Nodular lymphocyte predominant B-cell lymphoma with isolated central nervous system localization in a renal transplant patient: a rare lymphoma subtype

 CC BY 4.0
CC BY 4.0
Nodular lymphocyte predominant B-cell lymphoma with isolated central nervous system localization in a renal transplant patient: a rare lymphoma subtype
Nodular lymphocyte‑predominant B‑cell lymphoma (NLP‑BCL) is a rare subtype that accounts for approximately 5% of all lymphomas. The incidence of NLP‑BCL is rare, with an estimated frequency of 0.1 to 0.2/100 000/year.1-3 NLP‑BCL rarely involves the central nervous system (CNS). In the available literature, we did not find an example of NLP‑BCL in renal transplant patients. Typical symptoms of intracranial localization include cranial nerve palsies, motor deficits, pain and paresthesias, altered mental status, seizures, and other signs of increased intracranial pressure.4
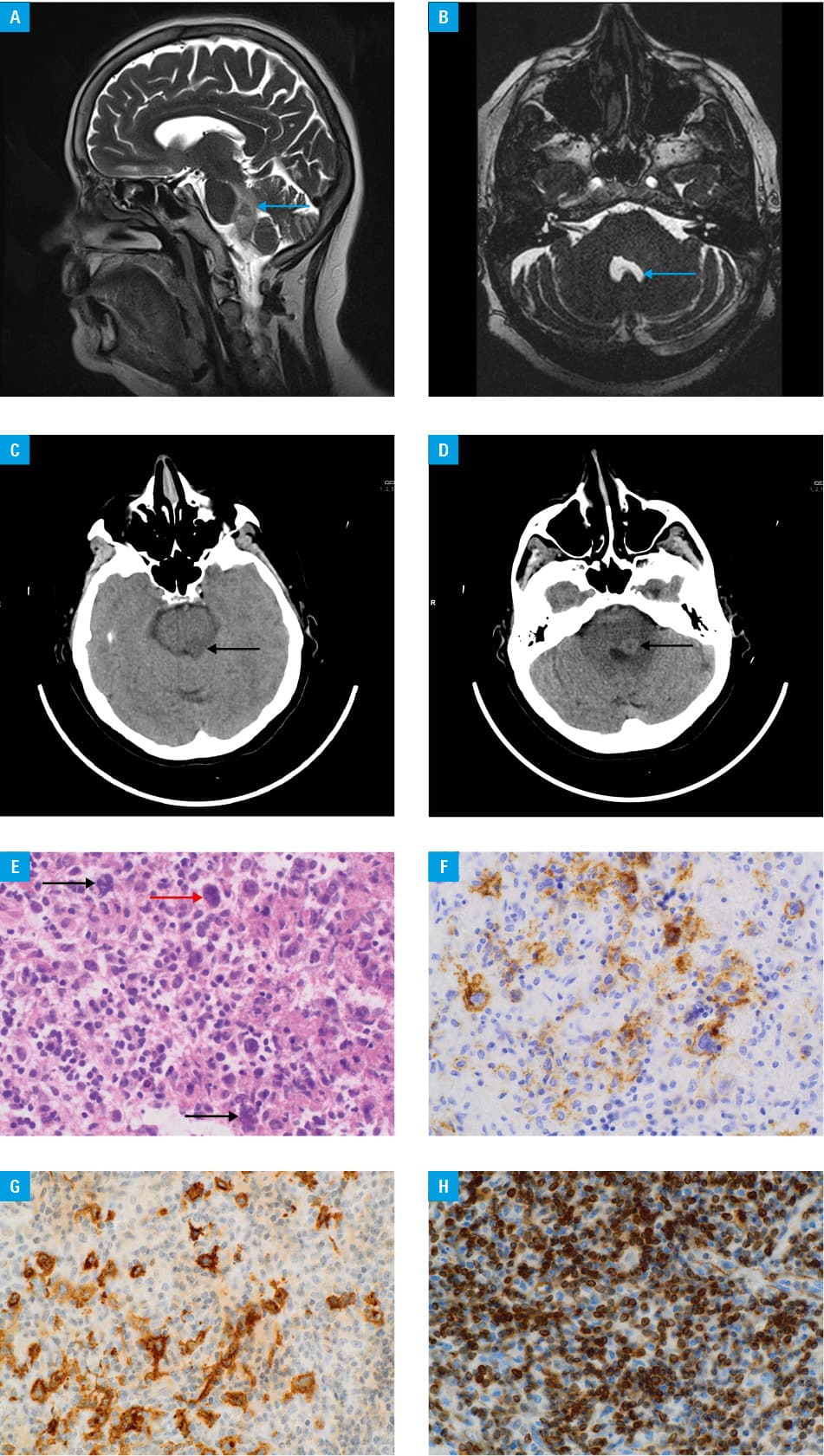
We present a case of a 54‑year‑old woman, 22 years after renal transplantation for end‑stage renal disease due to glomerulonephritis, treated with triple immunosuppressive therapy (prednisone, cyclosporine, and mycophenolate mofetil), who was admitted with imaging findings of focal lesions in the brainstem and cerebellum (Figure 1A–1D).
Medical history of the patient included diabetes mellitus, hypertension, subclinical hyperthyroidism, depression, glaucoma, and upper respiratory tract infection. The transplanted kidney had a preserved function with serum creatinine level of 96 µmol/l (reference range, 44–80 µmol/l).
On admission, the patient reported abnormal left temporomandibular joint pain lasting for several weeks, right‑sided facial paresthesia, left‑sided facial muscle weakness, imbalance, and altered taste on the left side of the tongue.
Physical examination showed right‑sided paresis of the cranial nerve III, superficial facial sensory loss on the right side, nystagmus, peripheral paresis of the cranial nerve VII on the left side, and positive Romberg test. After neurosurgical consultation, the patient was deemed a candidate for open biopsy of the focal brain lesion. Using computed tomography and neuronavigation, the biopsy site was localized and right suboccipital craniotomy was performed to obtain tissue from the lesion in the right cerebellar hemisphere.
The biopsy indicated a mixed lymphoproliferative process with T lymphocytes (CD3+, CD5+) and B lymphocytes (CD20+, CD79a+) with scattered CD15- and CD30‑positive cells, consistent with NLP‑BCL. The proliferative tissue also included macrophages (CD68+, langerin–, CD1a–). Notably, there are scattered, significantly larger, polymorphic, and occasionally binucleated cells with prominent nucleoli, some resembling classic Reed‑Sternberg cells, although the majority have the morphology of “LP cells” (Figure 1E–1H).
Cerebrospinal fluid (CSF) analysis demonstrated cell count of 0.02 × 10³/µl, leukocyte populations (CD45+; 97.91%) including 88.4% of cells of CD3+/CD2+/CD5+/CD7+ T‑cell lineage; CD4/CD8 ratio of 4.54, and CD45RA/CD45RO ratio of 0.23. The patient tested negative for Epstein‑Barr virus (EBV), consistent with a typical EBV‑negative status of NLP‑BCL. A positron emission tomography scan was performed to evaluate the disease progression and showed isolated lesions confined to the CNS without involvement of other organs. The patient was subsequently treated with 4 cycles of rituximab in a hematology department. The immunosuppressive regimen was changed, as cyclosporine and mycophenolate mofetil were discontinued and tacrolimus and mTOR inhibitor were added. Infectious complications including COVID‑19, pneumonia, and urosepsis were treated. At 5‑year follow‑up, there was no evidence of disease relapse, and graft function was maintained with estimated glomerular filtration rate of 60 ml/min/1.73 m2 (RR ≥ 60 ml/min/1.73 m2).
The diagnosis of NLP‑BCL requires clear morphologic and immunophenotypic features from lymph node or lesion biopsy. CSF evaluation is straightforward but has low sensitivity and may not accurately classify CNS lymphoma. Cell‑free circulating tumor DNA in the blood or CSF is increasingly being used to improve lymphoma diagnosis and recurrence detection.5 The presented case of NLP‑BCL demonstrates the necessity of a biopsy of the involved organ and the possibility of successful treatment with preserved function of the transplanted organ.
- Sidda A, Naleid NK, Manu G, et al. Nodular lymphocyte‑predominant Hodgkin lymphoma: review of current literature and case discussion. J Investig Med High Impact Case Rep. 2022; 10: 23247096221111767. | Crossref
- Eichenauer DA, Engert A. Nodular lymphocyte‑predominant Hodgkin lymphoma: a unique disease deserving unique management. Hematol Am Soc Hematol Educ Program. 2017; 1: 324‑328. | Crossref
- Banaszkiewicz M, Okoń K, Popiela T, et al. Post‑transplant lymphoproliferative disorder after kidney transplantation with organ‑specific disease. Pol Arch Intern Med. 2024; 134: 16698. | Crossref
- Gomez‑Figueroa E, Peiro‑Osuna RP, Reyes‑Moreno I, et al. Primary central nervous system lymphoma: clinical experience in a neurological center. Rev Neurol. 2019; 68: 59‑65.
- Bobillo S, Crespo M, Escudero L, et al. Cell free circulating tumor DNA in cerebrospinal fluid detects and monitors central nervous system involvement of B‑cell lymphomas. Haematologica. 2021; 106: 513‑521. | Crossref
ARTICLE INFORMATION