Diverticular inflammation and complication assessment does not predict diverticulitis in asymptomatic individuals
1,2 ,
Key words: colonoscopy, Diverticular Inflammation and Complication Assessment, diverticular disease, diverticulosis, predictive value
,
Key words: colonoscopy, Diverticular Inflammation and Complication Assessment, diverticular disease, diverticulosis, predictive value



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Diverticular inflammation and complication assessment does not predict diverticulitis in asymptomatic individuals
Introduction: Recently, a 3‑step endoscopic scale, known as the Diverticular Inflammation and Complication Assessment (DICA), was introduced to predict the course of diverticular disease (DD), yielding some promising outcomes. However, analyses were performed only for symptomatic individuals.
Objectives: The aim of our study was to prospectively evaluate the predictive value of DICA in asymptomatic individuals with no previous diagnosis of DD who underwent colorectal cancer screening colonoscopy.
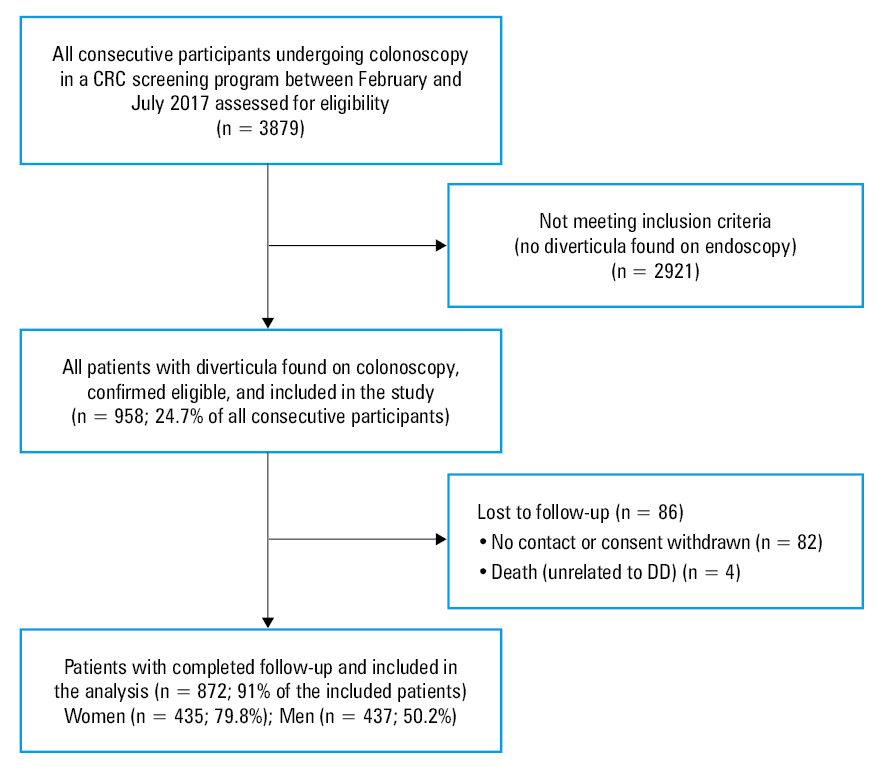
Patients and methods: We performed a prospective cohort study. All consecutive individuals, aged 55–65 years undergoing screening colonoscopy in a single center during a 6‑month period were assessed for eligibility. Those with diverticulosis were followed‑up for 12 months. Information on the course of the disease, symptoms, treatment, diverticulitis episodes confirmed by health care professionals, complications, and hospital admissions was obtained via telephone interviews conducted by doctors. Detailed patient data and medical conditions were evaluated.
