Measurement of lipoprotein(a) levels in real-world clinical and laboratory settings: a single-center experience

 CC BY 4.0
CC BY 4.0
Measurement of lipoprotein(a) levels in real-world clinical and laboratory settings: a single-center experience
Introduction
Lipoprotein(a) (Lp[a]) is composed of a low‑density lipoprotein (LDL) particle in which apolipoprotein (apo) B‑100 is bound to highly polymorphic apo(a). It is a well‑established risk factor for premature atherosclerotic vascular disease, particularly multivessel coronary artery disease (CAD), myocardial infarction (MI), ischemic stroke, and aortic valve stenosis (AVS).1-3 Plasma Lp(a) concentrations vary from below 0.1 mg/dl to over 300 mg/dl (<0.2–750 nmol/l, respectively), and are predominantly (>90%) genetically determined. Based on that, it has been recommended that the Lp(a) level should be measured once in a lifetime the general population. Approximately 20% of adult individuals, also in Poland,1 have Lp(a) concentrations exceeding 50 mg/dl, which represents a cardiovascular risk factor in Europe, although targeted Lp(a)-reducing therapy is currently unavailable.4
Despite guideline recommendations,5 Lp(a) levels are still not commonly determined.6 The European Atherosclerosis Society survey showed that 75.5% of 151 clinicians working in specialist lipidology clinics declared a routine measurement of Lp(a) levels in clinical practice.7 Of the clinicians working in Western Europe, approximately 90% stated that they routinely ordered Lp(a) level measurements; however, among those working in Central and Eastern Europe, this rate approached only 50%.7 It is unclear how often Lp(a) level measurements are currently requested in hospital and outpatient settings in European countries.
Despite growing awareness of the importance of Lp(a), little is known about everyday practice and indications for measuring this risk factor in Poland. Therefore, we evaluated the temporal changes in requests for Lp(a) level measurements in a tertiary cardiovascular center.
Patients and methods
We retrospectively assessed all consecutive Lp(a) level measurements performed in a tertiary cardiovascular center, St. John Paul II Hospital in Kraków, Poland, since 2017, when testing on a 24/7 basis became available in accordance with the 2016 European guidelines on cardiovascular disease prevention.8 We included measurements performed in hospitalized or ambulatory patients from January 2017 to June 2024. Measurements performed for scientific purposes were excluded.
Demographic and clinical data of all patients who underwent Lp(a) level evaluation were retrieved from the hospital database. As this study was part of routine clinical workup, approval of the Bioethical Committee was not required.
The indications for Lp(a) level measurements were CAD, ischemic stroke, peripheral arterial disease (PAD), family history of CAD, venous thromboembolism (VTE), AVS, and other conditions (retinal vein occlusion, myocarditis, cerebral venous thrombosis, autoimmune diseases).
Serum Lp(a) levels were determined using an immunoturbidimetric assay with an analytical measurement range of 5 to 112 mg/dl (7–240 nmol/l) (Roche Diagnostics, Mannheim, Germany). If the Lp(a) levels exceeded the upper limit of the measurement range, a 3‑fold automatic dilution was performed. Lipid profile parameters were analyzed using an enzymatic colorimetric assay (Roche Diagnostics).
To determine the LPA gene variant, samples were genotyped using a TaqMan SNP assay (rs3798220, Applied Biosystems, ThermoFisher Scientific, Foster City, California, United States) on the QuantStudio Dx Real‑Time PCR Instrument (ThermoFisher Scientific).
Statistical analysis
Variables were presented as numbers and percentages, mean with SD or median with interquartile range (IQR), as appropriate. Normality was assessed with the Shapiro–Wilk test. The Levene test was used to assess equality of variances. Differences between 2 groups were tested using the t test or the Mann–Whitney test, depending on data distribution. Categorical variables were compared by the Pearson χ2 test or the Fisher exact test. The Spearman or Pearson correlation coefficients were used for nonnormally and normally distributed variables, respectively. Differences between more than 2 groups were compared using the analysis of variance or Kruskal–Wallis test. A P value below 0.05 was considered significant. The Mann–Kendall test was used to analyze the trend in the occurrence of premature atherosclerotic vascular disease over the study period. Statistical analyses were performed with the R‑4.4.1 package (R Foundation for Statistical Computing, Vienna, Austria).
