Unexpected treatment outcomes in a patient with metastatic melanoma and immune-related hemophagocytic lymphohistiocytosis

 CC BY 4.0
CC BY 4.0
Unexpected treatment outcomes in a patient with metastatic melanoma and immune-related hemophagocytic lymphohistiocytosis
A 58‑year‑old woman presented at the National Research Institute of Oncology, Kraków, with BRAF‑positive cutaneous melanoma metastasized to the throat, lymph nodes, spleen, adrenal gland, and subcutaneous tissue. She received her first dose of immune checkpoint inhibitors (ICIs), ipilimumab and nivolumab, on June 1, 2022.
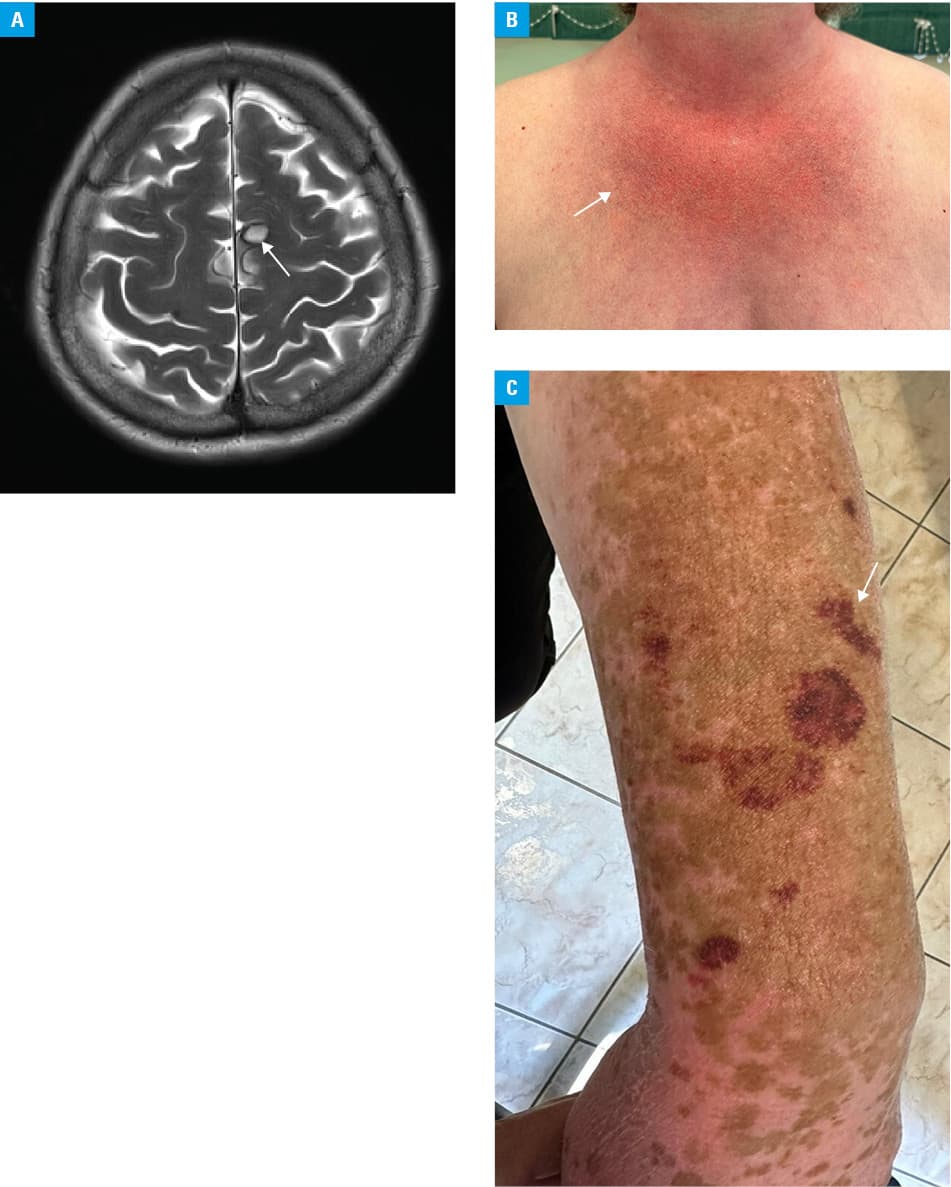
On June 30, the patient reported dysphagia and fever of 38.5 °C. Physical examination showed jaundice, peripheral edema, and new palpable lesions in the subcutaneous tissue. Laboratory tests indicated liver dysfunction, with ferritin concentration of 2266.7 ng/ml (reference range [RR], 11–282.5 ng/ml) and low fibrinogen concentration of 1.1 g/l (RR, 1.8–3.5 g/l). Abdominal ultrasound showed dilated bile ducts and thickened gallbladder walls. Endoscopic retrograde cholangiopancreatography excluded mechanical obstruction. Brain magnetic resonance imaging showed new metastases (Figure 1A). Given the patient’s deteriorating clinical condition, pseudoprogression was unlikely and true disease progression was assumed.1
During hospitalization, the patient developed purpura, gastrointestinal bleeding, stupor, rising bilirubin, and pancytopenia with hemoglobin level of 7.5 g/dl (RR, 12–16 g/dl), platelet count of 23 × 109/l (RR, 150–400 × 109/l), and neutrophil count of 0 × 109/l (RR, 2.2–7 × 109/l), meeting the 2004 hemophagocytic lymphohistiocytosis (HLH) diagnostic criteria2 (fever, splenomegaly, cytopenia, hypofibrinogenemia, elevated ferritin levels). She received high doses of prednisone, mycophenolate mofetil, cyclophosphamide, followed by etoposide, cyclosporine, antibiotics, blood transfusions, and febrile neutropenia prophylaxis without clinical improvement. After a month‑long hospital stay, with escalating total bilirubin levels up to 413.5 µmol/l (RR, 2–21 µmol/l) disqualifying her from further oncological treatment, the patient was transferred to a palliative medicine unit.
In September 2023, the patient unexpectedly presented at the Institute. She was discharged from the palliative care unit after 2‑month hospitalization, with decreasing total bilirubin levels and clinical improvement. After being lost to follow‑up, she continued mycophenolate mofetil for up to 3 months prior to the visit, along with 20 mg of prednisone per day. Physical examination revealed phototoxicity on her face and neck, and melanocytic lesions on her forearm (Figure 1B and 1C), which were confirmed through a skin biopsy as lentigo and drug‑related changes. Her laboratory tests remained within reference range. Follow‑up computed tomography scans since then have showed a partial response, with no apparent lesions in the brain.
Treatment with combined ICIs such as ipilimumab and nivolumab, which are antibodies targeting cytotoxic T‑lymphocyte–associated antigen 4 and programmed cell death protein 1, respectively, was found to improve outcomes in the first‑line treatment of metastatic melanoma.3 However, since ICIs eliminate the inhibitory mechanisms that regulate T‑cell activity, there is a potential for increased immune activation and subsequent immune‑related adverse events (irAEs). Consequently, the toxicity associated with ICIs seems to intersect with the dysregulated immune activation observed in HLH.4 Management of such complications remains challenging due to the absence of specific diagnostic criteria and treatment recommendations, leading to underrecognition and high mortality rates.5
Physicians of various specialties managing patients with ICIs‑induced irAEs should be aware that these complications can be unpredictable and prolonged. Despite their severity, they may be associated with improved treatment outcomes and unexpectedly long survival even in patients with a high cancer burden.5
- Pałucki J, Kucharz J. Response assessment in cancer immunotherapy. Cooperation between the oncologist and the radiologist. Oncol Clin Pract. 2022; 18: 119‑127. | Crossref
- Machowicz R, Basak G. How can an internal medicine specialist save a patient with hemophagocytic lymphohistiocytosis (HLH)? Pol Arch Intern Med. 2020; 130: 431‑437. | Crossref
- Wolchok JD, Chiarion‑Sileni V, Gonzalez R, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Eng J Med. 2017; 377: 1345‑1356. | Crossref
- Noseda R, Bertoli R, Müller L, Ceschi A. Haemophagocytic lymphohistiocytosis in patients treated with immune checkpoint inhibitors: analysis of WHO global database of individual case safety reports. J Immunother Cancer. 2019; 7: 117. | Crossref
- Liu LL, Skribek M, Harmenberg U, Gerling M. Systemic inflammatory syndromes as life‑threatening side effects of immune checkpoint inhibitors: case report and systematic review of the literature. J Immunother Cancer. 2023; 11: e005841. | Crossref
ARTICLE INFORMATION