Mitral valve prolapse (MVP) is the most common valvular heart defect.1 Some patients with MVP are at a risk of developing malignant ventricular arrhythmias (VAs) and sudden cardiac arrest (SCA).2 This report illustrates the clinical profile of an SCA survivor with MVP at the event and years before it to help identify such patients and consider them for active arrhythmia monitoring and preventive implantation of an implantable cardiac defibrillator (ICD).
A 34‑year‑old man was admitted to the intensive care unit after SCA due to defibrillation‑resistant ventricular fibrillation despite cardiopulmonary resuscitation starting immediately and the first defibrillation shock delivered within 10 minutes of SCA. The patient had a long history (22 years) of myxomatous MVP. Yearly checkup showed moderate mitral regurgitation (MR) and 24‑hour monitoring demonstrated low VA burden with nonsustained ventricular tachycardias (nsVTs) up to 4 beats at 200 bpm (Figure 1A). Even though the patient did not previously experience any syncope / presyncope, he complained of occasional several‑second long palpitations, which increased in frequency in the past year.
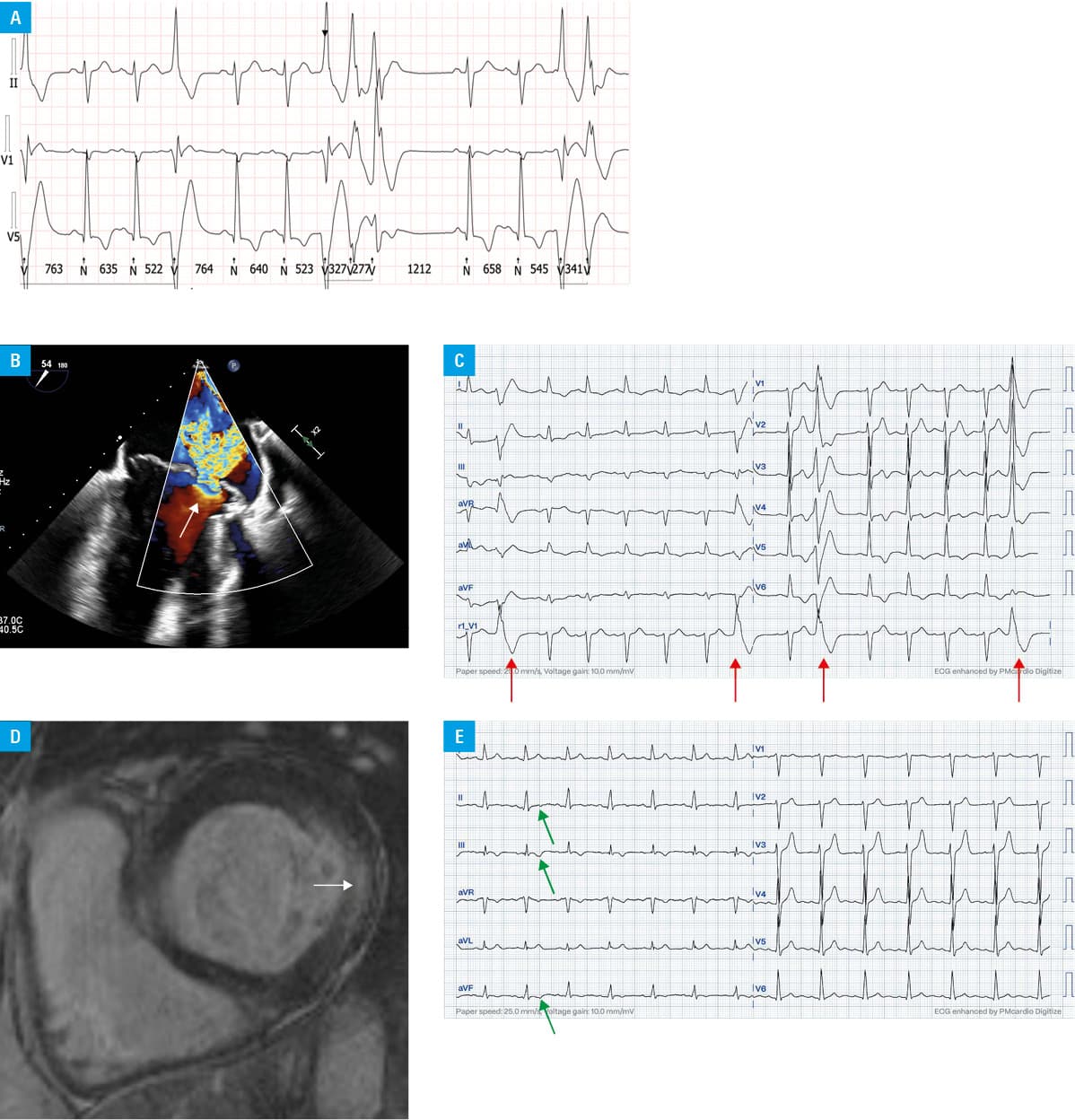
Echocardiography during hospitalization showed severe MR (Figure 1B) with prolapse of both mitral valve leaflets, left ventricular dilatation, and no wall motion abnormalities (WMAs). Coronary angiography excluded atherosclerosis. Twelve‑lead 24‑hour Holter electrocardiogram (ECG) showed 5540 premature ventricular contractions (PVCs) with right bundle branch block‑like morphology (Figure 1C) and 52 episodes of nsVTs up to 15 beats at 200 bpm within 24 hours. The ECG monitoring also registered numerous PVCs and episodes of nsVTs. Cardiac magnetic resonance (CMR) imaging demonstrated late gadolinium enhancement (LGE) in the basal segment of the inferior‑lateral and lateral‑left ventricular wall (Figure 1D), no WMAs, no mitral annular disjunction, and confirmed severe MR with prolapse of both mitral valve leaflets. A diagnosis of the arrhythmic phenotype of MVP was made. The clinical image corresponded to a disorder predisposing to VT (B0) according to the classification of rare arrhythmogenic and conduction disorders.3 The patient had a subcutaneous cardioverter‑defibrillator implanted and underwent mechanical mitral valve replacement. At 19‑month device follow‑up no VAs were detected.
According to the 2022 European Heart Rhythm Association consensus for MVP,2 the patient had documented short, fast nsVTs and at least 2 high‑risk 12‑lead ECG phenotypic features already 4 years before SCA (Figure 1E). Also, he experienced episodes of palpitations, which could be due to VAs, and which, considering his MVP, should be actively screened for by means of prolonged Holter‑ECG or even an implantable loop recorder. Furthermore, myxomatous degeneration was present along with redundant mitral valve leaflets, which put the patient at a higher risk of VAs.2 In such cases, CMR could have detected the LGE value indicative of fibrosis and severe MR—both increasing VA risk. As SCA in arrhythmic MVP is often provoked by stress or exertion,4 exercise stress testing could also be considered for VA risk evaluation.
In individuals with MVP and high‑risk features, an active search for VA and consideration of elective ICD implantation for sudden cardiac death prevention are suggested.
- Han HC, Ha FJ, Teh AW, et al. Mitral valve prolapse and sudden cardiac death: a systematic review. J Am Heart Assoc. 2018; 7: e010584. | Crossref
- Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart diseases: a population‑based study. Lancet. 2006; 368: 1005‑1011. | Crossref
- Podolec P, Baranchuk A, Brugada J, et al. Clinical classification of rare cardiac arrhythmogenic and conduction disorders, and rare arrhythmias Pol Arch Intern Med. 2019; 129: 154‑159. | Crossref
- Sabbag A, Essayagh B, Barrera JDR, et al. EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed by the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society. Europace. 2022; 24: 1981‑2003. | Crossref
ARTICLE INFORMATION