a tortuous artery can be overcome by applying a catheter that provides sufficient support; however, such catheters are also associated with a greater risk for iatrogenic vascular complications,4 which, as in this case, can be fatal. Nonetheless, urgent revascularization in STEMI is crucial,5 therefore such a risk is acceptable.
- Konigstein M, Ben‑Yehuda O, Redfors B, et al. Impact of coronary artery tortuosity on outcomes following stenting: a pooled analysis from 6 trials. JACC Cardiovasc Interv. 2021; 14: 1009‑1018. | Crossref
- Sadowski M, Milewski K, Zandecki Ł, et al. Revascularization in patients with ST‑segment elevation myocardial infarction and multivessel coronary artery disease: preliminary results from a large multicenter national registry. Pol Arch Intern Med. 2022; 132: 16315. | Crossref
- Karwowski J, Gierlotka M, Gąsior M, et al. Relationship between infarct artery location, acute total coronary occlusion, and mortality in STEMI and NSTEMI patients. Pol Arch Intern Med. 2017; 127: 401‑411. | Crossref
- Ramasamy A, Bajaj R, Jones DA, et al. Iatrogenic catheter‑induced ostial coronary artery dissections: Prevalence, management, and mortality from a cohort of 55,968 patients over 10 years. Catheter Cardiovasc Interv. 2021; 98: 649‑655. | Crossref
- O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST‑elevation myocardial infarction: a report of the American College of Cardiology Foundation / American Heart Association Task Force on Practice Guidelines. Circulation. 2013; 127: e362‑e425.
ARTICLE INFORMATION