Takotsubo syndrome (TS) is an acute, often reversible form of heart failure (HF), typically triggered by stressors, including medical or surgical interventions.1-4 While multiple potential causes of TS have been documented, cases arising from atrial fibrillation (AF) radiofrequency catheter ablation (CA) are exceedingly rare. In this report, we present a case where TS was induced by tamponade secondary to CA.
A 65‑year‑old woman with a diagnosis of paroxysmal AF and a history of anxiety disorder was admitted for her third CA. Prior to the procedure, the patient had no evidence of HF. The ablation procedure involved applications within the atrial chamber outside the pulmonary veins and took longer than standard pulmonary vein isolation. In the final stages of CA, a gradual decrease in blood pressure was observed. Transthoracic echocardiography (TTE) showed the presence of pericardial effusion, which was promptly drained. Immediately after the procedure the patient was in a stable condition, with adequate circulatory and respiratory function.
On the following day, the patient reported chest pain, dyspnea, and weakness. Additionally, sinus tachycardia was observed, along with a drop in oxygen saturation. Blood pressure values remained within normal limits. Considering the worsening signs of HF, furosemide and spironolactone were initiated. Additionally, the patient received ipratropium bromide, hydrocortisone, dabigatran, and supplemental oxygen. Moreover, potassium and magnesium supplementation, amiodarone, and metoprolol were provided to achieve rate control during an episode of AF. Subsequently, another TTE was performed (Figure 1A–1C), which showed severe akinesia of the apex, apical segments, and partially the midsegments of all walls of the left ventricle, with hyperkinesis of the basal segments. Left ventricular ejection fraction (LVEF) was assessed at 25%. Furthermore, there was left ventricular outflow tract obstruction (LVOTO), with the gradient values recorded at the level of 90 mm Hg (reference range <30 mm Hg), and significant mitral regurgitation due to systolic anterior motion (SAM) of the mitral valve. Electrocardiogram showed ST‑segment elevation and later inverted T waves (Figure 1D and 1E). Coronary computed tomography angiography was conducted due to the patient’s refusal to undergo coronary angiography, and it showed no significant stenosis of coronary arteries. The International Takotsubo Diagnostic Criteria score reached 83. Based on the above, a diagnosis of TS complicated by LVOTO and acute mitral regurgitation due to SAM was made.
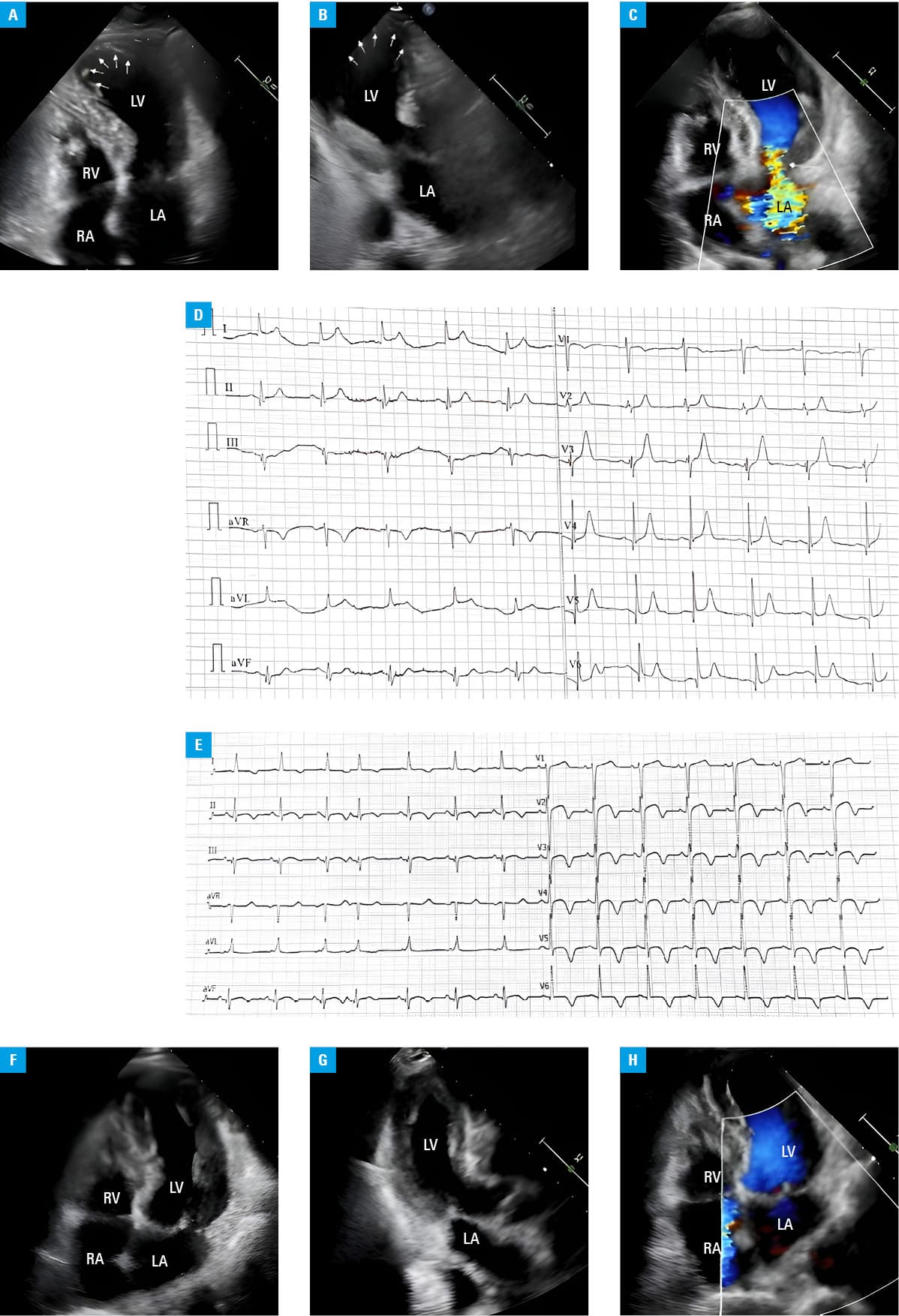
Abbreviations: LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle
On follow‑up TTE on the ninth day of hospitalization, an improvement in cardiac function was observed (Figure 1F–1H). Mild hypokinesia of the apex and apical segments of all walls was noted. LVEF rose to 53%. Mitral regurgitation was mild. LVOTO and SAM were absent, and there was no pericardial effusion.
Although TS is an extremely rare complication of CA, it might have an unfavorable prognosis.5 A case series of TS associated with AF CA has been reported5; however, according to our knowledge, no case of TS associated with CA‑related tamponade has been reported so far. While TS following AF CA typically resolves with supportive therapy, in rare instances, a malignant presentation may occur, requiring immediate intervention.5 Given the potential severity of TS, it is important to monitor patients after CA for symptoms indicative of this syndrome. Recognition of TS as a possible complication of CA for AF is essential to ensure prompt diagnosis and management.
- Lyon AR, Bossone E, Schneider B, et al. Current state of knowledge on Takotsubo syndrome: a Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2016; 18: 8‑27. | Crossref
- Budnik M, Piątkowski R, Ochijewicz D, et al. Pathophysiology of takotsubo syndrome as a bridge to personalized treatment. J Pers Med. 2021; 11: 879. | Crossref
- Boyd B, Solh T. Takotsubo cardiomyopathy: review of broken heart syndrome. JAAPA. 2020; 33: 24‑29. | Crossref
- Sobue Y, Watanabe E, Ichikawa T, et al. Physically triggered takotsubo cardiomyopathy has a higher in‑hospital mortality rate. Int J Cardiol. 2017; 235: 87‑93. | Crossref
- Mohanty S, Gianni C, Mayedo A, et al. Takotsubo syndrome following catheter ablation for atrial fibrillation: a single‑center experience. JACC Clin Electrophysiol. 2023; 9: 121‑123. | Crossref
ARTICLE INFORMATION