Results: Out of 3879 participants, 958 (24.7%) had diverticula. Of these, 872 (mean [SD] age, 61 [2] years; 49.8% women) completed the study. About 83.5%, 12.85%, and 3.67% of the patients were classified into the DICA 1, DICA 2, and DICA 3 group, respectively. Diverticulitis occurred in 12 (1.37%) patients. Hospital admission was needed in 5 of them. No surgical interventions were necessary. There were no significant relationships between the DICA score and diverticulitis or hospital admission. Previous abdominal surgery and appendectomy, the presence and severity of pain, bloating, and previous DD treatment were the only factors predisposing to diverticulitis.
Conclusions: In our cohort, the DICA scale had no predictive value for the occurrence of diverticulitis. Hence, it has a limited predictive value for occurrence of this condition and more studies on bigger cohorts are necessary to test its usefulness.
What's new?
Diverticular disease (DD) is a common condition of the gastrointestinal tract with a spectrum of symptoms, from asymptomatic diverticulosis to severe complicated diverticulitis. Currently, there is no established scale to predict the progression of DD. The endoscopic Diverticular Inflammation and Complication Assessment (DICA) scale was recently evaluated for its ability to forecast episodes of diverticulitis based on the severity of endoscopic changes. We found diverticula in 24.7% of individuals aged 55–65 years on prophylactic colonoscopy. A vast majority of patients remained asymptomatic. After 1 year, only 1.37% developed diverticulitis. There was no correlation between the DICA score and diverticulitis. We found that the DICA score is not useful in predicting the course of DD in asymptomatic individuals. Consequently, there is still no established scale or score to predict the course of DD in the general population that would serve as a basis for treatment recommendations.
Introduction
Diverticulosis is one of the most prevalent findings in the large intestine. It is diagnosed in about 30% of patients aged over 50 years. Later its prevalence increases linearly, with diverticula present in over 75% of people older than 80 years.1 A Scandinavian study has recently shown that 10%–50% of asymptomatic participants of a colorectal cancer (CRC) screening program were diagnosed with diverticulosis, depending on age.2 A majority of individuals remain asymptomatic throughout their lives. Symptomatic uncomplicated diverticular disease (SUDD), which is the most common manifestation of diverticulosis, occurs in 32%–45% of these patients.2-4 Radiologically confirmed or surgery‑requiring diverticulitis appears to be less common than previously estimated (1%–4.3% of previously asymptomatic individuals and up to 7.6% of SUDD patients). Unfortunately, it is the first and, at the same time, admission‑requiring manifestation in over 43% of cases. In the last decade, there was a 42.7% increase in the number of hospital admissions.5-7 After the first episode of diverticulitis, the 5‑year risk of recurrence is 20%–35% in conservatively treated patients.8 The operative rates in diverticulitis reach 14%. Postoperative relapses of diverticulitis occur in 1%–3% of cases. Mortality due to disease complications oscillates around 1%.5,6 Due to its prevalence, spectrum of symptoms, and limited therapeutic options, diverticular disease (DD) remains a challenge for patients, doctors, and the health care system. It generates significant treatment costs and has a negative impact on the quality of life in developed countries. To date, no categorized risk assessment criteria for development of symptomatic forms of DD and predicting the occurrence of severe complications have been developed. Recently, a 3‑step endoscopic score, known as the Diverticular Inflammation and Complication Assessment (DICA) scale, has been introduced to predict further course of the disease, with promising primary outcomes.3 The proposed classification assesses the extent of lesions (right / left colon), the number of diverticula in each segment, inflammatory mucosal changes, and intestinal wall changes. Patients are classified as DICA 1 (≤3 points), DICA 2 (4–7 points), and DICA 3 (>7 points) (detailed DICA scale is presented in Table 1). However, previous studies were retrospective, with a prospective analysis limited to symptomatic individuals.9 Also, there was no additional external validation of the tool.
Variable | Details | Pointsa |
a DICA 1, 1–3 points; DICA 2, 4–7 points; DICA 3, >7 points
Abbreviations: DICA, Diverticular Inflammation and Complication Assessment | ||
Diverticula localization | Left side | 2 |
Right side | 1 | |
Number of diverticula in each region | ≤15 | 0 |
>15 | 1 | |
Inflammation on endoscopy | Edema / hyperemia | 1 |
Erosions | 2 | |
Segmental colitis | 3 | |
Complications | Rigidity | 4 |
Stenosis | 4 | |
Pus | 4 | |
Bleeding | 4 | |
Therefore, the aim of our study was to prospectively assess the predictive value of DICA in a subgroup of asymptomatic individuals with no previous diagnosis of diverticulosis, who underwent CRC screening colonoscopy. The primary end point was to assess the correlation between DICA severity (higher DICA score) and the prevalence of diverticulitis or the need for surgical intervention. Hereby, we performed a short‑term scale validation in a specific subset of patients. The secondary end point was to determine diverticulitis risk factors other than the DICA score.
Patients and methods
All consecutive individuals undergoing screening colonoscopy in a single tertiary referral center over a 6‑month period in 2017 were assessed for eligibility. Baseline demographic, epidemiologic, and medical data were collected using surveys conducted by qualified medical personnel immediately before endoscopic examination. The endoscopic examinations were conducted by a team of 15 experienced endoscopists. Training on the use of the DICA scale was performed before the beginning of the study.3
The participants diagnosed with diverticulosis for the first time and without declared symptoms or known colon diseases were followed‑up for 12 months. Exclusion criteria involved incomplete colonoscopy, inflammatory bowel disease, cancer of any origin, ischemic colitis, microscopic colitis, any severe systemic disease being a contraindication for the screening program, such as congestive heart failure, renal failure requiring dialysis, or liver failure (Child‑Pugh grade C). Information on the course of the disease, DD symptoms, treatment, diverticulitis episodes confirmed by medical health care professionals, complications, and hospital admissions was obtained via telephone interviews conducted by doctors. Additionally, detailed demographic and epidemiologic data, as well as patient medical status were recorded for further evaluation.
The assessed DD symptoms included pain, tenderness, bloating, constipation, and diarrhea. All symptoms were assessed on the numeric rating scale (NRS; 0–10). Diverticulitis was diagnosed by a doctor treating an acute episode and later confirmed by the study investigators by reassessing symptoms, laboratory and radiological findings, as well as the available medical documentation.
Ethics
All data were anonymized and digitalized for further analysis. The study was conducted according to the STROBE protocol. All patients gave their written informed consent. Approval of the bioethical committee was obtained (41/PB/2016). Initially, this cohort was a part of an international study assessing the predictive value of DICA registered in Clinical Trials (NCT02758860). Finally, this group was not included for further evaluation due to a prophylactic indication for colonoscopy; therefore, we decided to evaluate it separately.
Statistical analysis
Numerical data were collected in Excel spreadsheet Tables. To describe the qualitative variables, we used percentages. To describe quantitative variables, we used mean and SD (normally distributed variables) or median and interquartile range (IQR; not normally distributed variables). Normality was checked based on histograms. Categorized (binary) variables were compared using the χ2 test or the Fisher test, depending on the number of observations. Continuous variables were analyzed with the t test (in the case of normal distribution) or the Wilcoxon rank sum test (in the absence of normal distribution) and using the 1‑way analysis of variance (normal distribution) or the Kruskal–Wallis test (absence of normal distribution). All tests were performed at α = 0.05. The Bonferroni correction was used for multiple comparisons. Severity of symptoms was assessed by the patients on the NRS scale from 0 to 10 points. For the analytic purposes, NRS of pain has been described as median, and tertiles (for each symptom divided into third parts) were used in a logistic regression. We used the logistic regression to identify any potential risk factors for diverticulitis, with the following tested variables in the risk model: age, sex, body mass index (BMI), smoking status, a history of surgery, and the use of acetylsalicylic acid. The DICA variable was included in each model, regardless of the level of significance, as it was the main predictor. Stata version 13.1 package (Stata Corporation, College Station, Texas, United States) was used for analyses. A P value below 0.05 was considered significant.
Results
A total of 958 out of 3879 participants (24.7%) had diverticula found on colonoscopy. Of these, 872 completed the study (study flowchart, Figure 1). About 83.5% of the patients were classified as DICA 1, 12.85% as DICA 2, and 3.67% as DICA 3. There were no significant demographic, clinical, or social differences between these 3 subgroups (Table 2). Interestingly, 6% of the participants screened for CRC and assumed to be asymptomatic presented with symptoms consistent with SUDD, such as left lower quadrant abdominal pain or changes in bowel habits.
Abbreviations: CRC, colorectal cancer; DD, diverticular disease
Parameter | Total | DICA 1 | DICA 2 | DICA 3 |
Data are presented as number and percentage unless indicated otherwise.
Significant differences: number of men and women in the DICA 2 group (more men; P = 0.01), current smokers in the DICA 1 and DICA 3 groups (more in the DICA 3; P = 0.02)
Abbreviations: ASA, acetylsalicylic acid, BMI, body mass index; IQR, interquartile range; others, see Table 1 | ||||
Patients | 872 (100) | 728 (83.5) | 112 (12.85) | 32 (3.65) |
Women | 435 (49.8) | 373 (51.2) | 47 (42) | 15 (46.9) |
Age, mean (SD) | 61 (2) | 61 (2) | 61 (2) | 61 (2) |
BMI, kg/m2, median (IQR) | 27.9 (25.2–31.4) | 27.8 (25.1–31.2) | 28.4 (25.3–31.8) | 28 (25.4–31.6) |
Former smoker | 373 (42.8) | 313 (43) | 48 (42.9) | 12 (37.5) |
Never smoker | 323 (37) | 279 (38.3) | 37 (33) | 7 (21.9) |
Current smoker | 176 (20.2) | 136 (18.7) | 27 (22.1) | 13 (40.6) |
Any abdominal surgery | 337 (43.2) | 317 (43.5) | 43 (38.4) | 17 (53.1) |
Appendectomy | 116 (13.3) | 98 (13.5) | 11 (9.82) | 7 (21.9) |
Cardiovascular disease | 98 (11.2) | 77 (10.6) | 17 (15.2) | 4 (12.5) |
Metabolic diseases | 94 (10.8) | 72 (9.9) | 17 (15.2) | 5 (15.6) |
Treatment with ASA | 127 (14.6) | 100 (13.7) | 20 (17.9) | 7 (21.9) |
During the 12‑month observation, mild‑to‑moderate symptoms occurred in 443 patients (50.8%). The most common symptom was bloating, which was reported by 397 patients (45.5%), mostly associated with abdominal pain, which was the second most common symptom, observed in 196 patients (22%). A total of 134 patients (15%) presented with all symptoms, that is, pain, bloating, and altered bowel habits. In our cohort, there were no differences between the patients with pain, bloating, and constipation and those with pain and bloating accompanied by diarrhea. The assessed symptoms occurred at similar prevalence in patients with DICA 1, DICA 2, and DICA 3 score (between‑group comparison, Table 3). During the study period, 105 symptomatic patients (23%) were treated due to DD. More DICA 3 patients received treatment (25%), as compared with DICA 1 and DICA 2 groups (11% and 10%, respectively; P value was 0.01 for DICA 3 and DICA 1 as well as for DICA 3 and DICA 2, and 0.53 for DICA 1 and DICA 2). Seventeen patients (16%) received rifaximin, which was effective in 71%. The patients were also treated with antispasmodic and analgesic medications as well as herbs and probiotics, also with good results. Some of them received mesalamine with poor effect. A subgroup of patients had recurrent SUDD: 8.51% in the DICA 1 group, 5.3% in the DICA 2, and 11.8% in the DICA 3 group. The differences between DICA 1, 2, and 3 were insignificant.
Parameter | Total | DICA 1 | DICA 2 | DICA 3 | P value |
a Significant difference: bloating occurrence between DICA 1 and DICA 2 as well as DICA 1 and DICA 3; difference between DICA 2 and DICA 3: P = 0.06
Data are presented as number and percentage unless indicated otherwise.
| |||||
Number of patients | 872 | 728 | 112 | 32 | – |
Pain | 196 (22.5) | 167 (22.9) | 20 (17.9) | 9 (28.1) | 0.3 |
Pain severity, median (IQR) | 4.88 (3–6) | 4.83 (3–6) | 4.55 (3–6) | 6.45 (3–6) | 0.61 |
Bloating | 347 (39.8) | 298 (40.9) | 34 (30.6) | 15 (46.8) | <0.001a |
Constipation | 155 (17.8) | 132 (18.1) | 16 (14.3) | 7 (21.9) | 0.58 |
Diarrhea | 112 (12.8) | 15 (2) | 7 (6.3) | 4 (12.5) | 0.97 |
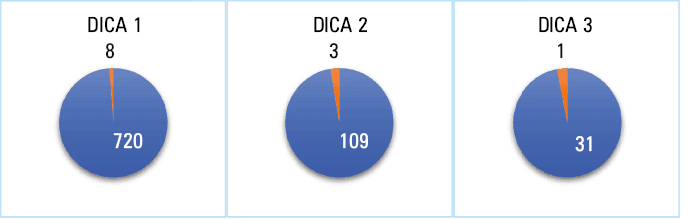
Diverticulitis occurred in 12 patients (1.37%; Figure 2). Treatment of diverticulitis was conducted by local doctors and included, apart from the medications mentioned above, oral or intravenous ciprofloxacin and / or metronidazole for 10 days depending on patient clinical assessment (hospitalized patients received intravenous treatment). No treatment‑related complications were reported. Five patients (42%) required hospital admission, but there were no surgeries due to complications. We found no differences between the DICA score groups in diverticulitis or hospitalization frequency (P values for compared variables were: DICA 1 vs DICA 2, 0.17; DICA 1 vs DICA 3, 0.3; and DICA 2 vs DICA 3, 0.89). In our cohort, we did not observe any recurrence of diverticulitis.
As for the risk factors, there were no differences in age, sex, body weight, or smoking status between the patients with and without diverticulitis, regardless of the DICA score. Previous laparotomy, regardless of the cause, was the only potentially significant predictive factor. Symptom analysis showed that pain and flatulence were the only symptoms that occurred more often in the patients with diverticulitis (P <0.001). Pain was worse in those who eventually developed inflammation (median, 7 vs 5 for patients without diverticulitis; IQR, 3–6 for both groups; P <0.001). A logistic regression model was then used to predict diverticulitis occurrence in different DICA groups by analyzing the relationship with previous surgery, abdominal pain, flatulence, and altered bowel habits. The patients who had undergone abdominal surgery were more likely to report abdominal pain and had higher prevalence of diverticulitis. The details are summarized in Supplementary material, Table S1.
Discussion
Until recently, DD was considered to be more or less expressed diverticulitis, with a varying spectrum of symptoms. Therefore, no attempt was made to identify predictors of diverticulitis in patients with mild symptoms, considering this to be a picture of the same disease. The disease perception has changed since 1999, when Kohler et al10 introduced the term SUDD. In 2012, Annibale et al11 published the first results of analyses summarizing the symptoms of DD, stratifying the condition into asymptomatic diverticulosis, SUDD, and complicated diverticulitis.
We found diverticula in 24.7% of the study population, and further 12 cases of diverticulitis were identified during 12‑month follow‑up, accounting for 1.37% of the study population. All diverticulitis diagnoses were positively verified, and no cases of inflammation were missed based on the interviews. Our data are consistent with previous studies. In 2016, Järbrink‑Sehal et al2 showed that in a group of participants randomly selected from the Swedish population, diverticulosis was diagnosed based on colonoscopy in 17.5%, with intestinal symptoms (primarily pain) affecting 45.1% of the respondents. Similarly, in 2019, van Dijk et al4 observed persistent symptoms in 32.2%–38.2% of patients after an episode of diverticulitis. The aforementioned study by Shahedi et al6 further showed that only 1% to 4% of asymptomatic patients developed diverticulitis. In our cohort, the spectrum and severity of symptoms were similar to those reported in previously published studies.12 These data allowed us to conclude that the group selected for further analysis was representative of a typical spectrum of the disease.
Prospective validation of the DICA scale, which assessed the correlation between the severity of lesions and occurrence of diverticulitis confirmed by medical professionals, was the primary end point. There were 8 (1.1%), 3 (2.7%), and 1 (3.1%) diverticulitis cases diagnosed in the DICA 1, DICA 2, and DICA 3 group, respectively. Diverticulitis was slightly more common in the DICA 2 and DICA 3 patients than in the DICA 1 group; however, the differences were not significant. Individual DICA subgroups were also compared in terms of the occurrence of diverticulitis with concomitant symptoms, such as flatulence and / or pain. We found no differences in the incidence of DD or diverticulitis symptoms depending on the DICA score. In our cohort, DICA severity did not translate into the incidence of diverticulitis in symptomatic or asymptomatic patients, or the need for hospital admission due to inflammation or its complications. The DICA score was not found to be a predictive factor, which excluded using the score as a tool for predicting the incidence of diverticulitis. Since we did not encounter any severe cases (eg, abscesses requiring drainage, peritonitis requiring laparotomy), we cannot state that DICA cannot predict the severity of an acute episode. Its predictive value may be limited and more studies are necessary to fully comprehend this issue.
In our study, the tool was negatively validated in patients without any significant clinical symptoms. In a retrospective study by Tursi et al,3 the DICA score had predictive significance, which became the basis for conducting a multicenter prospective analysis in a group of patients examined for various indications, but not prophylactically. The results of that analysis confirmed the predictive value of this score in patients with clinical symptoms.13 There were, however, several important differences between our study and that by Tursi et al.3
Our population comprised asymptomatic individuals younger than the patients in the compared study (mean age, 61 vs 66 years). In the retrospective observational study, Tursi et al3 included only patients with clinical indications for colonoscopy. It is possible that the study group consisted only of patients with abdominal symptoms or severe endoscopic lesions. Furthermore, since only the patients with complete medical records covering an average of 24 months were included, it may be assumed that these were mainly symptomatic individuals requiring further treatment. This assumption may also be supported by the percentage of patients diagnosed with inflammation (7.4%), which is the same as that of the SUDD patients. Due to the study group differences, there was a different proportion of DICA subgroups with the predominance of mild endoscopic changes in our population. Tursi et al3 identified 62.3% of patients as belonging to the DICA 1, 27% to the DICA 2 (twice more than in our study), and 10.6% to the DICA 3 (3 times more than in our study) group. Another difference is the percentage of diverticulitis in both studies. In our cohort, we found 1.34% of cases of diverticulitis, which is comparable to other recent studies, where diverticulitis was diagnosed in 1%–4.3% of asymptomatic participants of the CRC screening program over an 11‑year observation period.6 Meanwhile, Tursi et al3 found diverticulitis in 7.4% of cases over a 2‑year period. After 1 year of observation (duration of our study), diverticulitis accounted for 3% of cases. This number was already twice smaller than the number reported in the first retrospective assessment performed initially by the same primary investigator, but still 2 times higher than in other studies, including ours.2-5,11,13 Table 4 summarizes research results for diverticulitis assessing DICA scale usefulness.3,13 Such significant difference and high incidence of diverticulitis in both Tursi’s studies seems to be difficult to explain with reasons other than preselection of participants and / or symptom misinterpretation.3,9,13 It is also the main reason why there were significant differences between the DICA subgroups in these studies.
