Diabetic ketoacidosis leading to a diagnosis of medullary thyroid carcinoma and chronic lymphocytic leukemia: an extremely rare and unexpected case

 CC BY 4.0
CC BY 4.0
Diabetic ketoacidosis leading to a diagnosis of medullary thyroid carcinoma and chronic lymphocytic leukemia: an extremely rare and unexpected case
Diabetic ketoacidosis (DKA) is a life‑threatening metabolic complication that can occur in individuals with diabetes mellitus (DM). The risk of DKA is higher in patients with type 1 DM (T1DM), but it can also develop in those with T2DM, particularly in the presence of infection, trauma, or other critical health conditions. Prompt recognition and treatment are essential to prevent irreversible organ dysfunction.1
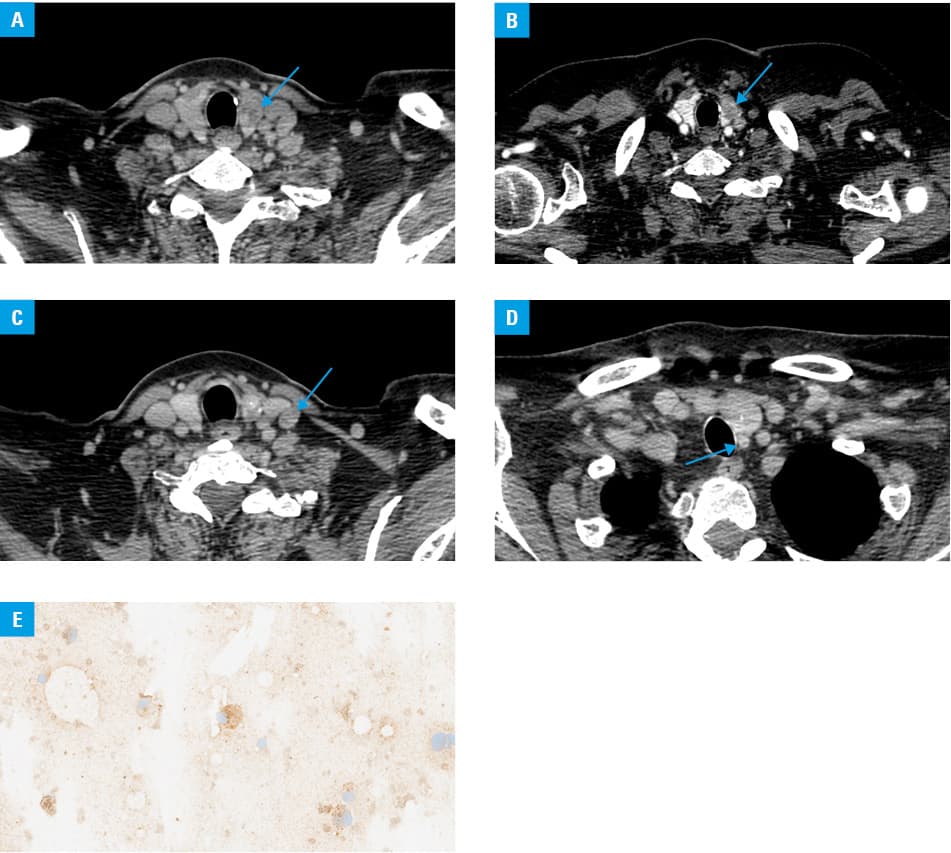
We report a case of a 65‑year‑old woman with a 10‑year history of T2DM, who presented to an emergency room in critical condition with a 1‑week history of profound fatigue, drowsiness, nausea, and a temperature of 39 °C for 2 days. She had been taking metformin, gliclazide, and dapagliflozin, the latter of which she had been on for 3 years. Based on the anamnesis and laboratory findings (Supplementary material, Tables S1 and S2), a diagnosis of DKA was established as a complication of T2DM. After 36 hours of intravenous insulin therapy, rehydration, electrolyte replacement (Supplementary material, Tables S3 and S4), and treatment with ceftriaxone, the patient’s clinical condition improved, and she was switched to subcutaneous insulin administration. On discharge, she was prescribed metformin and insulin pens containing insulin aspart and insulin aspart protamine. Since various factors can contribute to DKA, further detailed diagnostics were undertaken.2 After demonstrating lymphocytosis (7.68 × 109/l; reference range, 1–4 × 109/l) with atypical lymphocytes on blood smear, peripheral blood flow cytometry and computed tomography (CT) confirmed a diagnosis of chronic lymphocytic leukemia (CLL), Rai clinical stage 0, requiring only observation. CLL is an indolent B‑cell neoplasm, particularly affecting the elderly (mean age at diagnosis of approximately 70 years), involving a higher risk of infections due to impaired humoral immunity.3 Additionally, due to persistently high procalcitonin levels and low total calcium levels with significantly elevated serum calcitonin concentration (Supplementary material, Table S5), medullary thyroid carcinoma (MTC) was suspected. A neck CT scan (Figure 1A–1D) and the results of a fine‑needle aspiration biopsy of the tumor (Figure 1E) confirmed the diagnosis. MTC originates from parafollicular C cells and accounts only for 5%–10% of all thyroid cancers.4 In our patient, there was no family history of multiple endocrine neoplasia type 2.5 The patient was qualified for total thyroidectomy and bilateral neck lymphadenectomy and then discharged home.
Our report highlights the need for vigilant medical assessment and a multidisciplinary approach to identify and treat underlying causes of numerous abnormalities in laboratory tests. It is crucial to increase awareness among patients and health care professionals of the possibility of concurrent malignancies in patients presenting with medical emergencies, such as DKA, and having unrelated deviations on diagnostic tests.
- Cieluch A, Uruska A, Falkowski B, et al. Nonadherence to potassium replacement protocol leads to prolonged management of diabetic ketoacidosis. Pol Arch Intern Med. 2018; 128: 416‑420. | Crossref
- Araszkiewicz A, Bandurska‑Stankiewicz E, Borys S, et al. 2023 Guidelines on the management of patients with diabetes ‑ a position of Diabetes Poland. Current Topics in Diabetes. 2023; 3: 1‑133. | Crossref
- Długosz‑Danecka M, Jurczak W, Łątka‑Cabała E, et al. Efficacy and safety of the obinutuzumab‑chlorambucil combination in the frontline treatment of elderly CLL patients with comorbidities ‑ Polish Adult Leukemia Group (PALG) real‑life analysis. Pol Arch Intern Med. 2018; 128: 421‑426. | Crossref
- Erba PA, Maecke H, Mikolajczak R, et al. A novel CCK2/gastrin receptor‑localizing radiolabeled peptide probe for personalized diagnosis and therapy of patients with progressive or metastatic medullary thyroid carcinoma: a multicenter phase I GRAN‑T‑MTC study. Pol Arch Intern Med. 2018; 128: 791‑795. | Crossref
- Borowczyk M, Sypniewski M, Szyda J, et al. Genetic predisposition to differentiated thyroid cancer among Polish population. Pol Arch Intern Med. 2024; 134: 16654. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION