Asymptomatic retroperitoneal ganglioneuroma adjacent to the abdominal organs and large abdominal vessels

 CC BY 4.0
CC BY 4.0
Asymptomatic retroperitoneal ganglioneuroma adjacent to the abdominal organs and large abdominal vessels
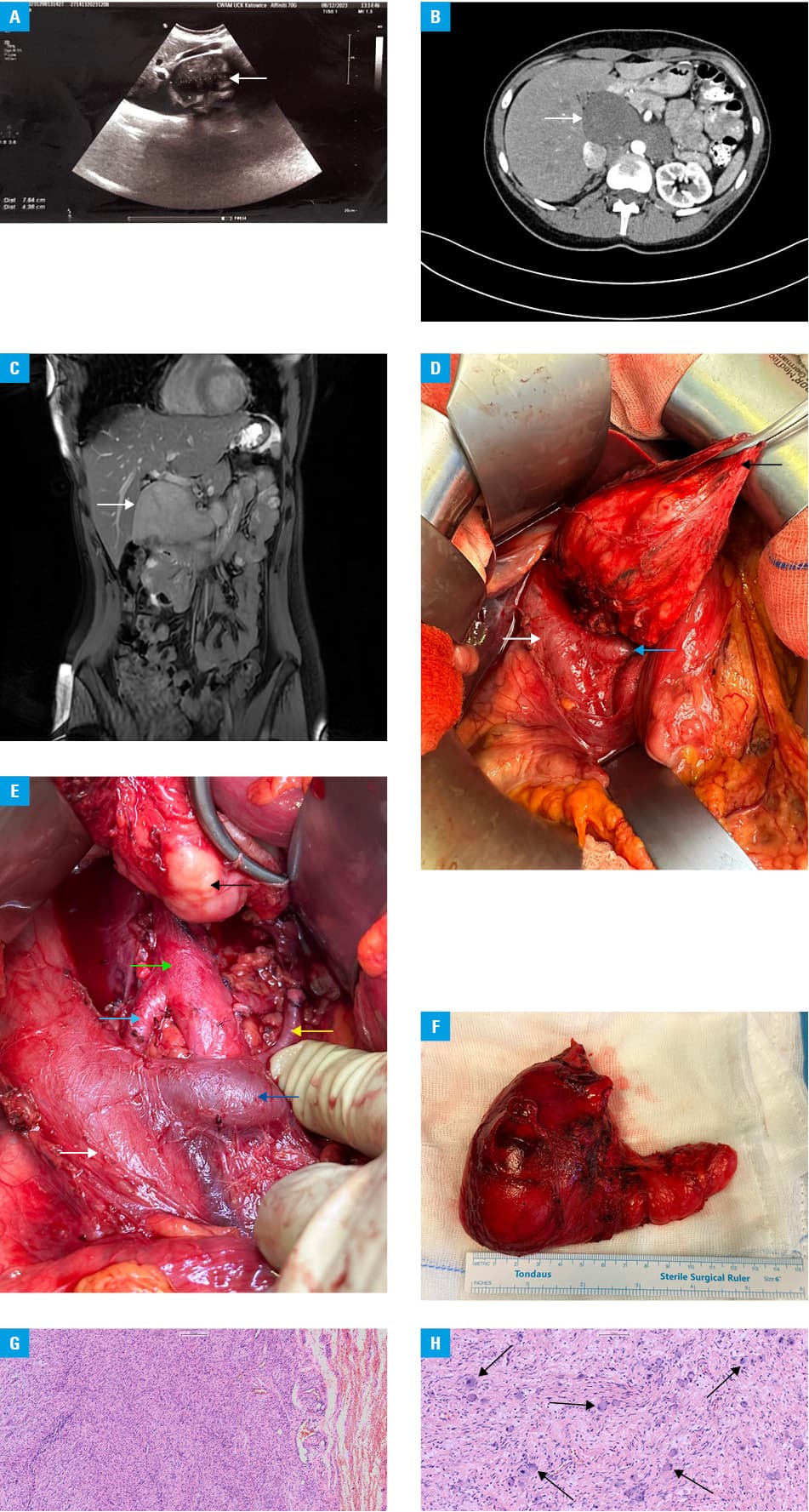
A 22‑year‑old woman was admitted to a hospital for diagnostics of a large mass (76.4 mm × 43.8 mm) found incidentally on abdominal ultrasound in the perihepatic space (Figure 1A). The patient was asymptomatic. Her physical examination (excluding the palpable mass) and laboratory tests were normal. Her family history was negative for malignancy. Contrast‑enhanced computed tomography (CECT) showed a well‑circumscribed hypodense retroperitoneal tumor (102 mm × 52 mm × 70 mm) extending from the hepatic hilum to the left adrenal gland (Figure 1B). On the T1‑weighted sequence of CE magnetic resonance imaging (MRI), the tumor was almost homogeneous, slightly hyperintense in the central part, and on T2‑weighted sequences it was heterogeneous with areas of hyperintense signal. The mass adhered to the posterior pancreas, stomach, liver, common bile duct (with its compression), gallbladder, and large abdominal arteries (abdominal aorta, superior mesenteric artery, right renal artery) and veins (inferior vena cava [with its compression], portal vein and splenic vein [with splenomesenteric confluent narrowing], and left renal vein). It displaced the pancreatic head and duodenum to the left and the left suprarenal gland to the posterior space of the retroperitoneum (Figure 1C). Further diagnostics included gastroduodenoscopy, which showed an impression in the wall of the stomach caused by the tumor. Ultrasound‑guided biopsy was inconclusive. Laparotomy was performed. The abovementioned close tumor adherence to the abdominal organs and large vessels was intraoperatively confirmed (Figure 1D and 1E). The tumor was carefully dissected and separated from all adjacent structures, and radical complete tumor resection (R0 resection) was performed (Figure 1F). The postoperative course was uneventful, and the patient was discharged on the seventh day without any complications. Pathologic examination showed a greyish, solid, and elastic tumor measuring 105 mm × 95 mm × 55 mm. The histopathological report (slide scanner Leica Aperio GT‑450DX, Deer Park, Illinois, United States) confirmed ganglioneuroma (GN; Figure 1G and 1H). There were no signs of the tumor recurrence during 6 months of follow‑up.
