Hospitalizations of patients with rheumatoid arthritis in Polish intensive care units or cardiac intensive care units in the years 2011–2021: a population study
Key words: cardiac intensive care unit, intensive care unit, mortality, rheumatoid arthritis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Hospitalizations of patients with rheumatoid arthritis in Polish intensive care units or cardiac intensive care units in the years 2011–2021: a population study
Introduction: Rheumatoid arthritis (RA) is a chronic autoimmune disease associated with significant comorbidities, including cardiovascular and respiratory complications, leading to increased hospitalization rates in intensive care units (ICUs) and cardiac intensive care units (CICUs). This study examines factors related to ICU/CICU admissions among Polish patients with RA from 2011 to 2021.
Objectives: We aimed to analyze trends in ICU/CICU admissions, identify key factors influencing outcomes, and assess the impact of comorbidities on RA patient ICU/CICU mortality in critical care settings.
Patients and methods: This retrospective population‑based study utilized data from the Polish national hospital morbidity registry. Inclusion criteria comprised ICU/CICU admission and an International Classification of Diseases, Tenth Revision code for RA. A total of 3066 hospitalization records were analyzed, focusing on demographics, length of stay, primary diagnosis, and ICU/CICU mortality rates. A logistic regression was used to evaluate the predictors of ICU/CICU mortality.
Results: The study revealed a rising trend in ICU/CICU admissions, with a significant increase in 2021, potentially due to the COVID‑19 pandemic. The overall ICU/CICU mortality rate was 39.1%, with the highest values observed in patients with gastrointestinal (58.5%) and endocrine / metabolic diseases (61.5%). Urgent admissions and older age were strong predictors of ICU/CICU mortality (P <0.001), while sex was not a significant factor.
Conclusions: Our findings emphasize the need for early intervention and comprehensive management strategies to mitigate severe RA complications. Future research should explore long‑term outcomes and the impact of RA treatments on ICU/CICU care.
What's new?
This study uncovers significant trends in hospitalization of patients with rheumatoid arthritis (RA) in Polish intensive care units (ICUs) and cardiac intensive care units (CICUs) from 2011 to 2021, highlighting an increase in admissions and ICU/CICU mortality, particularly in 2021, likely linked to the COVID‑19 pandemic. A key finding is a high ICU/CICU mortality rate of 39.1%, especially among older patients and those admitted urgently. This research emphasizes a critical need for early intervention and comprehensive management strategies to improve outcomes for RA patients in critical care, offering new insights into the burden of severe RA complications and their management in clinical practice.
Introduction
Rheumatoid arthritis (RA) is a chronic systemic connective tissue disease of immunological origin, characterized by nonspecific symmetrical inflammation of the joints, the occurrence of extra‑articular changes, and systemic complications, leading to disability, handicap, and premature death. RA affects approximately 0.5%–1% of the global population, with the highest incidence around the age of 80 years.1,2 Without treatment, RA patients experience numerous exacerbations leading to disability and poor health outcomes. Early treatment can improve performance and reduce disease activity, but mortality remains similar for both early and late treatment.3
The patients with RA often develop other chronic conditions that significantly affect their health. Cardiovascular diseases are the most common cause of death in this population. One of the most critical complications of RA is coronary artery disease.4,5 RA patients have twice the risk of heart attack and up to by 50% higher risk of cardiovascular mortality than the general population.6 The prevalence of type 2 diabetes is also increased in patients with RA. Glucocorticoids, used to suppress inflammation in RA, adversely affect glycemic control, and diabetes further exacerbates cardiovascular risk.7
Respiratory diseases are the second leading cause of death in RA patients, occurring in 30%–40% of cases. RA can affect the lung interstitium, airways, pleura, and less frequently the pulmonary vessels.6 Conditions such as pleuritis, bronchiolitis, and interstitial lung disease (ILD) are also associated with RA. Reports indicate that ILD develops in 5%–16% of RA patients, and its occurrence is associated with shorter survival.8,9 Moreover, venous thromboembolic disease is more prevalent in RA patients, especially during therapy with tumor necrosis factor inhibitors and Janus kinase inhibitors.10
Chronic anemia and Felty syndrome are common complications in patients with seropositive RA.11 Secondary Sjögren syndrome, present in about 10% of RA patients, further complicates the disease. Rheumatoid vasculitis, though rare, can have severe consequences, resembling polyarteritis nodosa.11,12 Furthermore, the patients with RA have a higher likelihood of developing diseases such as Hodgkin and non‑Hodgkin lymphoma than the general population.13
Premature death is a common outcome of RA complications and their treatment. Serious infections, exacerbated by disease‑modifying antirheumatic drugs (DMARDs) and immune system dysfunction, pose significant risks.14 Osteopenia and osteoporosis, resulting from the disease and drug therapies, increase the risk of fractures, particularly in postmenopausal women and older adults.15 RA also affects the gastrointestinal system and kidneys, mainly through drug therapies.6 Depression, a frequent complication, affects patients with long‑term active disease and significant physical dysfunction.16
RA is one of the most prevalent rheumatological conditions necessitating admission to intensive care units (ICUs).17-19 The patients with RA have a significantly elevated risk of ICU admission, as compared with the general population, with over 1% of RA individuals experiencing critical illness annually, and a cumulative 10‑year risk approaching 8%.20 This increased risk is often attributed to the disease exacerbation or adverse effects of immunosuppressive therapy.17,21 The cardiovascular and respiratory systems are the most frequently affected.18,20
Mortality in this patient population is associated with several factors, including the severity of illness measured by the Acute Physiology and Chronic Health Evaluation (APACHE) II score, the updated Charlson Comorbidity Index, the Sequential Organ Failure Assessment (SOFA) score, the need for vasopressor support, advanced age, prolonged prothrombin time / international normalized ratio, cytopenia, and extended hospital stays.17,19,22
Hospitalization in an ICU or a cardiac intensive care unit (CICU) indicates a severe exacerbation of the illness, often requiring advanced medical interventions and constant monitoring. Understanding the factors related to ICU or CICU admissions among RA patients is crucial for improving clinical outcomes, optimizing resource allocation, and developing preventive strategies to reduce the burden of severe complications.
The aim of this study was to characterize selected factors related to ICU/CICU hospitalizations of Polish patients diagnosed with RA over a long‑term perspective, covering the years 2011–2021. This study sought to identify the patterns and trends in hospital admissions, evaluate the impact of comorbidities, and explore the outcomes of RA patients requiring intensive care. By gaining insights into these aspects, the research aimed to contribute to better management strategies and enhanced care for the individuals suffering from this debilitating condition.
Patients and methods
This retrospective study utilized anonymized data derived from the Polish national hospital morbidity registry. The research was conducted in collaboration with the Department of Social Medicine and Public Health of Medical University of Warsaw, and institutions such as the National Institute of Public Health NIH – National Research Institute and the National Institute of Geriatrics, Rheumatology, and Rehabilitation. The study was approved by the ethics committee of the National Institute of Geriatrics, Rheumatology, and Rehabilitation in Warsaw (KBT‑4/4/2024). The ethics committee did not require an informed consent from the patients analyzed in this retrospective study and approved publication of its results. Each study procedure complied with the Declaration of Helsinki or similar standard of ethics.
High completeness of the hospital morbidity data is due to the legal obligation imposed on inpatient health care units to periodically report hospitalization data to the National Institute of Public Health – National Institute of Hygiene. The information is reported by the hospitals using the General Hospital Statistical Card Mz/Szp‑11, covering all hospitalizations within the analyzed period. The accuracy and reliability of the data result from the efficiency and precision of reporting by individual entities. The study population, encompassing nearly 100% of hospitalizations in Poland, ensures the accuracy and reliability of the utilized data.
The study inclusion criteria comprised an ICU or CICU stay code in the hospitalization record and an International Classification of Diseases, Tenth Revision (ICD‑10) code for RA (M05, M05.x, or M06, M06.x) in the reported hospital morbidity data.
