The role of lipoprotein(a) in atrial fibrillation: a systematic review
Key words: atrial fibrillation, biomarker, lipoprotein(a), risk factor



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The role of lipoprotein(a) in atrial fibrillation: a systematic review
Introduction: Atrial fibrillation (AF) is the most prevalent form of cardiac arrhythmia worldwide. Early diagnosis and treatment are essential, emphasizing the need to develop novel biomarkers. Lipoprotein(a) (Lp[a]) has recently been widely investigated as a potential risk factor for various cardiovascular conditions, including AF.
Objectives: Our objective was to systematically review the current knowledge on the role of Lp(a) in AF.
Methods: This systematic review adhered to the PRISMA 2020 guidelines. We included full‑text original clinical studies in English assessing the role of Lp(a) in AF. A comprehensive search in 5 databases: Embase, MEDLINE Ultimate, PubMed, Scopus, and Web of Science yielded 26 original, relevant clinical research articles that we analyzed in this study.
Results: Studies investigating the association between Lp(a) level and the incidence of AF present conflicting findings. However, Mendelian randomization studies advocate a causal association between high Lp(a) levels and AF. Research data suggest that AF patients who experience stroke or other thromboembolic events tend to have higher Lp(a) levels than those not experiencing such events.
Conclusions: Existing data suggest Lp(a) may play a pathophysiological role in AF patients, especially those who experience thromboembolic events. Nevertheless, this field requires further research due to inconsistencies in the existing evidence.
What's new?
Lipoprotein(a) (Lp[a]), a variant of low‑density lipoprotein, is an established causal risk factor for atherosclerotic cardiovascular disease and aortic stenosis. While evidence supporting its role in other conditions is limited, some studies reported its pathophysiological role in atrial fibrillation (AF). This research systematically reviews current knowledge on the role of Lp(a) in AF, providing a study‑by‑study analysis and overall conclusions. To the best of our knowledge, this is the first systematic review on the role of Lp(a) in AF that includes various study types. We found little evidence to support the association between the Lp(a) levels and AF incidence. However, genetic studies show a causal relationship between high Lp(a) level and AF. Patients with AF who experienced thromboembolic events had higher Lp(a) concentrations than those who did not.
Introduction
Atrial fibrillation (AF) is the most prevalent form of cardiac arrhythmia worldwide.1 Early diagnosis and optimal patient management are essential to minimize the risk of major adverse cardiac and cerebrovascular events, such as stroke.2 Some risk factors are well established, but not all have been discovered yet.3 Therefore, it is necessary to adequately manage all risk factors associated with AF and its complications.4 Despite clear diagnostic criteria for AF, its diagnosis may be challenging due to the self‑limiting character of the condition. Thus, a patient suffering from paroxysmal AF may remain undiagnosed for a significant period of time, which increases the risk of adverse events.5 A biomarker capable of differentiating between healthy people and those with AF, regardless of the current heart rhythm, would significantly improve AF diagnosis and management.6-8 Additionally, biomarkers with predictive value for adverse events in already diagnosed AF patients would be highly useful.9 Novel biomarkers, with improved sensitivity and specificity, which can independently predict adverse events, could facilitate more accurate decisions on whether to treat patients with anticoagulation, especially those with low CHA2DS2-VA scores.10
Lipoprotein(a) (Lp[a]) is a type of low‑density lipoprotein (LDL) that contains a protein called apolipoprotein(a) on its surface.11 Although it was first discovered in 1963, it remained overlooked for many years.12 Lp(a) received scientific attention again when Mendelian randomization studies on large cohorts proved its independent causal association with atherosclerotic cardiovascular disease (ASCVD).13 It is well documented that Lp(a) is a continuous risk factor for ASCVD, meaning that the risk increases continuously with an increase in Lp(a) concentration.14 According to the European Atherosclerosis Society (EAS) consensus statement, Lp(a) is a new risk factor for aortic stenosis.15 Everyone should check their Lp(a) level at least once in a lifetime.16 Several recent studies have reported the incidence of elevated Lp(a) concentration in the Polish population. The PMMHRI‑Lp(a)-Registry included 511 patients at a mean (SD) age of 48.21 (20.57) years. Of those, 27.8% had Lp(a) levels above 30 mg/dl, and 19.8% above 50 mg/dl (normal range <30 mg/dl).17 The first results from the Zabrze‑Lipoprotein(a) Registry, which included 2001 patients, showed very similar findings despite the mean (SD) age of patients being significantly higher, that is, 66.4 (14.1) years. Lp(a) levels above 30 mg/dl were found in 27% of the patients, while those above 50 mg/dl were reported in 20% of the participants.18 A STAR‑Lp(a) cross‑sectional study19 included 2475 patients without ASCVD, heart failure (HF), significant valve disease, and aortic aneurysm. As expected, the proportions of patients with elevated Lp(a) levels were lower, that is, Lp(a) levels equal to or above 30 mg/dl were found in 21.5% od cases, and those equal to or above 50 mg/dl in 13.5% of the patients.19
High Lp(a) levels contribute significantly to the overall risk of ASCVD, and neglecting them may lead to substantial risk underestimation and inadequate management.13,20 In addition, Lp(a) is highly homologous with plasminogen. Thus, it was hypothesized that Lp(a) would play an essential role in thromboembolism.21
Many studies have explored the potential role of Lp(a) in AF. While some investigated the difference in Lp(a) levels between AF patients and healthy individuals, others examined whether Lp(a) is a risk factor for AF and the extent to which it may predict AF onset. Thus, while the potential predictive value of Lp(a) for AF occurrence or reoccurrence has been widely studied, Mendelian randomization techniques were invaluable in assessing the possible causal association between high Lp(a) levels and AF incidence.
This study systematically reviews and discusses the results of original clinical studies investigating the role of Lp(a) in AF. It aimed to answer the following questions: 1) Is Lp(a) level associated with the incidence of AF? 2) Is there a causal relationship between Lp(a) level and AF occurrence? 3) Can Lp(a) level predict thromboembolic events in patients with AF?
Methods
This systematic review was conducted in accordance with the PRISMA 2020 guidelines22 (Supplementary material, Table S1). Full‑text original clinical studies in English assessing the role of Lp(a) in AF were included. Systematic reviews, meta‑analyses, reviews, case reports, letters to editors, commentaries, conference abstracts, guidelines / statements, expert opinions, and preprints were excluded. A comprehensive search was conducted on October 22, 2024 in 5 databases: Embase, MEDLINE Ultimate, PubMed, Scopus, and Web of Science. The following query was utilized: (lipoprotein(a) OR lp(a) OR lipoprotein[a] OR lp[a] OR lipoprotein a OR lp a) AND (atrial fibrillation OR atrial fibrilation), which yielded a total of 647 records. GP screened the records and extracted data from each included work.
The following data were extracted from each research study: study characteristics (sample sizes, methodology used, year of publication, study type) and the main findings regarding Lp(a) in the context of AF.
After removing 394 duplicates, the remaining 253 records were screened by title and abstract. This yielded 29 records that met the inclusion criteria. All 29 studies were retrieved in a complete form. The entire data report was evaluated for eligibility, and further 3 studies were excluded: 1 due to the paper type (research letter, not full‑text original research), 1 due to low‑quality data (the research focused on gut microbiota in the context of AF, while Lp[a] was one of the multiple additional factors analyzed), and 1 due to non‑English language. Finally, 26 original clinical research articles relevant to the discussed area were included (Figure 1). The quality of the included studies in terms of the aim of this systematic review was assessed using the Newcastle‑Ottawa Scale for assessing the quality of nonrandomized case‑control studies23 (Supplementary material, Table S2).
![Summary of the role of lipoprotein(a) (Lp[a]) in atrial fibrillation (AF)](/paim/_next/image/?url=https%3A%2F%2Fpamw.pl%2Fsites%2Fdefault%2Ffiles%2Fjson_zip_files%2Funcompressed%2F16924%2FIMAGES%2FKP_WEB__FIG_01.png&w=3840&q=75)
The included studies were divided into the following groups: 1) Lp(a) and the association with AF; 2) Lp(a) as a causal risk factor of AF in Mendelian randomization studies; 3) Lp(a) as a predictor of thromboembolic events in patients with AF; and 4) Lp(a) correlation with the presence of left atrial (LA) thrombus (LAT) in patients with AF.
Results
Lipoprotein(a) and the association with atrial fibrillation
Díaz‑Peromingo et al24 recruited 101 patients with AF and an equivalent number of patients without AF, matched for sex and age. They compared Lp(a) concentrations between the groups and found no significant differences. Nevertheless, they included a relatively small number of patients, which might have potentially influenced the results. Naji et al25 identified Lp(a) as a potential biomarker predicting the recurrence of AF after electrical cardioversion (EC). They analyzed retrospective medical data of 79 AF patients undergoing EC and followed‑up for 2 years after the procedure. The patients were divided into 2 groups of those with and without AF recurrence. No difference in Lp(a) concentration was found between the groups. In addition, Lp(a) levels did not exhibit any association with AF recurrence.25 Li et al26 investigated the significance of Lp(a) in AF occurrence in 679 patients with chronic HF (CHF) divided into 2 groups based on the AF status at baseline. The patients with AF had higher Lp(a) concentration than those without AF at baseline. Furthermore, the patients without AF were followed‑up for new‑onset AF, demonstrating that Lp(a) was an independent predictor of new‑onset AF in a multivariable model.26 Aronis et al27 analyzed if high Lp(a) concentration increases the risk of AF incidence in a large prospective community‑based cohort from the ARIC (Atherosclerosis Risk in Communities) study. They included 9908 participants free of AF at baseline and measured their Lp(a) concentration. The researchers analyzed the incidence rate of AF in the groups with increasing Lp(a) concentration: 1) up to 10 mg/dl, 2) above 10 to 20 mg/d, 3) above 20 to 30 mg/dl, 4) above 30 to 50 mg/dl, and 5) above 50 mg/dl. No association was found between Lp(a) concentration and the rate of AF, regardless of the adjustment model.27 On the contrary, Tao et al28 obtained results that contradicted those of other researchers. In a group of 13 533 patients (4511 with AF and 9022 without AF) divided into 4 groups based on the quartiles of Lp(a) concentrations, they found that Lp(a) concentrations were lower in the patients with AF than those without AF. The authors hypothesized that this observation might have been influenced by the ethnicity of the patients, that is, Han ethnicity, which is known to have lower Lp(a) levels than other ethnicities. Moreover, this inverse correlation was observed only in women and was confounded by coronary heart disease and type 2 diabetes mellitus. Potential mechanisms responsible for this inverse correlation, as indicated by the authors, could be cell membrane stabilization preventing the abnormal discharge of cardiomyocytes, or inflammation status, as the patients with AF had higher levels of C‑reactive protein, a biomarker of inflammation. The authors argued that during inflammation total cholesterol and LDL cholesterol levels are reduced and potentially the same may apply to Lp(a).28
Li et al29 studied the interplay between Lp(a), AF, and coronary artery disease (CAD). They included 2048 patients and divided them into 4 subgroups based on the AF and CAD status: 1) no CAD or AF, 2) AF without CAD, 3) CAD without AF, and 4) CAD and AF. The authors found that patients with CAD and AF had higher levels of Lp(a) than those with CAD but without AF. This result was not observed in patients without CAD. Moreover, in a multivariate logistic regression, Lp(a) was an independent risk factor for AF in CAD patients.29 Toprak et al30 examined the association between several biomarkers and the incidence of AF in a large cohort of 42 280 individuals without AF at baseline. They found no association between the Lp(a) level and the occurrence of AF. Zhang et al31 performed a retrospective case‑control study with 89 patients newly diagnosed with nonvalvular AF (NVAF) and 88 sinus rhythm patients as controls. Their findings indicated that Lp(a) concentration was higher in the patients with NVAF than in the controls. The authors also found that Lp(a) was an independent risk factor for the incidence of newly diagnosed NVAF; however, the sensitivity and specificity were relatively low (53.9% and 73.9%, respectively). Manla et al32 compared patients with Lp(a) levels above and below 125 nmol/l (approximately 50 mg/dl). They found no difference in the incidence of AF between the groups. In contrast, Burzyńska et al19 recruited 2475 patients referred to outpatient cardiology clinics and divided them based on Lp(a) levels adopting a cutoff of 30 mg/dl. They found that AF was independently related to Lp(a) levels equal to or above 30 mg/dl.19
Of the 10 studies discussed, 5 did not identify any difference in Lp(a) levels between AF patients and healthy controls; 4 found that a high Lp(a) level was associated with the incidence of AF; and 1 concluded that a low Lp(a) level was associated with the incidence of AF. Noteworthy, 2 of the 4 studies that identified high Lp(a) levels as a potential AF risk factor included a specific cohort of patients, that is, patients with CHF and those with CAD. A different study design (retrospective vs prospective) can partially explain discrepancies within the existing evidence. However, studies based on the largest cohorts did not find an association between high Lp(a) level and AF incidence.27,30 All studies discussed in this section, along with supplementary information, are presented in Table 1.