Parameter | Tursi,3 2016 | Tursi,13 2021a | Our study | |
a The prospective study lasted for 3 years, and after 1 year an interim analysis of the data was performed. It is presented in the Table to compare results with our study.
Abbreviations: see Table 1 | ||||
Type of study | Retrospective | Prospective | Prospective | |
Follow‑up, mo | 9–38 | 12 | 36 | 12 |
All DICA groups | 15.9 | 3.05 | 3.3 | 1.34 |
DICA 1 | 3.8 | 1 | 11.6 | 1.1 |
DICA 2 | 21.9 | 4.8 | 22 | 2.7 |
DICA 3 | 56.4 | 10.5 | 7.4 | 3.3 |
In our cohort, the participants in all groups were overweight or obese, thus we could not conduct any further analysis concerning the impact of body weight and BMI on the prevalence of diverticulitis. As reported by Mari et al,14 overweight is associated with over 3 times increased risk of diverticulitis among patients with diverticulosis. The impact of higher BMI is potent, and since overweight is a modifiable factor, it should be pointed out that nowadays over 53% of adult population in Europe have BMI over 25 kg/m2, and overweight and obesity remain large epidemiologic, socioeconomic, and public health problems.15 Increased BMI can be also a surrogate of highly‑processed food diet, which also is a risk factor for diverticulitis, as shown by Tursi and Elisei in 2020.16
We found diverticula in about 25% of the participants, which corresponds with other large epidemiologic studies.1,2,6-8 As mentioned earlier, the sensitivity of colonoscopy in the diagnosis of diverticula ranges between 64% and 91%. It should be pointed out that colonoscopy is not a recommended method of diagnosing anatomical changes, including diverticula. Endoscopists find approximately half of the diverticula described on double‑contrast barium enemas. The number of diverticula in each colonic segment is one of the assessed parameters. Incorrect calculation of the number of diverticula may result in misclassification.17-20
Twelve months of follow‑up may seem a short observation period. Nevertheless, if the predictive usefulness of the tool (DICA) estimating the risk of a diverticulitis episode unrelated to the onset of the observation, that is, colonoscopy, is assessed, then, in the case of an effective tool, parallel curves on the time‑frequency graph for the event should be obtained rather than curves constantly and nonlinearly increasing over time. When analyzing a sufficiently large cohort, the randomness of the event should not depend on the onset of the observation.
Considering the increasing incidence of diverticulitis during follow‑up, it can also be suspected, especially in patients with advanced endoscopic lesions, that cleansing for colonoscopy and the examination itself may cause some changes in the microbiota, and thus present a risk factor for symptomatic disease. None of the studies were designed to confront this hypothesis, but it is worth referring to studies linking colonoscopy with microbiota changes that give rise to gastroenterological symptoms.21,22
Contemporary studies investigating the etiopathogenesis of DD indicate that dysbiosis plays the main role in symptom onset. New insights have emerged regarding irreversibility of changes in the intestinal microbiota, which appears to be crucial for the occurrence and persistence of symptoms. This observation was confirmed by recent studies21-24 finding qualitative and quantitative changes in the intestinal microbiota composition and diversity between patients without diverticula, asymptomatic patients with diverticula, and those with the symptomatic disease. Major changes include reducing the abundance of Fecalibacterium, Lactobacillus, and Acermansia, which are butyrate‑producing bacteria. This reduction leads to proinflammatory changes with rising number of inflammatory cells and activation of inflammatory pathways.23 It is worth noticing that there are significant geographic differences in the composition of the intestinal microbiota. In the western and industrialized countries, the microbiota is less diverse but more prone to cause the gastrointestinal symptoms.24 Given the fact that cleansing the intestines replaces the microbiota, as evidenced in scientific research, colonoscopy may paradoxically increase the risk of inflammation. Performing endoscopy in individuals with pre‑existing symptoms or after episodes of diverticulitis, where additional microperforation of the intestinal wall weakened by the disease may occur, increases this risk. A previous study in a large group comprising 236 377 participants indicated that diverticulitis may rarely be a complication of colonoscopy (0.029%).25 With millions of colonoscopies performed annually worldwide, the absolute number of cases of inflammation will be noticeable. This is an additional argument questioning the safety of endoscopy in the case of borderline indications.
To the best of our knowledge, this is the first and so far the only study prospectively validating the DICA scale in asymptomatic individuals.
Colonoscopies were performed by experienced endoscopists trained in the DICA scoring system; graphic scales were available in endoscopy rooms where the examinations were performed and described, which helped to avoid incorrect interpretation of the results and minimize the percentage of omissions. The percentage of patients lost to follow‑up was small, and there were no significant differences in demographics or health issues (including DICA) between the group that completed the study and the group that was lost. Clear criteria for the diagnosis of diverticulitis were established based on simple, repeatable scales, and they were additionally verified by the principal investigator.
The limitation of the study was that it was a single‑center one. However, there were 7 endoscopy rooms and 15 experienced endoscopists involved. Short duration of the study was another limitation. As discussed earlier, if the endoscopic changes observed on colonoscopy were to translate into symptoms, this phenomenon should be independent of the observation time (these are not dependent variables), unless we accept the hypothesis of the negative impact of colonoscopy on the course of DD. The next significant limitation concerns the number of cases of diverticulitis possibly affecting the final results. Although the percentage of inflammation in our cohort is comparable to previous studies, numerically, a low number of diverticulitis cases was evaluated (12 in total, only 5 hospitalizations, and only 1 case in the DICA 3 group).6
Summarizing, DICA scale is useful, repeatable, and easy to implement. It is worth introducing this tool into everyday practice, as it enables precise diagnosis and communication between specialists. Although there are many similar scores in medicine, not all of them are predictive in nature. Similarly, DICA should not yet be considered a predictive tool for the general population, taking into account the results of this study and the arguments from previous studies. It seems to have a limited predictive value (or at least not as high as previously suggested) in asymptomatic individuals for the occurrence of diverticulitis, and more studies on bigger cohorts are necessary to test its usefulness. Analyzing our results, where the only risk factors for inflammation included previous abdominal surgery, severe abdominal pain, and treatment of DD, tools based on clinical symptoms should be developed. Finally, it should be emphasized that pain, with varying intensity of DICA score (more severe in DICA 3), was the main symptom in the discussed study by Tursi et al.13 The study did not analyze the risk factors for inflammation other than DICA (or age and sex). In our analysis, intense pain was the only symptomatic risk factor for diverticulitis; it could be concluded that pain was a predictive factor for diverticulitis also in the study by Tursi et al,13 with various severe endoscopic changes being only “innocent bystanders.”
- Strate LL, Modi R, Cohen E, et al. Diverticular disease as a chronic illness: evolving epidemiologic and clinical insights. Am J Gastroenterol. 2012; 107: 1486‑1493. | Crossref
- Järbrink‑Sehgal ME, Andreasson A, Talley NJ, et al. Symptomatic diverticulosis is characterized by loose stools. Clin Gastroenterol Hepatol. 2016; 14: 1763‑1770. | Crossref
- Tursi A, Brandimarte G, Di Mario F, et al. Predictive value of the Diverticular Inflammation and Complication Assessment (DICA) endoscopic classification on the outcome of diverticular disease of the colon: an international study. United European Gastroenterol J. 2016; 4: 604‑613.
- van Dijk ST, Daniels L, de Korte N, et al. Quality of life and persistent symptoms after uncomplicated acute diverticulitis. Dis Colon Rectum. 2019; 62: 608‑614. | Crossref
- Tursi A, Elisei W, Picchio M, et al. Impact of diverticular inflammation and complication assessment classification on the burden of medical therapies in preventing diverticular disease complications in Italy. Ann Transl Med. 2017; 5: 320. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION