Ambient air pollution and a risk of hospital admission due to acute and chronic coronary syndromes: a time-stratified case-crossover study in the 3 largest urban agglomerations in Poland
Key words: acute coronary syndromes, air pollution, chronic coronary syndromes, PM10, PM2.5

 CC BY 4.0
CC BY 4.0
Ambient air pollution and a risk of hospital admission due to acute and chronic coronary syndromes: a time-stratified case-crossover study in the 3 largest urban agglomerations in Poland
Introduction: Short‑term exposure to air pollution may worsen the course of ischemic heart disease (IHD), causing acute and chronic coronary syndromes.
Objectives: This study aimed to assess the risk of hospital admission due to chronic coronary syndromes (CCSs) and acute coronary syndromes (ACSs) after exposure to various air pollutants in Poland.
Patients and methods: This time‑series study evaluated the risk of hospital admission due to IHD over 3 days from exposure to several air pollutants. A distributed lag nonlinear modelling was used to determine the counts of hospital admissions due to CCSs and ACSs. Data for the 3 largest urban agglomerations in Poland between 2012 and 2017 were collected.
Results: Within the study period, there were 88 467 admissions due to CCSs and 35 403 admissions due to ACSs. After adjusting for meteorological variables, the risk of admission due to CCSs increased after the exposure to particulate matter (PM) of aerodynamic diameter no greater than 10 µm (PM10; cumulative rate ratio [CRR] per 10 µg/m3, 1.007; 95% CI, 1.002–1.012), of diameter no greater than 2.5 µm (PM2.5; CRR per 10 µg/m3, 1.008; 95% CI, 1.001–1.014), and NO2 (CRR per 10 µg/m3, 1.037; 95% CI, 1.026–1.047). The risk of admission due to ACSs was increased after exposure to PM10 (CRR per 10 µg/m3, 1.009; 95% CI, 1.002–1.015) and PM2.5 (CRR per 10 µg/m3, 1.009; 95% CI, 1.001–1.018), whereas the association for the gaseous pollutants, NO2 and SO2, was less pronounced, that is, CRR per 10 µg/m3, 1.012; 95% CI, 0.998–1.026 and CRR per 10 µg/m3, 1.032; 95% CI, 0.998–1.067, respectively.
Conclusions: The exposure to PM10, PM2.5, and NO2 is associated with an increased short‑term risk of hospital admission due to ACSs and CCSs.
What's new?
Air quality in Polish cities is among the worst in Europe. Previous studies reported that air pollution is an important risk factor for cardiovascular diseases, including ischemic heart disease (IHD). This study used the largest dataset to date in Poland to assess the changes in the risk of chronic and acute exacerbations of IHD following exposure to several air pollutants. We found that the risk of hospital admission due to chronic and acute IHD events increased within 3 days of exposure to particulate matter of an aerodynamic diameter no greater than 10 µm (PM10) and no greater than 2.5 µm (PM2.5). Moreover, exposure to nitrogen dioxide was associated with an increased risk of chronic events. Our results provide further evidence to substantiate the need to improve air quality in Poland.
Introduction
Ischemic heart disease (IHD) affects 126 million people worldwide and accounts for 9 million deaths annually, with a particularly high disease burden in Eastern European countries.1-3 The disease is progressive and can become unstable, causing acute coronary syndromes (ACSs), such as myocardial infarction (MI) and heart failure.4,5 However, most clinical presentations of IHD can be classified as chronic coronary syndromes (CCSs), which are typically associated with chest pain and / or dyspnea on exertion that can be relieved with rest and medications.6
The main risk factors for IHD include age, male sex, hypertension, diabetes, dyslipidemia, obesity, and smoking.7 Arterial hypertension is one of the key causes of circulatory system diseases in general,8 having the greatest impact on the incidence of human deaths worldwide, and air pollution is also among the factors contributing to arterial hypertension. However, air pollution emerges as the most important environmental risk factor for IHD.9 Chronic exposure to air pollution increases oxidative stress and inflammation, which lead to the development of IHD risk factors.9,10 Epidemiologic studies showed that long‑term exposure to particulate and gaseous air pollutants is associated with an increased prevalence of IHD.11 In addition, exposure to air pollution may lead to coronary vasomotor abnormalities and plaque destabilization, causing ACSs and CCSs.9,12-15 Indeed, meta‑analyses of epidemiologic studies showed that exposure to both particulate matter (PM) of an aerodynamic diameter no greater than 2.5 µg (PM2.5) and to NO2 was associated with an increased short‑term risk of IHD events.16-19 Air pollution can also affect the risk of atrial fibrillation (AF). It is the most common heart rhythm disorder, and during smog incidents, the frequency of AF episodes in the population is noted to increase.20
In Poland, both IHD and air pollution are important public health issues. IHD is the leading cause of morbidity and mortality, accounting for 10% of all deaths.21 In Poland, recently reported number of deaths from IHD was 16.9 per 10 000 population,22 whereas air quality in Polish cities is among the worst in Europe: nearly half of the 50 most polluted European cities are in Poland.23 However, the association between exposure to ambient air pollution and the burden of IHD in Poland has been so far only partially elucidated.24-27 Therefore, we conducted a time‑stratified case‑crossover study to assess the link between ambient air pollution and the risk of hospital admission due to IHD.
Patients and Methods
Setting and definitions
We assessed hospital admissions due to IHD in the 3 largest agglomerations in Poland: Tricity (population, 0.75 million; northern Poland, at the Baltic coast), Warsaw (population, 1.8 million; central Poland), and Kraków (population, 0.77 million; southern Poland). The study was conducted from January 1, 2012 to December 31, 2017.
Hospital admissions due to IHD were defined as those billed with the following codes from the International Classification of Diseases, Tenth Revision (ICD‑10): I20 (IHD), I21 (acute MI), I22 (subsequent MI), I23 (certain current complications following acute MI), I24 (other acute IHD), and I25 (chronic IHD). The daily admission counts were obtained from the National Health Fund, which is the only public health care insurer in Poland. The data on admissions regarded only adult patients and included all hospitals in the 3 cities within the study period.
The mean daily concentrations of PM10, PM2.5, NO2, and SO2, and the mean daily values of temperature, relative humidity, precipitation, and ambient air pressure were obtained from the Chief Inspectorate of Environmental Protection.28 For each city, we averaged the values from all available stations.
The study analyzed aggregated data and therefore did not require an approval of a bioethics committee.
Statistical analysis
The I20 and I25 codes were assessed together because they are used interchangeably to refer to CCSs. Likewise, the I20, I21, I23, and I24 codes were grouped together as denoting ACSs. We used a time‑stratified case‑crossover analysis to compare exposures on case days with exposures on control days (ie, in each city, control days were on the same day of the week in the same month and year as the case days). The differences in admission counts on the case and control days were related to differences in exposure to air pollutants by the conditional quasi‑Poisson regression.29 The “gnm” package was used to fit the conditional quasi‑Poisson models. We used a stratum variable of “city‑year‑month‑day‑of‑the‑week” to control for a long‑term trend and seasonality in admission counts and concentrations of pollutants. The stratification also allowed us to pool data from the 3 cities.30,31
We combined this case‑crossover analysis with distributed lag linear‑nonlinear modeling (DLNM) to assess the risk of hospital admission up to day 2 from exposure in single‑pollutant models.32 The use of DLNM allowed us to model nonlinear and delayed effects of air pollutants and meteorological variables. Considering that any concentration of the tested pollutants may be harmful, we assumed a linear relationship between pollutant concentrations and the risk of admission, with no threshold. Based on our previous experience,33 the lag in the DLNM models was modelled with a polynomial function and 3 degrees of freedom (df), whereas covariates, including temperature, relative humidity, and atmospheric pressure, were modelled with natural cubic splines (df = 2) and a lag of 1 day. The results were presented as rate ratios (RRs) per 10 µg/m3 for each day after exposure, including cumulative effects. Cumulative RRs (CRRs) were forward looking. We calculated the percentages of hospitalizations attributable to the individual air pollutants with the “FluMoDL” package.34 Medians with interquartile ranges were used as descriptive statistics for pollutant concentrations and meteorological variables. Significance of the results was evaluated with 95% CIs. A P value below 0.05 was considered significant. All calculations were completed in the R software version 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Air pollution and admissions
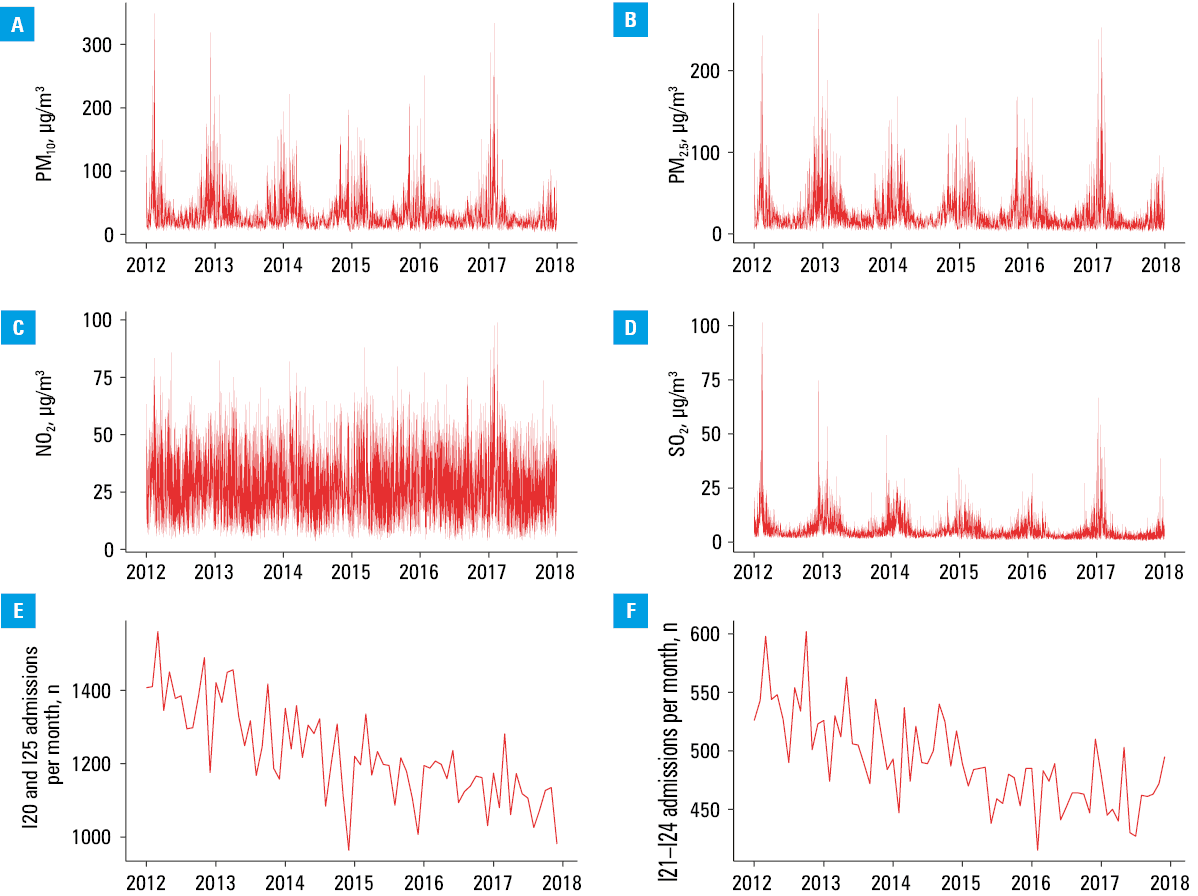
The daily concentrations of all air pollutants were the highest in the winter and the lowest in the summer (Figure 1A–1D). The mean concentrations of all air pollutants were the highest in Kraków and the lowest in Tricity (Table 1).
Characteristic | Kraków (n = 2192)a | Tricity (n = 2192)a | Warsaw (n = 2192)a |
Data are presented as median (interquartile range) unless provided otherwise.
a Total number of days for which daytime measurements were considered
Abbreviations: see Figure 1 | |||
PM10, μg/m3 | 35 (23–57) | 15 (11–21) | 27 (20–39) |
PM2.5, μg/m3 | 25 (17–44) | 10 (7–15) | 21 (15–32) |
NO2, μg/m3 | 40 (33–48) | 14 (9–19) | 34 (27–42) |
SO2, μg/m3 | 5.5 (4–9.3) | 2.5 (1.8–3.8) | 4.8 (3.1–7.2) |
Temperature, °C | 10 (3–17) | 9 (4–16) | 9 (3–17) |
Relative humidity, % | 78 (68–86) | 74 (67–80) | 77 (65–87) |
Atmospheric pressure, hPa | 988 (984–992) | 1007 (1002–1012) | 1003 (998–1008) |
Chronic coronary syndromes, n | 17 340 | 11 683 | 59 444 |
Acute coronary syndromes, n | 10 062 | 5420 | 19 921 |
The total admission counts for each ICD‑10 code were as follows: I20, 29 044; I21, 33 551; I22, 183; I23, 116; I24, 1553; and I25, 59 423. The monthly admission counts for CCSs and ACSs decreased steadily over the study period (Figure 1E and 1F).
Lagged association of exposure to PM10, PM2.5, NO2, and SO2 with a risk of hospital admission
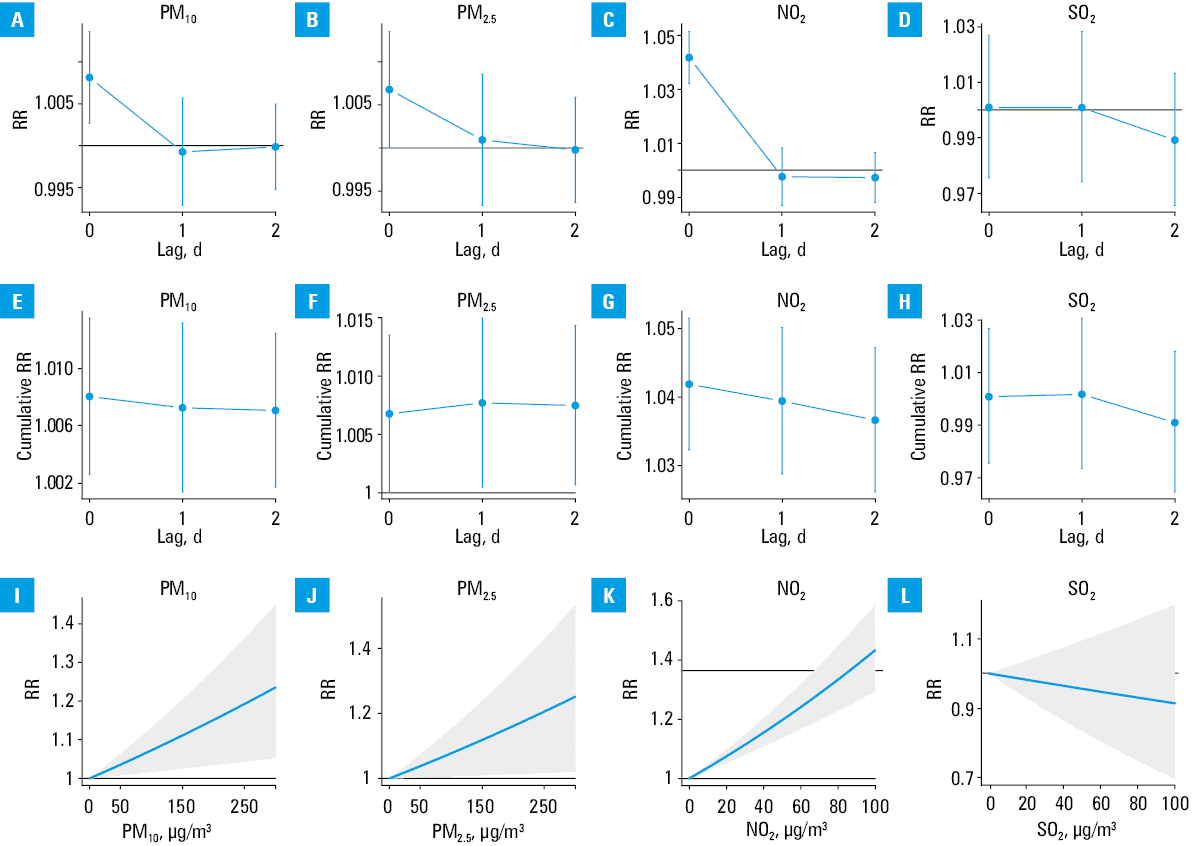
After adjusting for meteorological variables, the risk of admission due to CCSs increased following the exposure to PM10 (CRR per 10 µg/m3, 1.007; 95% CI, 1.002–1.012), PM2.5 (CRR per 10 µg/m3, 1.008; 95% CI, 1.001–1.014), and NO2 (CRR per 10 µg/m3, 1.037; 95% CI, 1.026–1.047). In contrast, the exposure to SO2 was not associated with the risk for admission due to CCSs (CRR per 10 µg/m3, 0.991; 95% CI, 0.965–1.018). The daily and cumulative RRs for admission due to coronary syndromes and the relationship between pollutant concentrations and the admission risk are shown in Figure 2.
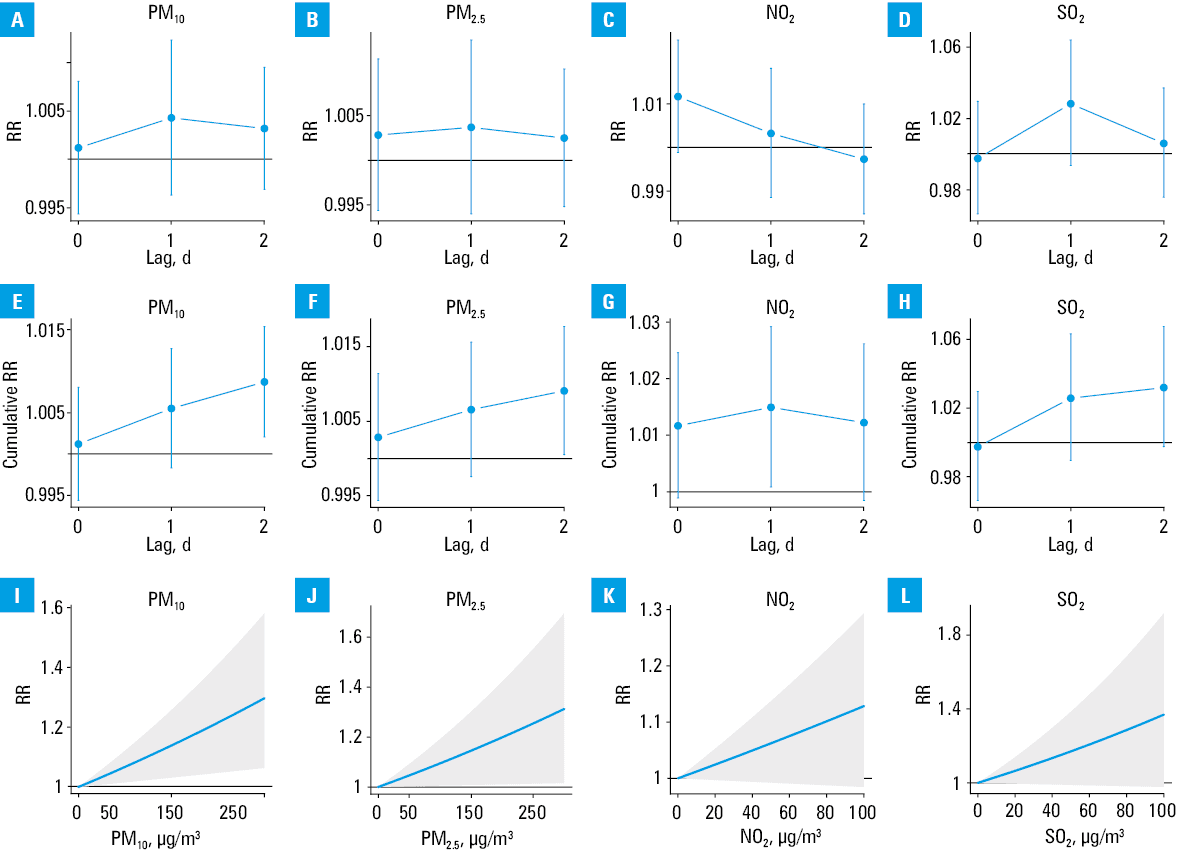
After adjusting for meteorological variables, the risk of admission due to ACSs increased during the 3 days from the exposure to PM10 (CRR per 10 µg/m3, 1.009; 95% CI, 1.002–1.015) and PM2.5 (CRR per 10 µg/m3, 1.009; 95% CI, 1.001–1.018). The risk increased on the day of exposure to NO2 and on the first day after exposure to SO2, but the lower limits of 95% CI for CRRs over 3 days were slightly below the value of no effect, that is, CRR per 10 µg/m3, 1.012; 95% CI, 0.998–1.026 for NO2 and CRR per 10 µg/m3, 1.032; 95% CI, 0.998–1.067 for SO2. The daily and cumulative RRs for admission due to ACSs and the relationship between pollutant concentrations and the admission risk are shown in Figure 3.
In single‑pollutant models, the exposure to PM10 and PM2.5 accounted for 1.9% to 2.9% of admissions due to CCS or ACS, whereas the exposure to NO2 accounted for 11.7% of admissions due to CCSs (Table 2).
Variable | Pollutant | Admission percentage (95% CI) |
Only significant associations are presented.
Abbreviations: see Figure 1 | ||
Chronic coronary syndromes | PM10 | 2.3 (0.7–4.1) |
PM2.5 | 1.9 (0.2–3.5) | |
NO2 | 11.7 (8.6–14.6) | |
Acute coronary syndromes | PM10 | 2.9 (0.7–4.8) |
PM2.5 | 2.4 (0.1–4.5) | |
Discussion
In this study, we assessed over 100 000 hospital admissions due to ACSs or CCSs in the 3 largest urban agglomerations in Poland. The analysis showed that exposure to particulate and gaseous air pollutants was associated with an increased short‑term risk of IHD events requiring in‑hospital care. The risk of admission due to CCSs increased significantly after the exposure to PM10, PM2.5, and NO2 but not SO2. The risk of ACSs increased after the exposure to PM10, PM2.5, NO2, and SO2, but this association was significant only for PM. Over the study period, the counts of hospital admissions due to IHD decreased, which is in line with a decreasing incidence of IHD in Poland.35 The diminished correlation between SO2 concentrations and hospital admissions for ACS and CCS may be attributed to a substantial reduction in SO2 levels observed approximately a dozen or so years ago. In recent years, SO2 concentrations have stabilized at very low levels,36 consistently below the World Health Organization guidelines.37 Therefore, they do not significantly impact health deterioration. However, there are geographic differences in SO2 concentrations, as noted in the cities we examined, with the highest levels in Kraków and the lowest in the Tricity area.
Our findings are largely in line with previous evidence. The seminal HEAPSS study (Health Effects of Air Pollution among Susceptible Sub‑populations), conducted in several European cities, showed that exposure to PM10, NO2, and carbon monoxide was associated with a significantly increased risk for same‑day hospital readmission among MI survivors.38 In Bulgaria, hospitalization risk for IHD (I20–I25) increased after the exposure to NO2 but not to PM10, PM2.5, and SO2.39 A nationwide crossover study from China reported that the hospitalization risk due to IHD (I20–I25, about 400 000 cases) increased over 3 days after exposure to PM2.5 (0.42% per 10 µg/m3), PM10 (0.26% per 10 µg/m3), NO2 (2.56% per 10 µg/m3), and SO2 (0.51% per 10 µg/m3).40 Likewise, another study from China showed that the risk of death due to acute MI was significantly increased after short‑term exposure to PM10, PM2.5, NO2, and SO2.41
A study of nearly 140 000 MIs in Japan reported that the risk of hospital admission increased after the exposure to PM2.5 (odds ratio [OR], 1.06 per 10 µg/m3 over 2 days), but the effect of gaseous pollutants was not investigated.42 In Changzhou, China, the exposure to PM2.5 and PM10, but not to NO2 and SO2, was associated with a significantly increased risk of MI.43 However, in another Chinese region, the risk of MI increased significantly after exposure to PM2.5, PM10, NO2, and SO2.44 A study in the United States reported that mortality due to chronic IHD was increased in counties with aerosol particle pollution.45
A previous study in Poland reported that the exposure to PM2.5 and PM10 increased the short‑term risk of hospitalization due to cardiovascular diseases (CVDs; I00–I99).46 However, the authors did not separate ICD‑10 codes for IHD and did not study gaseous pollutants, such as NO2 and SO2. A regional cohort study of 2645 patients in Białystok, Poland, reported that the risk of acute MI (I21) and unstable angina (I20.0) increased after the exposure to NO2 on the day of exposure (OR, 1.02 per an interquartile‑range increase), but the risk of hospitalization did not change noticeably after exposure to PM10, PM2.5, and SO2.47 In contrast, a single‑city study from Kraków reported that the risk of acute MI (I21) increased after exposure to PM2.5 (OR, 1.32 per 10 µg/m3) in all participants, whereas the effect was significant for NO2 (OR, 1.13, at lags 0 and 1 d) only among patients older than 70 years.48 The analysis of nearly 2000 patients with acute MI in the Polish region of Silesia reported that the risk of admission increased significantly on the day of exposure to PM10 (OR, 1.078 per 10 µg/m3) and PM2.5 (OR, 1.099 per 10 µg/m3) but not after the exposure to SO2 and NO2.49
There are several potential mechanisms that can explain how air pollutants may exacerbate IHD in the short term.10 Air pollutants may uncouple the endothelial nitric oxide synthase, leading to the formation of reactive oxygen and nitrogen species. Oxidative stress, in turn, causes vasoconstriction and activates macrophages that release prothrombotic mediators, resulting in thrombosis and platelet activation.50,51 Further research will likely pinpoint new molecular pathways, which could help elucidate the effects of air pollutants on cardiovascular health.
The limitations of our study need to be acknowledged. As we based it on the National Health Fund database, all analyses were carried out for aggregated daily hospital admissions, which did not allow us to investigate whether the relationship between the exposure to air pollutants and the risk of hospital admission differed in the subgroups of patients (age group, sex, comorbidities). Moreover, we could not identify repeated admissions for the same patients or the patients transferred from other hospitals to reference centers. For the same reason, we could not include admissions for the first time in a given patient. When planning future studies in this area, we will consider a prospective approach, which will allow us to identify individual patients and thus also the medical procedures performed on them. However, this will require a completely different way of obtaining data and significantly increased involvement of the research team.
We also had no influence on possible coding errors. The possibility of misclassification of IHD types in hospital records, as well as the inability to include individual patient data, are significant limitations. Combining the so‑called ACSs (I20, IHD; I21, acute MI), I22 (subsequent MI), I23 (certain current complications following acute MI), I24 (other acute IHD) may raise concerns that during coding for the National Health Fund, the person analyzing the documentation will indicate the better scored ACS procedure as the main diagnosis. However, in our approach to data analysis, we assumed that the physicians coding the procedures (cardiologists, internal medicine specialists) were able to correctly recognize ACS, which required treatments typical of this procedure, for example, coronary angiography, coronary balloon angioplasty, or stent implantation in the coronary vessels. Therefore, we would rather not expect major errors in ACS coding. For chronic IHD (I25), symptoms of decompensation requiring hospital admission may be included in the same group as planned admissions related to the need to optimize chronic treatment or treatment of concomitant circulatory system diseases, such as heart failure, AF, etc. We were not able to clearly determine subgroups in the group of patients qualified as I25, based on the collected data. However, since we used the same method of collecting and analyzing data in each of the considered 3 urban agglomerations, we expect that the risk of a significant error is relatively small. However, to avoid such errors, we intend to conduct a prospective research and group the examined patients according to the medical procedures used during their hospital stay, taking into account all diagnoses that the patient received.
In the case of research similar to ours, based on retrospective data, some errors and shortcomings may also result from the imperfections of available registers, including incorrect initial diagnosis, incomplete data, different methods of data collection, or failure to take into account various confounding variables, such as the impact of comorbidities, infections, risk factors for atherosclerosis, etc. Moreover, neither ours nor other studies constructed this way took into account individual exposure to air pollutants or susceptibility of the studied persons, different chemical composition of the pollutants in individual cities related to differences in emission sources, or the summation of the impact of various other pollutants (including, for example, indoor air pollution, which is not included in the studies of ambient air quality, conducted as part of the State Environmental Monitoring by the Chief Inspectorate of Environmental Protection).
Our study has also some strengths. Most previous studies assessed the relationship between exposure to air pollution and hospitalization risk due to CVDs without dedicated analyses for IHD. Moreover, studies that did assess IHD focused on MI only or aggregated all IHD ICD‑10 codes (I20–I25). Contrary to that, we analyzed ACSs and CCSs separately. Another strength of our study is that the 3 agglomerations we investigated account for nearly 10% of Poland’s population, and the dataset we used is the largest to date in Poland. Moreover, we used a time‑stratified case‑crossover design, which reduced confounding by conditioning data specific to the location and a short time window, that is, the control days were the same days of the week, in the same month, and in the same year as the case days.29,30 Such a design also allowed us to account for the long‑term downward trend in hospital admissions due to IHD in Poland over the study period. Moreover, we accounted for the effect of meteorological variables, such as temperature, humidity, and precipitation, which may also increase the risk of IHD events.52-54
As indicated by experts from the World Heart Federation, American College of Cardiology, American Heart Association, and the European Society of Cardiology,55 citing the Global Burden of Disease Study,56 air pollution can be attributed to 20% of all CVD deaths. Our research indicates that air pollution with PM and nitrogen oxides has a short‑term and negative impact on health by increasing the number of ACSs and CCSs. This fact indicates that air pollution has a greater impact on CVD than an improper diet or lack of physical activity. Therefore, not only a patient‑tailored approach is essential for management of CCSs57 but air pollution issues should definitely be included in the national and global strategies for the prevention and treatment of CVD. Experts include the following methods of reducing the negative impact of air pollution on health: 1) informing and educating patients about the harmfulness of air pollution and encouraging them to monitor information about local pollution; 2) avoiding walking and other activities (eg, cycling, rollerblading) along traffic arteries with high traffic volume; 3) planning physical activity in parks and gardens, but not near busy roads and on days when the concentration of pollution increases or conducting physical activity in rooms with an air filtering system on days when air pollution increases; 4) limiting physical activity outdoors, especially by people from risk groups (pregnant women, children, the elderly, and people with chronic circulatory and respiratory diseases); 5) installing ventilation and air filtering systems in apartments, especially in areas with high concentrations of air pollution.
In conclusion, exposure to PM10, PM2.5, and NO2 was associated with an increased short‑term risk of hospital admission due to ACSs and CCSs in Poland. Our findings add to the evidence linking air pollution with disease burden in Poland.33,58,59
- Movsisyan NK, Vinciguerra M, Medina‑Inojosa JR, et al. Cardiovascular diseases in Central and Eastern Europe: a call for more surveillance and evidence‑based health promotion. Ann Glob Health. 2020; 86: 21. | Crossref
- Murphy A, Johnson CO, Roth GA, et al. Ischaemic heart disease in the former Soviet Union 1990‑2015 according to the Global Burden of Disease 2015 Study. Heart. 2018; 104: 58‑66. | Crossref
- Khan MA, Hashim MJ, Mustafa H, et al. Global epidemiology of ischemic heart disease: results from the global burden of disease study. Cureus. 2020; 12: e9349. | Crossref
- Bhatt DL, Lopes RD, Harrington RA. Diagnosis and treatment of acute coronary syndromes: a review. JAMA. 2022; 327: 662‑675. | Crossref
- Jensen RV, Hjortbak MV, Bøtker HE. Ischemic heart disease: an update. Semin Nucl Med. 2020; 50: 195‑207. | Crossref
ARTICLE INFORMATION