Year | Population | Comparison | Methodology | Study type | Outcome |
a 1 nmol/l = 0.4 mg/dl
Abbreviations: ↓, decreased; ↑, increased; AF, atrial fibrillation; ARIC, Atherosclerosis Risk in Communities; CAD, coronary artery disease; CHF, chronic heart failure; EC, electrical cardioversion; EDTA, ethylenediaminetetraacetic acid; ELISA, enzyme‑linked immunosorbent assay; Lp(a), lipoprotein(a); NVAF, nonvalvular atrial fibrillation | |||||
200624 | 101 AF patients | 101 age- and sex‑matched controls | Lp(a) measured by ELISA | Case‑control study | No difference in Lp(a) concentrations |
201125 | 79 AF patients undergoing EC | 2 groups: 1) AF recurrence, 2) no AF recurrence | Data on Lp(a) measurements unavailable | Retrospective case‑control study |
|
201626 | 679 CHF patients | 2 groups: 1) AF at baseline (n = 145), 2) no AF at baseline (n = 534); patients with no AF at baseline followed‑up | Lp(a) measured in plasma / serum by ELISA | Prospective cohort study |
|
201727 | 9908 ARIC cohort participants free of AF at baseline | Incidence rate of AF between various Lp(a) concentration groups | Lp(a) measured in EDTA plasma by Denka Seiken assay | Prospective cohort study | No association between Lp(a) levels and incidence of AF |
202228 | 4511 AF patients | 9022 patients without AF | Lp(a) measured in serum by latex‑enhanced turbidimetric method | Retrospective cohort study |
|
202229 | 2048 patients | 4 groups: 1) no CAD or AF (n = 400), 2) AF without CAD (n = 126), 3) CAD without AF (n = 1294), 4) CAD and AF (n = 228) | Lp(a) measured in EDTA blood by ELISA | Retrospective case‑control study |
|
202330 | 42 280 individuals without AF at baseline | 1496 cases of incident AF documented | Lp(a) measured in serum by particle‑enhanced turbidimetric immunoassay | Prospective case‑control study | Lp(a) level not associated with the incidence of AF |
202431 | 89 newly diagnosed NVAF patients | 88 sinus rhythm patients | Data on Lp(a) measurements unavailable | Retrospective case‑control study |
|
202432 | 903 patients with Lp(a) >125 nmol/la | 4774 patients with Lp(a) <125 nmol/l | Lp(a) measured by latex‑enhanced turbidimetric method | Retrospective cohort study | No difference in the incidence of AF between the groups |
202419 | 533 patients with Lp(a) ≥30 mg/dl | 1942 patients with Lp(a) <30 mg/dl | Lp(a) measured by ELISA | Prospective cohort study | AF independently related to Lp(a) ≥30 mg/dl |
Lipoprotein(a) as a causal risk factor of atrial fibrillation in Mendelian randomization studies
Zanetti et al33 conducted a Mendelian randomization study assessing the causal role of Lp(a) alongside other biomarkers in several cardiovascular diseases, including AF. The authors used data from the United Kingdom (UK) Biobank, including up to 451 933 participants. AF occurred in 13 312 cases. Although several causal associations were observed, including the causal role of Lp(a) in CAD, such a relationship was not noted in the case of Lp(a) in AF.33 Satterfield et al34 conducted another Mendelian randomization study, including 804 507 participants from the Electronic Medical Records and Genomics Network, UK Biobank, and Million Veteran Program cohorts. The authors mainly focused on analyzing the association between Lp(a) levels and the risk of ASCVD subtypes. Nevertheless, using the Mendelian randomization‑phenome‑wide association analyses, they found a novel association between genetically increased Lp(a) levels and the risk of AF.34