Results
Number of lipoprotein(a) measurements
A total of 2822 consecutive Lp(a) measurements were performed in 2637 patients (1142 women [43.31%] and 1495 men [56.69%]) during the study period. Most patients underwent testing only once (n = 2469 [93.62%]), while 153 individuals (5.8%) had 2 measurements performed, 13 (0.49%) were assessed 3 times, and 2 (0.08%) were tested 4 times.
As shown in Figure 1A, Lp(a) level measurements were performed 47 times in 2017 (1.68% of all measurements), with the measurement frequency showing a tendency to increase in the subsequent years (increase by 257% in 2018 vs 2017; P <0.001). In 2020, due to the COVID‑19 pandemic, the number of measurements decreased by 20% (as compared with 2019), and remained at a similar level in 2021. In 2022, the number of tests increased approximately 1.5‑fold as compared with 2019, exceeding the prepandemic levels.
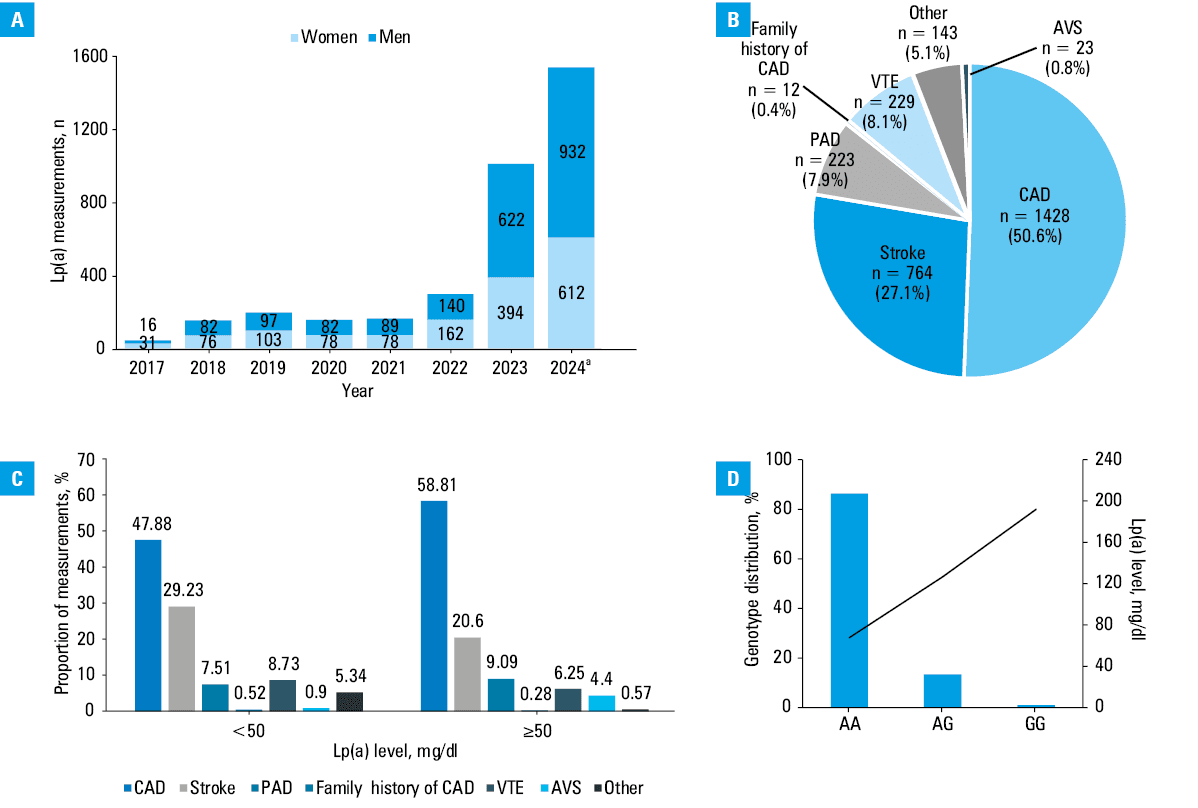
Abbreviations: AVS, aortic valve stenosis; CAD, coronary artery disease; PAD, peripheral artery disease; VTE, venous thromboembolism
The median (IQR) age of the patients undergoing Lp(a) level measurement was 55 (44–65) years, with an increase in specific years (P <0.001). There were no significant sex‑related differences with respect to the Lp(a) level. The largest age subgroup comprised patients younger than 50 years (n = 1075 [38.1%]), while as few as 387 individuals (13.7%) were aged 70 years or above. The youngest patient tested was a 6‑year‑old boy with ischemic stroke, while the oldest one was a 93‑year‑old man with CAD.
Blood samples for Lp(a) level measurements were obtained mostly from outpatients (n = 2119 [75.1%]) at a median (IQR) age of 52 (42–61.5) years, with a predominance of men (n = 1112 [52.5%]). Women were tested more frequently in 2017, 2019, 2021, and 2022. As expected, most of the measurements were performed in outpatients treated at cardiology clinics (n = 1988 [93.8%]). Among the hospitalized patients (n = 703 [24.9%]), a majority of Lp(a) level measurements were requested by physicians working at cardiology departments (n = 670 [95.3%]).
The indications for Lp(a) level assessment are shown in Figure 1B. The measurements were performed most often in patients with CAD (n = 1428 [50.6%]), followed by those with ischemic stroke (n = 764 [27.1%]), VTE (n = 229 [8.1%]), PAD (n = 223 [7.9%]), AVS (n = 23 [0.8%]), family history of CAD (n = 12 [0.4%]) and other conditions (n = 143 [5.1%]). Interestingly, the number of samples from ischemic stroke patients tended to increase (26 in 2017, about 90 in 2018–2022, and about 150 in 2022–2024).
Among the patients undergoing Lp(a) level assessment, a significant increase in the share of CAD cases was observed in women under 65 years and men under 45 years (P = 0.03 and P = 0.01, respectively).
Additionally, among the individuals younger than 55 years, a nonsignificant upward trend in CAD as the indication for Lp(a) measurement was noted (P = 0.06).
Lipoprotein(a) levels
The median (IQR) Lp(a) level was 9.7 (4–49.35) mg/dl, without any associations with age or sex. However, higher Lp(a) levels were noted in the samples derived from women over 50 years than in the samples derived from men of the same age (median [IQR], 12.9 [3.6–62.4] mg/dl vs 10.1 [5.3–48.6] mg/dl; P <0.001).
Serum Lp(a) levels greater than or equal to 50 mg/dl, considered a threshold for increased cardiovascular risk,2,4 were noted in 704 samples (24.95%). In this subgroup, the median (IQR) Lp(a) level was 95.8 (74.45–128.55) mg/dl, with a higher proportion of samples derived from men (57%). The patients with Lp(a) levels greater than or equal to 50 mg/dl were older than those with the Lp(a) level below 50 mg/dl (median [IQR] age, 56 [46–65] vs 54 [43–64] years; P = 0.02) and had a higher prevalence of CAD (P <0.001). The patients with stroke and VTE were more prevalent in the group with Lp(a) levels below 50 mg/dl (P <0.001 and P = 0.36, respectively) (Figure 1C).
A total of 312 measurements (11.06%) yielded Lp(a) levels exceeding 100 mg/dl. There were no sex‑related differences, and most of these patients (66%) had CAD. The median patient age in this group was higher than in the groups with Lp(a) levels between 50 and 100 mg/dl and below 50 mg/dl (median [IQR], 57 [48–67] vs 54 [44–63] and 54 [43–64] years, respectively; P <0.001). Lipid profiles did not differ between the above subgroups. No significant correlations between lipid profiles and Lp(a) levels were found.
Genetic testing
A total of 562 patients (21.3%), mostly individuals with Lp(a) levels greater than or equal to 50 mg/dl treated at cardiology outpatient clinics (n = 514 [91.45%]), were genotyped since 2022, when the test was introduced (n = 153 [27.2%] in 2024). The largest proportion of those were patients with CAD (n = 371 [66%]), followed by 99 individuals (17.6%) with stroke. The genotype distribution of LPA c.5673A>G variants was as follows: AA, 485 (86.3%); AG, 75 (13.35%); and GG, 2 (0.36%). Among the c.5673G allele carriers, the median (IQR) Lp(a) levels were 10‑fold higher than in the wild‑type carriers (AA, 10.7 [4.4–64.7] mg/dl vs AG+GG, 127.4 [90–161.1] mg/dl; P <0.001) (Figure 1D). Among the 102 patients with Lp(a) levels exceeding 100 mg/dl, the heterozygous LPA AG variant was detected in 52 individuals (49%), and a homozygous GG variant was detected in 2 patients with CAD (a 46‑year‑old woman and a 55‑year‑old man).
Discussion
To our best knowledge, this is the largest European study showing real‑life indications and temporal changes for Lp(a) level measurements performed over the last 7 years in a tertiary hospital specialized in cardiovascular disease care. We found that the frequency of Lp(a) testing had been rapidly increasing in recent years, with a 5‑fold increase from 2018 to 2024, most likely due to ongoing randomized trials that evaluate new Lp(a)-lowering therapies.9,10 A similar observation was reported by other authors.11-14
Regarding the indications for Lp(a) testing,14 individuals with CAD and ischemic stroke prevailed, while PAD and VTE were less prevalent indications. The number of samples derived from patients following ischemic stroke increased from 2022, which is related to the emerging evidence for the role of Lp(a) in stroke of unknown causes. This aligns with findings from the United States, where the Lp(a) tests were more common among patients without a prior history of atherosclerotic cardiovascular disease (24.3%), including those with ischemic stroke (44.8%), followed by individuals with MI (41.1%) and PAD (27.3%).14 Surprisingly, in our study, patients with PAD were rarely tested for Lp(a), with no increase in the measurement frequency over time. This finding highlights the need for initiatives aimed at enhancing vascular surgeons’ awareness of the clinical relevance of Lp(a) level measurement, especially in younger patients.
The observed median Lp(a) levels (9.7 mg/dl) were similar to those reported in other studies on Central European cohorts, for example, the SpecialisT cARe patients (STAR)-Lp(a) cross‑sectional study (8.5 mg/dl)15 or the Zabrze‑Lip(a)Registry study (6.6 mg/dl).16 Similarly to the study by Konieczyńska et al,1 we observed higher Lp(a) levels in samples derived from women older than 50 years, which may be explained by the impact of menopause.17
We did not find any correlation of Lp(a) with lipid profiles; however, data on this topic are inconsistent.1,15,16 Burzyńska et al15 showed that total cholesterol, LDL cholesterol, and the triglyceride to high‑density lipoprotein cholesterol ratio were related to the Lp(a) level but patients with CAD were excluded from this study. In the Zabrze‑Lip(a) Registry reports covering patients at a very high cardiovascular risk, no association of Lp(a) with lipid profiles was found.16 It is likely that statin therapy affects the results; both our study population and the cohort from Zabrze included patients on lipid‑lowering therapy.16,18
Our genetic data were in line with previous reports, where the rs3798220 variant was associated with higher Lp(a) levels.4,19 It is unclear whether genetic testing could influence prognosis or impact efficacy of future therapies.
Our study has several limitations. Firstly, it was a retrospective, single‑center study and our data cannot be extrapolated to multispecialty hospitals. Temporal changes in Lp(a) level variability have been noted recently20; however, this issue was beyond the scope of the current study. Finally, information about other comorbidities or pharmacotherapy was not collected; however, most medications, including statins, have no effect on the Lp(a) level.9
Conclusions
The frequency of Lp(a) testing was low but increased significantly over 7 years. The source of this increase may be multifactorial, including new guideline recommendations, broader education, clinician awareness, and preventive programs. However, our real‑life experience suggests that Lp(a) testing is still not requested frequently enough and should particularly be prioritized in patients with multivessel disease and PAD. Currently, no targeted therapies are available for lowering Lp(a) levels; therefore, it is essential for elevated Lp(a) concentrations to prompt preventive strategies, which may include lifestyle modifications, management of diabetes and hypertension, and efforts to reduce cholesterol levels.
- Konieczyńska M, Nowak K, Pudło J, et al. Elevated lipoprotein(a) in the middle‑aged Polish population: preliminary data on the genetic background. Kardiol Pol. 2023; 81: 1279‑1281. | Crossref
- Wilson DP, Jacobson TA, Jones PH, et al. Use of lipoprotein(a) in clinical practice: a biomarker whose time has come. A scientific statement from the National Lipid Association. J Clin Lipidol. 2019; 13: 374‑392. | Crossref
- Kopytek M, Ząbczyk M, Mazur P, et al. Oxidized phospholipids associated with lipoprotein(a) contribute to hypofibrinolysis in severe aortic stenosis. Pol Arch Intern Med. 2022; 132: 16372. | Crossref
- Kronenberg F, Mora S, Stroes ESG, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J. 2022; 43: 3925‑3946. | Crossref
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020; 41: 111‑188.
ARTICLE INFORMATION