Both criteria had to be met simultaneously for patient inclusion in the study. There were no exclusion criteria.
The study involved 3066 hospitalization records. Of these, 2815 hospitalizations (91.8% of all records) were in the ICUs, and 251 (8.2%) in the CICUs. The majority of hospitalizations concerned women (n = 2270; 74%). Women accounted for 74.3% of the ICU and 71.3% of the CICU hospitalizations. The age of patients ranged from 19 to 96 years (mean [SD], 65.2 [11.5] years; median, 66 [range, 19–96] years).
Statistical analysis
Descriptive statistics were computed for the patient population. Frequencies were calculated for categorical variables, while means (SD) were computed for continuous variables. Trend lines for ICU/CICU admissions and patient deaths per year were plotted to examine temporal trends. Cross‑tabulation analyses were performed to investigate the distribution of primary diagnosis groups based on ICD‑10 codes, including their length of stay (LOS) and ICU/CICU mortality rates. The term “ICU/CICU mortality” used throughout the study refers to deaths recorded during the stay in the ICU/CICU. A cross‑tabulation Table was also created to display the primary wards to which the patients were admitted, including the frequency of emergency admissions.
A logistic regression model was used to identify the predictors of patient mortality during ICU/CICU stay. The dependent variable was ICU/CICU mortality (0 = survived, 1 = died), and the predictors included sex, age, and hospital admission mode. The predictors were introduced into the model in blocks to assess the incremental value of each block of predictors. The logistic regression results provided odds ratios with 95% CIs for each predictor. The model’s fit was evaluated using Nagelkerke pseudo R2. The significance level was set at a P value below 0.05.
All analyses and Figures were prepared using R (version 4.3.3; R Core Team, Vienna, Austria) with the ggplot2, MASS, broom, and rcompanion packages.
Results
The analysis demonstrated that 1198 patients out of the studied population (39.1%) died during their stay in the ICU/CICU. Figure 1 shows the trend lines for the number of ICU/CICU admissions and the number of deaths per year.
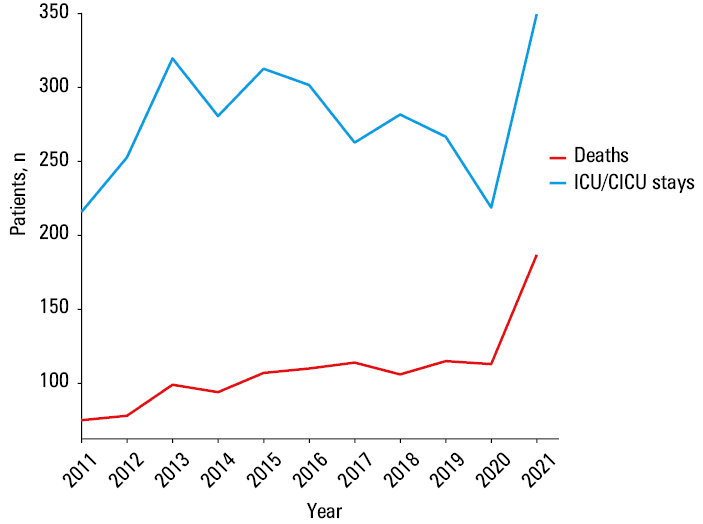
The chart indicates an increase in the ICU/CICU admissions and deaths in 2021, possibly related to the COVID‑19 pandemic.
In the next section, the factors related to the hospital admission were analyzed. As many as 1885 patients (63.9% of the study population) were urgently admitted to the hospital. The LOS ranged from 0 to 248 days (median [interquartile range {IQR}], 14 [7–23.75] days).
Mortality rates among the ICU patients were compared with those in the CICU, with the value of 42% in the former and 6.4% in the latter. The χ2 test showed a notable relationship between the type of ICU and the occurrence of death (χ2 = 123; P <0.001; ϕ = 0.2).
Table 1 presents the frequency of disease groups based on ICD‑10 codes for the primary diagnosis upon admission to the first ward. It shows that the largest group consisted of patients with diseases of the circulatory system (22% of the study population), musculoskeletal system and connective tissue (19.5% of the study population), and respiratory system (16.2% of the study population). Conversely, out of specific system diseases, the notably high ICU/CICU mortality rates were observed in patients with gastrointestinal (58.5% ICU/CICU mortality), endocrine, nutritional, and metabolic diseases (61.5% ICU/CICU mortality). The longest median (IQR) LOS was associated with the diseases of the skin and subcutaneous tissue (26 [19–39] days), while the shortest with pregnancy, childbirth, and puerperium (8 [5–14.5] days), where none of the 23 patients died. This lower ICU/CICU mortality rate and shorter LOS in the pregnancy, childbirth, and puerperium group could be attributed to the generally healthier and younger population and the nature of the hospital admission related to childbirth rather than acute or severe illness.
Disease group (ICD‑10 code) | Study population, n (%) | LOS, median (IQR) | ICU/CICU mortality rate, % |
a Due to a low number of individuals, calculating quartiles was impossible.
Abbreviations: CICU, cardiac intensive care unit; ICD‑10, International Classification of Diseases, Tenth Revision; ICU, intensive care unit; LOS, length of stay | |||
Diseases of the circulatory system (I00–I99) | 674 (22) | 10 (5–21) | 34.9 |
Diseases of the musculoskeletal system and connective tissue (M00–M99) | 599 (19.5) | 15 (10–22) | 19 |
Diseases of the respiratory system (J00–J99) | 498 (16.2) | 15 (7–28) | 47.6 |
Diseases of the digestive system (K00–K95) | 234 (7.6) | 15 (7–28) | 58.5 |
Symptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified (R00–R99) | 160 (5.2) | 12 (4–26.5) | 52.5 |
Certain infectious and parasitic diseases (A00–B99) | 143 (4.7) | 14 (5–27) | 57.3 |
Neoplasms (C00–D49) | 226 (7.4) | 12 (6–20) | 31.4 |
Codes for special purposes (U00–U85) | 136 (4.4) | 15 (9.75–24) | 71.3 |
Diseases of the genitourinary system (N00–N99) | 96 (3.1) | 12.5 (5–25.2) | 51 |
Diseases of the blood and blood‑forming organs and certain disorders involving the immune mechanism (D50–D89) | 87 (2.8) | 12 (5.5–20.5) | 46 |
Injury, poisoning, and certain other consequences of external causes (S00–T88) | 140 (4.5) | 15 (11.2–21) | 27.1 |
Diseases of the nervous system (G00–G99) | 44 (1.4) | 16 (9–31.5) | 38.6 |
Factors influencing health status and contact with health services (Z00–Z99) | 39 (1.3) | 13 (9–21.5) | 15.4 |
Endocrine, nutritional, and metabolic diseases (E00–E89) | 26 (0.8) | 10 (6–18.8) | 61.5 |
Diseases of the skin and subcutaneous tissue (L00–L99) | 25 (0.8) | 26 (19–39) | 56 |
Pregnancy, childbirth, and puerperium (O00–O9A) | 23 (0.8) | 8 (5–14.5) | 0 |
Congenital malformations, deformations, and chromosomal abnormalities (Q00–Q99) | 2 (0.1) | 11.5a | 50 |
Mental, behavioral and neurodevelopmental disorders (F01–F99) | 1 (0.05) | 16.4a | 0 |
Table 2 lists the primary wards to which the patients were admitted. The wards not shown in the Table had individual frequencies below 5%. In the analyzed population of patients with RA, the most common initial admission was to a department of trauma and orthopedic surgery, which accounted for 18.4% of all patients, primarily for elective procedures. Other common initial departments included ICU (18%), internal medicine (10.8%), hospital emergency (9.5%), general surgery (7.2%), and CICU (5.8%). In these cases, the admissions were predominantly emergencies.
Ward | Total admissions | Emergency admissions | ||
N1 | Percent of the study population | N2 | N2/N1, % | |
Department of trauma and orthopedic surgery | 563 | 18.4 | 72 | 12.8 |
Intensive care unit | 553 | 18 | 447 | 80.8 |
Internal medicine ward | 330 | 10.8 | 298 | 90.3 |
Hospital emergency ward | 290 | 9.5 | 284 | 97.9 |
General surgery department | 221 | 7.2 | 173 | 78.3 |
Cardiac intensive care unit | 179 | 5.8 | 141 | 78.8 |
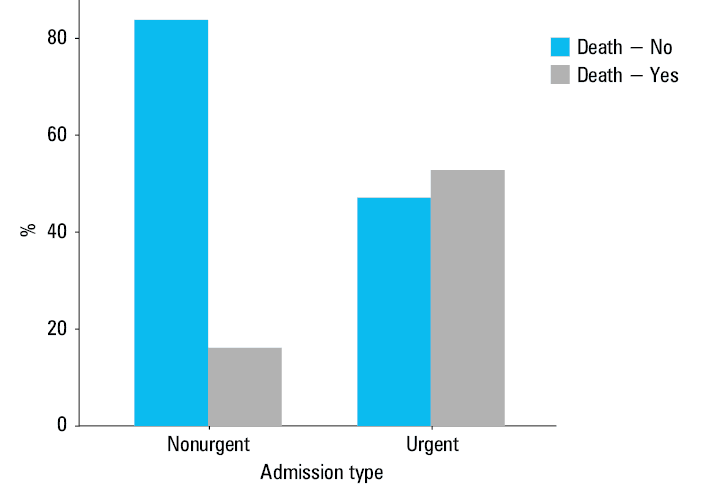
Figure 2 shows the percentage of deaths among patients admitted to a hospital on an urgent vs elective basis. The data indicate a significantly higher ICU/CICU mortality rate among the patients admitted urgently, as compared with those admitted electively. Specifically, the urgent admissions accounted for a ICU/CICU mortality rate of 52.8%, whereas the elective admissions had a substantially lower ICU/CICU mortality rate of 16.1%. This disparity can be attributed to a critical nature of conditions requiring the urgent admission, where patients often present with severe, life‑threatening complications necessitating immediate medical intervention. In contrast, elective admissions typically involve preplanned procedures for managing chronic conditions or routine surgeries, allowing for better preparation and stabilization of the patient’s health status prior to admission. The literature points out that surgical patients generally have better ICU prognoses than nonsurgical ones, who may present with complex, multisystem conditions requiring intensive, multifaceted management.23 Our findings highlight the importance of timely and effective acute care management for reducing ICU/CICU mortality rates in emergency situations.
In the logistic regression analysis, the dependent variable was death. The predictors included sex, age, and hospital admission mode. The results are presented in Table 3.
Independent variable | Estimate | SE | Z | P value | Odds ratio (95% CI) |
Intercept | –3.313 | 0.297 | 11.137 | <0.001 | – |
Sex (0 – men; 1 – women) | 0.048 | 0.092 | 0.521 | 0.6 | 1.049 (0.875–1.259) |
Age | 0.024 | 0.003 | 6.567 | < 0.001 | 1.025 (1.018–1.033) |
Admission type (0 – nonurgent; 1 – urgent) | 1.701 | 0.096 | 17.721 | < 0.001 | 5.483 (4.543–6.619) |
Nagelkerke R2 = 0.195 | |||||
The data included in Table 3 indicate that sex was not a predictor of ICU/CICU mortality in the studied population (P = 0.6). However, the results suggest that the older the patient is during their ICU/CICU stay, the higher the risk of death (P <0.001). There is also a higher risk of death among patients admitted to the hospital on an urgent basis (P <0.001).
Discussion
This study provides a comprehensive analysis of hospitalizations of patients with RA in Polish ICUs and CICUs over a decade of 2011–2021. The findings highlight significant trends and outcomes that are crucial for understanding the burden of severe RA complications and improving patient management strategies.
Trends in intensive care unit / cardiac intensive care unit admissions
The study demonstrated an upward trend in ICU/CICU admissions and associated ICU/CICU mortality over the observed period, particularly in 2021, which could be attributed to the COVID‑19 pandemic. The pandemic likely exacerbated existing health issues in RA patients, who are already at an increased risk for severe infections and complications due to their immunocompromised status and the use of immunosuppressive therapies. Of the analyzed patients, 165 were diagnosed with COVID‑19 during their hospital stay between 2020 and 2021, and 125 individuals died.
Intensive care unit / cardiac intensive care unit mortality and comorbidities
The ICU/CICU mortality rate among RA patients was notably high at 39.1%. This finding underscores the severe nature of RA and its associated complications. Cardiovascular and respiratory diseases were the most common primary diagnoses upon admission, consistent with existing literature that highlights these conditions as leading causes of ICU/CICU mortality in RA patients.17,19 Interestingly, the highest mortality rates were observed in the patients with gastrointestinal and endocrine, nutritional, and metabolic diseases, which points to the complexity and severity of comorbid conditions in this population. Patients with RA are particularly susceptible to infections, as evidenced by the fact that sepsis was identified in 351 of ICU/CICU hospitalized individuals.
Admission patterns and outcomes
A significant proportion of RA patients (63.9%) was admitted urgently, and they had higher ICU/CICU mortality rates than those admitted electively. This finding is critical, as it emphasizes the urgent need for timely and effective acute care management. The logistic regression analysis confirmed that urgent admissions and older age were significant predictors of ICU/CICU mortality. This aligns with previous studies suggesting that advanced age and the acute nature of hospital admissions are key factors influencing outcomes in critically ill RA patients.3-5,9,11
Sex disparities
While the majority of hospitalizations concerned women, reflecting the higher prevalence of RA among them, sex did not significantly predict ICU/CICU mortality. This finding suggests that while RA more often affects women, the severity of outcomes in ICU/CICU settings is influenced more by age and the urgency of admission rather than sex.
Length of stay and disease groups
The length of hospital stay varied significantly, with the longest average stay associated with diseases of the skin and subcutaneous tissue and the shortest with pregnancy, childbirth, and puerperium. This variation reflects the different nature and severity of the conditions leading to the ICU/CICU admissions. The notably lower ICU/CICU mortality and shorter hospitalizations in the pregnancy‑related group highlight the generally healthier status of these patients, as compared with those admitted for acute or severe RA complications.
Implications for clinical practice
The findings of this study have several implications for clinical practice, as described below.
Early intervention and monitoring
Given the high ICU/CICU mortality associated with urgent admissions, there is a need for proactive monitoring and early intervention strategies for RA patients, particularly those with known cardiovascular or respiratory comorbidities. Studies indicate that prompt detection and management of critical conditions, such as fluid overload, may help reduce mortality in acutely ill patients.24 Noninvasive monitoring techniques, including chest X‑rays enhanced with deep‑learning models, could be instrumental in identifying early signs of patient deterioration and facilitating timely interventions, especially when invasive approaches are not feasible.
Comprehensive management plans
Health care providers should develop comprehensive management plans that address both RA and its associated comorbidities to mitigate the risk of severe complications requiring ICU/CICU admissions. For end‑of‑life patients, maintaining an appropriate balance between essential interventions and nonbeneficial treatments is paramount. A focus on patient‑centered care and minimizing unnecessary interventions can offer greater benefit, particularly through palliative and supportive methods.25 This approach aligns with guidelines that advocate for respectful, dignified care plans and a balanced application of intensive treatments.
Resource allocation
Understanding the factors leading to ICU/CICU admissions can help optimize resource allocation and improve the preparedness of health care facilities to manage severe RA cases effectively. Furthermore, circumstances such as the recent, rapidly progressive streptococcal toxic shock syndrome epidemic in Kraków underscore the importance of response capability for diverse emerging threats.26
The above implications are confirmed by a large European study examining ICU mortality in patients over 80 years old,27 which found that delayed access to critical care, particularly in countries with lower health care expenditures, can exacerbate severity of the illness and boost mortality rates. This suggests that organizational factors and early access to ICU care for urgent RA admissions play a critical role in outcomes.
Limitations and future research
While this study provides valuable insights, it has several limitations. Its retrospective design and reliance on hospital records may introduce bias due to inaccuracies in coding and reporting. Another limitation is a lack of data on the illness severity on admission, such as APACHE or SOFA scores, which restricts the ability to assess the impact of patient condition on outcomes. Similarly, the absence of information on baseline RA treatment (eg, conventional, targeted, and biological DMARDs) and ICU interventions (eg, mechanical ventilation, continuous renal replacement therapy, vasopressors) limits the understanding of how organ support may have influenced mortality. Furthermore, the study did not explore the impact of specific RA treatments on ICU/CICU outcomes, which could be an area for future research.
While urgent admissions and older age are well‑established predictors of mortality in most ICU populations, our study highlights that patients with RA present additional complexities due to the burden of specific comorbidities, such as cardiovascular and respiratory diseases. These factors compound the already increased risk, making early intervention and comprehensive management strategies particularly important for this vulnerable group. No data on patient frailty on admission were available, despite frailty being a known predictor of mortality in critically ill patients, particularly among the elderly. This further constrains the analysis of baseline risk factors.
The analyzed data indicate that a notable portion of nonemergent admissions took place at the orthopedics and traumatology departments, raising the possibility that the ward of admission, rather than the urgency status alone, may play a role in influencing the prognosis. The fact that an admission was not classified as urgent does not necessarily mean it was elective. A substantial portion of such cases included, for example, transfers from other hospitals or compulsory admissions. These facts may represent a significant limitation of the above analysis and should be considered by the reader.
Future studies should aim to address these gaps by incorporating severity scores, treatment data, frailty assessments, and cause‑specific mortality to provide a more comprehensive analysis. Further investigations could also examine the long‑term outcomes of RA patients post‑ICU/CICU discharge to provide a better understanding of their recovery and quality of life.
Conclusions
This study highlights the significant burden of hospitalizations among patients with RA in Polish ICUs/CICUs from 2011 to 2021. The rising trend in the ICU/CICU admissions and associated mortality, particularly visible in 2021, underscores the heightened vulnerability of RA patients to severe complications, exacerbated by the COVID‑19 pandemic.
Key findings indicate a high overall ICU/CICU mortality rate of 39.1% among the RA patients in critical care, with cardiovascular and respiratory diseases being the most common primary diagnoses. The study also found that urgent admissions and older age were significant predictors of ICU/CICU mortality, emphasizing the need for timely and effective acute care management.
Sex did not significantly predict ICU/CICU mortality, despite the higher prevalence of hospitalizations among women. The length of hospital stay varied significantly across different disease groups, reflecting the diverse nature of the conditions leading to ICU/CICU admissions.
The findings underscore the need for proactive monitoring, early intervention, and comprehensive management plans that address both RA and its comorbidities to reduce severe complications and improve patient outcomes. Future research should focus on the long‑term recovery and quality of life of RA patients post‑ICU/CICU discharge and the impact of specific RA treatments on critical care outcomes.
- Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016; 388: 2023‑2038. | Crossref
- Radu AF, Bungau SG. Management of rheumatoid arthritis: an overview. Cells. 2021; 10: 2857. | Crossref
- Gwinnutt JM, Symmons DPM, MacGregor AJ, et al. Twenty‑year outcome and association between early treatment and mortality and disability in an inception cohort of patients with rheumatoid arthritis: results from the Norfolk arthritis register. Arthritis Rheumatol. 2017; 69: 1566‑1575. | Crossref
- Holmqvist M, Mantel Ä, Wållberg‑Jonsson S, et al. Findings on coronary angiographies in patients with rheumatoid arthritis and ischemic heart disease: are they different from patients without rheumatoid arthritis? Arthritis Care Res (Hoboken). 2021; 73: 658‑665. | Crossref
- Solomon DH, Goodson NJ, Katz JN, et al. Patterns of cardiovascular risk in rheumatoid arthritis. Ann Rheum Dis. 2006; 65: 1608‑1612. | Crossref
ARTICLE INFORMATION