GN is a benign neuroectodermal neoplasm, mainly seen in children and young adults, with a predilection for women.1,2 It is found along the distribution sites of the sympathetic nervous system, particularly in the posterior mediastinum and retroperitoneum.2 GN is extremely rare. Its incidence is around 1 case per 1 000 000 population, and retroperitoneal GNs account for 0.72% to 1.6% of all primary retroperitoneal tumors.1 These tumors show no characteristic symptoms, they are often asymptomatic, until they grow significantly to cause mass effect; however, most of them are smaller than 10 cm and symptoms caused by mass effect are rare.2,3 The only treatment offered to the patients is a surgical excision.3
In the presented case, the tumor was asymptomatic even though it was large and adjacent to a majority of the abdominal organs, major abdominal arteries and veins, including the inferior vena cava, portal vein, and it compressed the common bile duct. Further detailed imaging investigations (CECT, MRI) enabled early surgical treatment with complete tumor resection.
This case highlights the value of abdominal ultrasound in the diagnosis of retroperitoneal solid tumors, and it shows that abdominal ultrasound is important and may be crucial in GN diagnostics and treatment, which is related to a good prognosis.
- Xiao J, Zhao Z, Li B, Zhang T. Primary retroperitoneal ganglioneuroma: a retrospective cohort study of 32 patients. Front Surg. 2021; 8: 642451. | Crossref
- Pacella G, Brunese MC, Donnarumma F, et al. Imaging of ganglioneuroma: a literature review and a rare case of cystic presentation in an adolescent girl. Diagnostics (Basel). 2023; 13: 2190. | Crossref
- Avila‑Sanchez P, Barron‑Cervantes NM, Martinez‑Esteban A, Chan‑Nuñez LC. Retroperitoneal peripancreatic ganglioneuroma encasing the celiac trunk and superior mesenteric artery. Cureus. 2024; 16: e52405. | Crossref
ARTICLE INFORMATION