Jiang et al35 also performed a Mendelian randomization study using the UK Biobank resources. They included 377 600 participants with measured Lp(a) concentrations and known single nucleotide polymorphisms (SNPs) associated with Lp(a). The analysis found that genetically high Lp(a) levels were associated with an increased risk of AF. This was also observed in multivariable models adjusted for other lipid profile components. The effect size was a 1.001 odds ratio (OR) for each 1‑SD increase in the Lp(a) measure. The authors concluded that Lp(a)-lowering therapies might benefit the primary prevention of AF.35 Mohammadi‑Shemirani et al36 also performed a Mendelian randomization study using data from the UK Biobank. They assessed the occurrence of AF (20 432 cases) within the studied population (435 579 participants) in the context of measured and genetically predicted Lp(a) levels. Consistent with Jiang et al,35 their findings indicated that an increase in Lp(a) concentration was associated with an increased risk of AF (for a 23‑mg/dl increase in Lp[a] hazard ratio was 1.03 for measured Lp[a], and OR was 1.03 for genetically predicted Lp[a] level). Notably, although ASCVD mediated some of this risk, Lp(a) was a risk factor for AF independent of its established effects mediated via ASCVD.36
Wang et al37 conducted another Mendelian randomization study evaluating the relationship between Lp(a) and a risk for various CVDs. The authors based their research on a different Lp(a) dataset, specifically employing data from Neale Lab, which comprised 377 590 individuals of the European ancestry. They found no causal association between Lp(a) and AF.37 Xia et al38 recruited 1256 individuals and measured their Lp(a) serum concentrations. For Mendelian randomization analyses, they used published data from genome‑wide association studies. However, their findings were in contrast with the previously mentioned ones; they found that genetically increased Lp(a) level was inversely associated with the risk of AF. The possible discrepancies between these studies may result from the inclusion of different ethnic groups, which is known to affect Lp(a) concentration.38 The last discussed Mendelian randomization study was conducted by Tao et al.39 The authors found that genetically predicted high levels of Lp(a) are associated with an increased risk of AF in the European population. They also showed that inhibiting the LPA gene may have a potential protective effect partially mediated by lowering coronary heart disease risk.39
In summary, of the 7 identified Mendelian randomization studies, 4 found high levels of Lp(a) being causally associated with the increased risk of AF. The other 2 studies found no causal association between Lp(a) and AF, while 1 revealed an inverse association between these variables. This controversial inverse association was obtained in a study with the smallest sample size, which might have caused some bias. Different or even contradictory results from the same biobank analysis can be surprising. However, it is important to note that the populations presented in Table 2 refer to the population used to obtain Lp(a) levels, and Mendelian randomization needs other studies (not presented in Table 2) to derive genetic associations with AF from an independent validation cohort, often from publicly available genome‑wide association studies (GWAS). Even if the same biobank was used for Lp(a) level analyses, using different GWAS explains the heterogeneity in the obtained results. Overall, the Mendelian randomization studies advocate for the causal association of Lp(a) with AF, contrary to the studies described in the previous section. All studies discussed in this section, along with supplementary information, are presented in Table 2.
Year | Population | Comparison | Methodology | Outcome |
Abbreviations: eMERGE, electronic Medical Records and Genomics; MVP, Million Veteran Program; SNP, single nucleotide polymorphism; UK, United Kingdom; others, see Table 1 | ||||
202033 | 451 933 participants from the UK Biobank | Risk of AF (13 312 cases) vs genetically determined Lp(a) levels | Lp(a) measured by immunoturbidimetric assay | No causal association of Lp(a) with AF |
202134 | 804 507 participants form eMERGE Network, UK Biobank, and MVP cohorts | Risk of AF vs genetically determined Lp(a) levels | Only genetically determined Lp(a) levels based on SNP | ↑ Risk of AF due to high Lp(a) levels |
202135 | 377 600 participants from the UK Biobank | Risk of AF vs genetically determined Lp(a) levels | Lp(a) measured by immunoturbidimetric assay | ↑ Risk of AF due to high Lp(a) levels |
202236 | 435 579 participants from the UK Biobank | Risk of AF (20 432 cases) vs genetically determined Lp(a) levels | Lp(a) measured by immunoturbidimetric assay | ↑ Risk of AF due to high Lp(a) levels |
202237 | 377 590 participants from Neale Lab | Risk of AF vs genetically determined Lp(a) levels | Only genetically determined Lp(a) levels based on SNP | No causal association of Lp(a) with AF |
202138 | 1256 individuals | Risk of AF vs genetically determined Lp(a) levels | Lp(a) measured in serum by particle‑enhanced turbidimetric immunoassay | Lp(a) inversely associated with the risk of AF |
202439 | 273 896 participants from Neale Lab | Risk of AF vs genetically determined Lp(a) levels | Data on Lp(a) measurements unavailable |
|
Lipoprotein(a) as a predictor of thromboembolic events in patients with atrial fibrillation
Igarashi et al40 recruited 172 patients with NVAF. They divided them into 2 groups of thromboembolic (patients with a recent embolic event or a thrombus in the LA found on transesophageal echocardiography [TEE]) and nonthromboembolic. The patients from the thromboembolic group had higher Lp(a) concentrations than those from the nonthromboembolic group. Further analysis showed that Lp(a) concentration equal to or above 30 mg/dl was an independent predictor of thromboembolism in the NVAF patients.40 Yan et al41 evaluated the use of Lp(a) in assessing the risk of thrombotic events among NVAF patients with low CHA2DS2-VASc scores. They included 595 patients and divided them into 2 groups based on the incidence of thrombotic events. The study showed that the patients who experienced thrombotic events had higher Lp(a) concentrations than those who did not experience such events. The authors also found that Lp(a) level was an independent risk factor for thrombotic events, as assessed in the multivariate logistic regression.41
Song et al42 conducted a large cross‑sectional study including 16 357 patients suffering from NVAF. They analyzed the association between Lp(a) levels and the risk for ischemic stroke and systemic embolism incidence in patients grouped according to Lp(a) level quartiles. An increase in Lp(a) level was found to increase the risk of both conditions, suggesting its potential role in the pathogenesis of thromboembolism. Guo et al43 evaluated the possible role of Lp(a) as a predictive factor for stroke in 301 NVAF patients. The patients were divided into 2 groups based on the occurrence of acute ischemic stroke during follow‑up. The patients from the stroke group had a higher Lp(a) concentration than those from the nonstroke group. The authors constructed a nomogram model for predicting acute ischemic stroke in elderly patients with NVAF. In addition to Lp(a) concentration, neutrophil‑to‑lymphocyte ratio, red cell distribution width (RDW), systolic pressure, history of stroke, hyperlipidemia, and high‑density lipoprotein cholesterol concentration were included in the model. This model was more effective at predicting stroke than the CHA2DS2-VASc score, when assessing the area under the receiver operating characteristic curve.43 Hou et al44 retrospectively analyzed 313 NVAF patients, dividing them into 2 groups based on the occurrence of acute ischemic stroke during follow‑up. They found that Lp(a) concentration was higher in the patients who developed acute ischemic stroke. The authors also showed that the CHA2DS2-VASc‑60 score combined with Lp(a) and RDW predicted the occurrence of stroke better than the CHA2DS2-VASc‑60 score alone.44 The reports by Guo et al43 and Hou et al44 were conducted in the same hospital during a similar period, and they analyzed similar research problems. Thus, caution is required when extrapolating the results to other institutions. Furthermore, Zhang et al45 retrospectively analyzed 2258 AF patients using the propensity score matching method to create 2 groups of patients who experienced stroke and those who did not. They found that the first group had higher levels of Lp(a). Moreover, Lp(a) levels above 30 mg/dl were associated with an increased risk of stroke in the unadjusted model.45
All presented studies found some association between the risk of thromboembolic events and the high level of Lp(a). Some works showed an increased concentration of Lp(a) in the subgroup of patients who experienced thromboembolic events. However, this does not necessarily indicate causality, and may only be an indicator. Two studies concluded that high Lp(a) levels are an independent risk factor for thromboembolism / stroke. Nevertheless, the findings in this field require further exploration to clarify the mechanisms underlying this association. All studies discussed in this section, along with supplementary information, are presented in Table 3.
Year | Population | Comparison | Methodology | Outcome |
Abbreviations: see Table 1 | ||||
200040 | 172 nonanticoagulated NVAF patients | 2 groups: 1) thromboembolic (n = 34), 2) nonthromboembolic (n = 138) | Lp(a) measured in serum by latex‑enhanced turbidimetric immunoassay |
|
201941 | 595 NVAF patients | 2 groups: 1) with thrombotic events (n = 68), 2) without thrombotic events (n = 527) | Data on Lp(a) measurements unavailable |
|
202242 | 16 357 NVAF patients | Patients divided into 4 groups by quartiles of Lp(a) concentration | Lp(a) detected using an automated blood analyzer | ↑ Lp(a) associated with ischemic stroke and systemic embolism |
202443 | 301 NVAF patients | 2 groups: 1) stroke (n = 143), 2) nonstroke (n = 158) | Data on Lp(a) measurements unavailable | ↑ Lp(a) in the stroke group |
202444 | 313 NVAF patients | 2 groups: 1) stroke (n = 150), 2) nonstroke (n = 163) | Data on Lp(a) measurements unavailable | ↑ Lp(a) in the stroke group |
202445 | 2258 AF patients | 2 groups: 1) stroke (n = 1129), 2) nonstroke (n = 1129) | Lp(a) measured in serum by latex‑enhanced turbidimetric immunoassay |
|
Lipoprotein(a) correlation with the presence of left atrial thrombus in patients with atrial fibrillation
Igarashi et al46 evaluated 150 patients with AF. The patients underwent TEE and were divided into 2 groups based on the presence of LAT. The patients with LAT had higher Lp(a) concentrations than those without. Moreover, in a multivariate analysis, Lp(a) concentration was found to be an independent positive predictor of LAT.46 Saeed et al47 obtained results that were consistent with those of Igarashi et al.46 They included 50 AF patients divided into 2 groups based on the presence of LAT. It was found that patients with LAT had higher Lp(a) concentrations than the patients without this condition.47 Kamili et al48 performed a cross‑sectional study that included 481 patients suffering from NVAF. They were classified into 2 groups with and without LAT or spontaneous echo contrast (SEC) found on TEE. The study showed that Lp(a) concentrations were higher in the LAT/SEC group than the non‑LAT/SEC group. Moreover, high Lp(a) concentration was an independent predictor of LAT/SEC even after adjustment for propensity score matching. Thus, incorporating Lp(a) and LA diameter into the CHA2DS2-VASc score improved its predictive value for the LAT/SEC.48
All presented studies consistently found that patients with LAT had higher Lp(a) levels. Again, this may not be a causative factor, although consistency within this subject is fascinating and merits further exploration. Table 4 presents all studies discussed in this section, along with supplementary information.
Year | Population | Comparison | Methodology | Study type | Outcome |
Abbreviations: LAT, left atrial thrombus; SEC, spontaneous echo contrast; others, see Table 1 | |||||
199846 | 150 AF patients | Patients divided based on the presence of LAT | Lp(a) measured in serum by latex‑enhanced turbidimetric immunoassay | Case‑control study |
|
200747 | 50 AF patients | Patients divided based on the presence of LAT (25 with and 25 without) | Lp(a) measured in serum by immunoturbidimetric method | Case‑control study |
|
202448 | 481 NVAF patients | 2 groups: 1) LAT/SEC (n = 88), 2) non‑LAT/SEC (n = 393) | Data on Lp(a) measurements unavailable | Cross‑sectional study |
|
Discussion
The association between Lp(a) and the incidence of AF remains inconclusive, as studies present conflicting findings. Five works found no association between Lp(a) and AF, while 4 showed increased concentrations of Lp(a) in patients with AF, indicating high Lp(a) level as an independent risk factor for AF. One study presented contradictory findings, where Lp(a) concentrations were lower in the AF patients than in the controls. Several factors can explain these contrary results, and they incorporate differences in study design, techniques used for Lp(a) measurements, and types of population. Hence, this problem needs further investigation. The interplay between ASCVD, Lp(a), and AF is noteworthy. Since Lp(a) is a well‑established causal risk factor for ASCVD, its increased levels lead to the development of CAD, a risk factor for AF. Consequently, increased Lp(a) levels in AF patients may only be associated with the underlying CAD, not AF per se.
Outcomes from the Mendelian randomization studies regarding the causal role of increased Lp(a) levels in AF development are also ambiguous. Although 4 studies found that high Lp(a) is a causal risk factor for AF, 2 found no significant association. On the other hand, 1 study concluded that Lp(a) was inversely associated with the risk of AF. These discrepancies may result from different ethnicities of the participants, which is known to affect Lp(a) concentration. Although the overall effect advocates a causal association between high Lp(a) level and AF, it should be interpreted cautiously and requires further research.
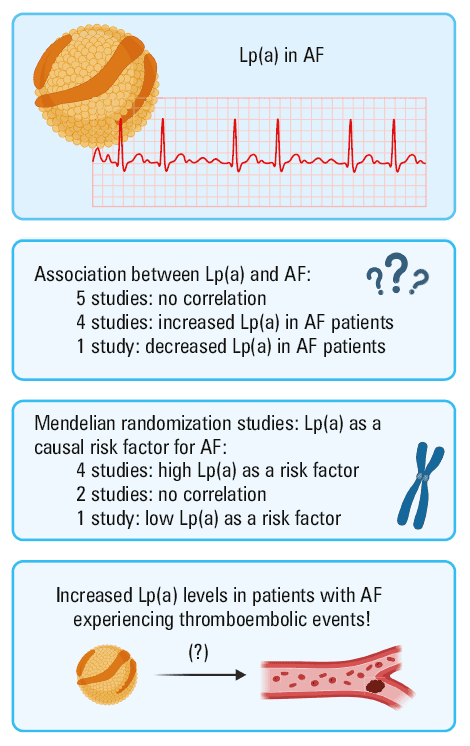
Data from the analyzed studies suggest that patients with AF who experience stroke or other thromboembolic events have higher Lp(a) concentrations than patients who do not experience such events. Some studies found that Lp(a) level was an independent risk factor for thrombotic events in AF patients. Moreover, it was unambiguously shown that Lp(a) concentrations were higher in AF patients with LAT detected on TEE than in AF patients without it. Incorporating Lp(a) into the CHA2DS2-VASc score might improve its performance. Nevertheless, the causality of increased Lp(a) level for thromboembolism was not found in the Mendelian randomization studies, at least within the general population. Thus, it is worth exploring if this causality exists in the subpopulation of AF patients. Figure 2 presents a comprehensive summary of the current knowledge on the role of Lp(a) in AF.
A limitation of this systematic review is the inclusion of different study types, which might have introduced some heterogeneity regarding the assessed outcomes. Additionally, the included studies significantly differ in the population size, which implies the need for cautious interpretation of the presented results. Data gathered in Tables 1, 2, 3, 4 and the quality assessment provided in Supplementary material, Table S2 should allow for a more meaningful and in‑depth interpretation and understanding of the results.
In conclusion, Lp(a) is a fascinating subject of investigation, and existing evidence suggests it may play a pathophysiological role in patients with AF, especially those who experience thromboembolic events. It could be an additional tool for estimating the risk of thromboembolic complications if further validated. Nevertheless, this field requires further research to draw unambiguous conclusions prior to its application in clinical practice. It would be beneficial to conduct a large prospective cohort study that includes healthy individuals with Lp(a) levels measured at baseline and to assess the association between those Lp(a) levels and the first AF occurrence in a long‑term observation. It is essential to use appropriate assays for Lp(a) measurements, as indicated in the EAS consensus statement (2022).15
- Lippi G, Sanchis‑Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. 2021; 16: 217‑221. | Crossref
- Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio‑Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021; 42: 373‑498. | Crossref
- Kornej J, Börschel CS, Benjamin EJ, et al. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. 2020; 127: 4‑20. | Crossref
- Lau DH, Nattel S, Kalman JM, et al. Modifiable risk factors and atrial fibrillation. Circulation. 2017; 136: 583‑596. | Crossref
- Turakhia MP, Shafrin J, Bognar K, et al. Estimated prevalence of undiagnosed atrial fibrillation in the United States. PLoS One. 2018; 13: e0195088. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION