Left main percutaneous coronary angioplasty only with kissing drug-coated balloons as a treatment strategy in a young woman with active systemic lupus erythematosus and cardiogenic shock after coronary artery bypass grafting

 CC BY 4.0
CC BY 4.0
Left main percutaneous coronary angioplasty only with kissing drug-coated balloons as a treatment strategy in a young woman with active systemic lupus erythematosus and cardiogenic shock after coronary artery bypass grafting
Autoimmune diseases, such as systemic lupus erythematosus (SLE), often cause severe cardiovascular disruption, with myocardial infarction (MI) frequently being the first clinical manifestation.1 Percutaneous coronary interventions (PCIs) entail a significantly higher risk of major adverse cardiovascular events, MI, and repeated revascularization in these patients, as compared with the general population, frequently due to in‑stent restenosis.2 However, coronary artery bypass grafting (CABG) can be performed with acceptable results.3 Studies on detailed management of patients with SLE undergoing PCI are missing.
A 34‑year‑old woman with unstable angina, SLE, mixed hyperlipidemia, stage 5 chronic kidney disease requiring peritoneal dialysis, arterial hypertension with a history of MI at the age of 24 (ST‑segment elevation inferior MI), 29, and 30 (non–ST‑segment elevation MI), and numerous PCIs with drug‑eluting stent implantations was admitted for a planned CABG due to multivessel disease with 75% stenosis of the left main coronary artery (LM), 85% stenosis in the middle segment of the anterior descending artery (LAD), 90% stenosis in the ostium of the intermediate artery (IM), and 75% stenosis in the middle segment of the first obtuse marginal branch (OM‑1; in‑stent restenosis). Preoperative transthoracic echocardiography showed isolated hypokinesis of the inferior wall with preserved left ventricular (LV) ejection fraction and LV concentric hypertrophy.
Two saphenous vein bypass grafts (SVBGs) were performed to the LAD and OM‑1. The procedure was complicated by a dissection of the OM‑1 requiring suturing, resulting in no‑flow to the distal part of the artery. Hemodynamic collapse 2 days after CABG forced the insertion of an intra‑aortic balloon pump (IABP), followed by veno‑arterial extracorporeal membrane oxygenation (V‑A ECMO) on the next day. Additionally, decompression of 300 ml of pericardial effusion was performed.
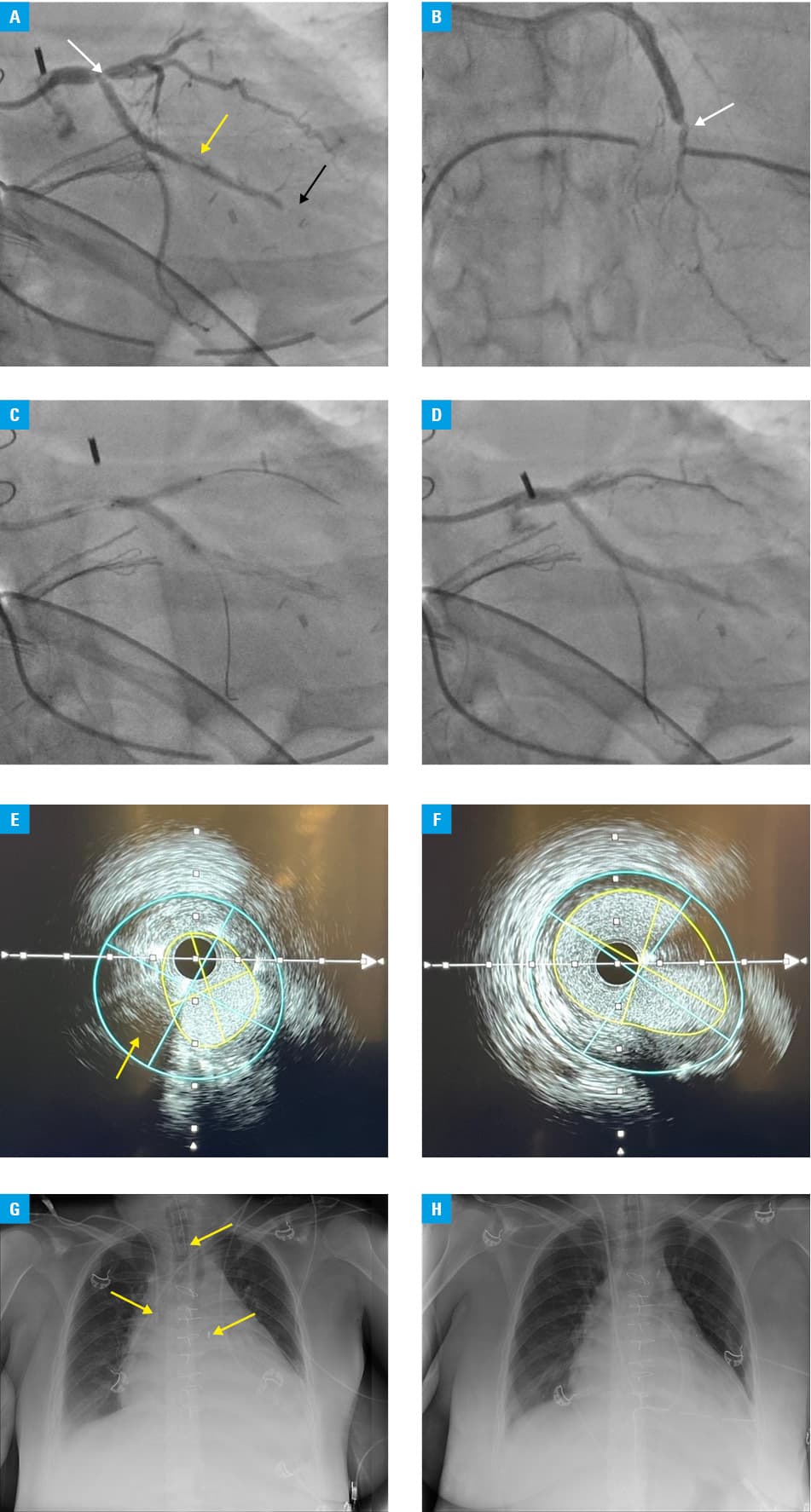
Due to unstable hemodynamic status, control coronary angiography (ultrasound‑guided left brachial access, no other vascular access available) with intravascular ultrasound (IVUS) was performed showing a fibrous atherosclerotic plaque at the LM bifurcation and an occlusion of the SVBG‑OM (Figure 1A and 1B). PCI of the LM / left circumflex coronary artery (LCx) / IM was performed using drug‑coated balloons (DCBs). Following predilatation with noncompliant balloons, kissing balloon inflation was carried out with 2 sirolimus‑coated balloons: 2.5 mm × 20 mm (SeQuent SCB, B. Braun, Melsungen, Germany) in the IM and 3 mm × 20 mm (SeQuent SCB, B. Braun) in the LCx (Figure 1C and 1D). IVUS confirmed satisfactory results with no signs of dissection (Figure 1E and 1F). Hemodynamic status began to stabilize allowing for weaning of V‑A ECMO (after 3 days) and IABP (after 7 days; Figure 1G and 1H). The patient was discharged on the 24th day of hospitalization on dual antiplatelet therapy (acetylsalicylic acid and clopidogrel), atorvastatin 80 mg/day, bisoprolol, ramipril, and methylprednisolone 4 mg/day. Five‑month follow‑up was free of cardiovascular events.
PCI using DCBs in patients with active SLE may be a promising method of treating coronary artery disease (CAD), as it seems to reduce the risk of in‑stent restenosis due to the absence of foreign bodies in the vessels.4 However, an objective evidence to support such treatment strategy for SLE patients with CAD is missing. To our knowledge, this is the first case of an SLE patient with severe LM stenosis treated only with DCBs.
- Ayyad M, Albandak M, Khaleel M, et al. Acute myocardial infarction as the first presentation of systemic lupus erythematosus in a 23‑year‑old patient. Cureus. 2023; 15: e41026. | Crossref
- Bundhun PK, Boodhoo KD, Long M‑Y, Chen M‑H. Impact of antiphospholipid syndrome and / or systemic lupus erythematosus on the long‑term adverse cardiovascular outcomes in patients after percutaneous coronary intervention: a systematic review and meta‑analysis. Medicine. 2016; 95: e3200. | Crossref
- Sakowitz S, Bakhtiyar SS, Kim S, et al. Acute outcomes of cardiac operations in patients with autoimmune disorders: a national analysis. Am Surg. 2023; 89: 4025‑4030. | Crossref
- Muramatsu T, Kozuma K, Tanabe K, et al. Clinical expert consensus document on drug‑coated balloon for coronary artery disease from the Japanese Association of Cardiovascular Intervention and Therapeutics. Cardiovasc Interv Ther. 2023; 38: 166‑176. | Crossref
ARTICLE INFORMATION