Vitamin C for the common cold and pneumonia
1 ,2
Key words: COVID-19, meta-analysis, randomized trial, respiratory tract infection, sepsis
,2
Key words: COVID-19, meta-analysis, randomized trial, respiratory tract infection, sepsis

 CC BY 4.0
CC BY 4.0
Vitamin C for the common cold and pneumonia
This paper provides an overview of the efficacy of vitamin C for preventing and treating respiratory infections. Studies in a wide variety of animals have shown vitamin C to be protective against infections. In controlled trials in the general human population, vitamin C at a dose greater than 1 g/day did not prevent common colds. However, in 5 trials with participants undertaking heavy physical activity, vitamin C halved the incidence of colds. In 15 trials (n = 6244), regular supplementation of 1 g or more of vitamin C per day decreased the severity of colds by 15%.
Results: of therapeutic trials in which vitamin C was initiated after the onset of common cold symptoms have been inconsistent. However, 2 therapeutic trials found that 6–8 g/day of vitamin C was twice as effective at reducing the duration of colds as 3–4 g/day. In 3 controlled trials, vitamin C was shown to prevent pneumonia, but the contexts were atypical: the participants were schoolboys attending a boarding school in the United Kingdom before World War II, soldiers hospitalized for influenza A, and United States Marine recruits. It is unlikely that vitamin C would reduce the risk of pneumonia in the general population; however, 4 trials reported a treatment benefit for pneumonia patients, although the findings encourage further research rather than providing firm evidence of efficacy. Vitamin C has been tested for efficacy in COVID‑19 and sepsis with conflicting results. Given the evidence that vitamin C reduces the severity and duration of the common cold, paired with its good safety profile and low cost, it is not unreasonable for patients to test whether therapeutic vitamin C supplementation at a dose of 6–8 g/day is beneficial at the individual level.
Introduction
In animal studies, vitamin C administration has been shown to have protective effects against diverse viral and bacterial infections. According to a systematic review published in 2006, more than half of 148 identified animal studies reported a significant benefit (P <0.01) of vitamin C administration for infectious diseases (Table 1).1,2 A large proportion of the studies were carried out in guinea pigs, which is informative, given that both guinea pigs and humans require dietary vitamin C. Nevertheless, benefits were found across the animal kingdom. For example, in animal models, influenza led to higher lung inflammation scores at 1 week with vitamin C deficiency,3 and vitamin C decreased mortality due to parainfluenza infection.4
Category | Number of studies in the category | Number of studies with a benefit in any infectious disease outcome (P <0.01) |
This table is based on data collected and analyzed in Appendi × 2 of 1, with an earlier version summarizing the findings in 2. | ||
All studies | 148 | 86 |
Animal species | ||
Guinea pig | 36 | 21 |
Rat, mouse, gerbil, hamster | 40 | 24 |
All mammals | 100 | 58 |
Birds | 13 | 8 |
Fish | 35 | 20 |
Etiological agent | ||
Tuberculosis (TB) | 8 | 3 |
Bacteria (non‑TB) | 70 | 36 |
Bacterial toxin | 19 | 16 |
Virus | 22 | 12 |
Candida albicans | 6 | 4 |
Protozoa | 23 | 15 |
In humans, several infections, such as the common cold, COVID‑19, and pneumonia, cause a decrease in vitamin C levels.1,2,5-12 As compared with plasma levels, the level of vitamin C in white blood cells is about 100‑fold higher, indicating that vitamin C has a role in these immune cells.13 Vitamin C has diverse effects on the immune system (Supplementary material, References). Taking the evidence‑based medicine approach, this review focuses on clinically relevant findings.
Alongside water‑soluble vitamin C, lipid‑soluble vitamin E should be considered, as these 2 antioxidants interact—vitamin C transforms oxidized vitamin E back to the reduced form.1,5,6 In a large randomized controlled trial (RCT) involving 29 133 Finnish men followed for 6 years, the effect of vitamin E on the risk of pneumonia was significantly modified by smoking, leisure‑time physical activity, weight, and dietary vitamin C intake, demonstrating heterogeneity in vitamin E effects between population groups.1,14,15 Direct extrapolation of these findings to vitamin C is not justified; however, the notion that various factors can modify the effects of antioxidants is important when narrowing down broad generalizations from individual trials, irrespective of whether the finding is positive or negative, and whether or not the trial is large and methodologically sound. Thus, although meta‑analyses of similar vitamin C trials are informative, caution is needed in extrapolation of the findings to other contexts.
The literature was systematically searched for trials on vitamin C for 2 Cochrane reviews on the common cold and pneumonia published by 2013.5,6 We also carried out a systematic search for trials on vitamin C and the common cold in 2023.16 These searches have since been updated to cover the recent literature. Unless stated otherwise, we show 1‑tailed P values for testing comparisons of vitamin C with controls. In Supplementary material, we include additional information, our calculations, and additional links to references.
The common cold
After the identification of vitamin C in the 1930s, reports appeared arguing that it was beneficial against the common cold.17-20 After World War II, the Sheffield trial21 examined the effects of vitamin C deprivation and found that it increased the length of colds.
In 1971, Linus Pauling22 published a meta‑analysis—one of the very first in medicine—in which he pooled the results of 4 placebo‑controlled trials on vitamin C for the common cold, and concluded that it was highly unlikely that the reported benefits could be explained by chance alone (P <0.001).22 Pauling had a high profile, having earlier won 2 Nobel Prizes (Chemistry and Peace), and so his interest in this field inspired many further RCTs on vitamin C and the common cold being carried out in the 1970s.1,2,5 The main findings of the 4 largest RCTs are shown in Table 2.23-26
Trial | Study characteristics | Outcome | Effect of vitamin C | P value |
In all these trials, vitamin C was administered regularly, that is, each day over the 2- to 4‑month trial. Comparisons without P value are not significantly different. See the Supplementary material for explanations and calculations.
a Pitt and Costrini25: “the placebo Tablets were formulated from citric acid and were indistinguishable in appearance and taste from the vitamin C Tablets.” After the trial, the participants were asked which pill they thought they were taking. Forty out of 674 patients (5.9%) were able to infer their treatment correctly by subjective observations indicating physiological effects (see p. 26 in 1 for data background).
b Anderson et al26 administered 3 g/day extra for 3 days when the participant had a cold. In the vitamin C group, 26% were free of any illness during the trial, as compared with 18% in the placebo group, a difference of 7.3 percentage points (see p. 44 in 1 for data background). The difference in vitamin C effect between those who had and did not have contact with young children was significant (2‑tailed P = 0.02), as was the difference between those who had or did not have frequent colds (2‑tailed P = 0.02).2,16 The trial lasted for about 4 months, so the estimates relate to that period. | ||||
Elwood et al23 (1976) |
| Incidence of “chest colds” | –18% | 0.01 |
Incidence of “simple [nasal] colds” | +1% | – | ||
Duration of colds | –5% | – | ||
Ludvigsson et al24 (1977) |
| Incidence of “cold symptoms from the nose” | +7% | – |
Duration of nasal symptoms per episode | +6% | – | ||
Incidence of “absence from school because of colds” | +3% | – | ||
Days of absence from school per episode | –14% | 0.008 | ||
Pitt and Costrini25 (1979) |
| Incidence of colds | +1% | – |
Duration of colds | –3% | – | ||
Severity of colds | –10% | 0.01 | ||
Incidence of pneumonia | –85% | 0.02 | ||
Proportion of participants who identified vitamin C by subjective observationsa | 5.9% | 0.007 | ||
Anderson et al26 (1972) |
| Incidence of “throat colds” | –21% | 0.005 |
Incidence of “nose colds” | –2% | – | ||
Duration of symptoms per episode | –5% | – | ||
Confined to house per episode, d | –21% | 0.008 | ||
Confined to house per person, d | –30% | <0.001 | ||
Proportion of participants free of any illness during the trialb | 7.3% | 0.006 | ||
Confined to house per person during the follow‑up | ||||
Contacts with young childrenb | –1.12 d | <0.001 | ||
No contacts with young children | –0.26 d | |||
Frequent coldsb | –0.98 d | <0.001 | ||
Infrequent colds | –0.2 d | |||
In 2013, we published a Cochrane review in which we included placebo‑controlled trials that had investigated administration of ≥0.2 g/day of vitamin C.5,27,28 Based on data from 24 trials with 10 708 participants from the general population, there was strong evidence that vitamin C did not prevent colds, with a risk ratio [RR] of 0.97 (95% CI, 0.94–1.00).5 In another meta‑analysis restricted to the 6 largest RCTs with a vitamin C dose ≥1 g/day (5480 cold episodes), the numbers of colds were equal in the vitamin C and placebo groups.29,30 Thus, vitamin C does not have an effect on the average incidence of colds in the general community. However, the picture is more complex than indicated by the narrow confidence intervals. There is strong evidence that vitamin C can prevent colds in specific circumstances.
Vitamin C halved the rate of the common cold in 5 RCTs with 598 participants undertaking heavy short‑term physical activity, such as running or skiing (Figure 1).5,31-36 The number‑needed‑to‑treat in these 5 trials ranged from 3 to 10 (Table 3). Exercise causes oxidative stress, and the benefit may be explained by the antioxidant effect of vitamin C.1,2,5
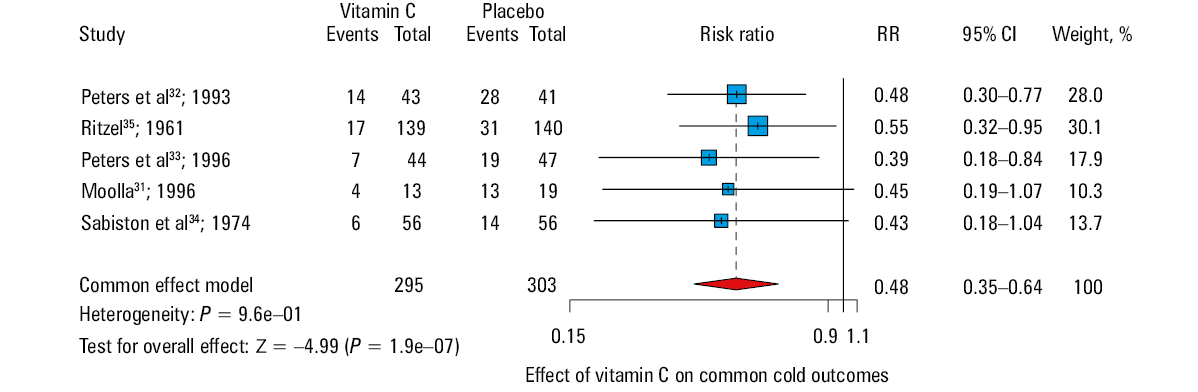
Trial | Incidence of colds, % | NNT from the results | NNT from RR = 0.48 | ||
Vitamin C | Placebo | Difference | |||
a Number needed to treat (NNT): how many people need to be treated to prevent 1 case of the common cold. For example, in the first row, NNT = 1/0.38 =2.7. The NNT in the right‑hand column is calculated from the inverse of the (1 – RR) × placebo group incidence. This gives a more accurate estimate for NNT if we assume that the pooled RR applies to all 5 contexts.
Abbreviations: see Figure 1 | |||||
Moolla31 (1996) | 31 | 68 | 38 | 2.7 | 3 |
Peters et al32 (1993) | 33 | 68 | 36 | 2.8 | 3 |
Peters et al33 (1996) | 16 | 40 | 25 | 4.1 | 5 |
Sabiston34 (1974) | 11 | 25 | 14 | 7 | 8.2 |
Ritzel35 (1961) | 12 | 22 | 10 | 10.1 | 9.2 |
In another context, 4 placebo‑controlled trials from the 1940s to 1970s found that vitamin C prevented colds in British men, with a pooled RR estimate of 0.70 (95% CI, 0.60–0.81).1,29,30 According to surveys, in the 1970s, the British diet was low in vitamin C (around 0.04 g/day), and the United Kingdom (UK) recommendation for vitamin C intake was the lowest in Europe. Three of the UK trials estimated that dietary intake ranged from 0.015 to 0.05 g/day.29,37-39 The benefit in this group is not explained by high vitamin doses, but by particularly low dietary intakes. The lowest vitamin C supplementation dose was just 0.08 g/day in the trial by Baird et al,39 which reported a decrease in common cold incidence by 37% (95% CI, 22%–50%).29,39 In line with the potential benefit for people with low dietary vitamin C intake, Anderson et al26 found that the effect of vitamin C was greater on the participants who had a low intake of fruit juices, an important source of vitamin C. Low dietary vitamin C is not uncommon. For example, in the United States (US), 5% of men have a vitamin C intake of less than 0.05 g/day,40 and in many countries, the proportion of men with a low vitamin C intake is much higher.
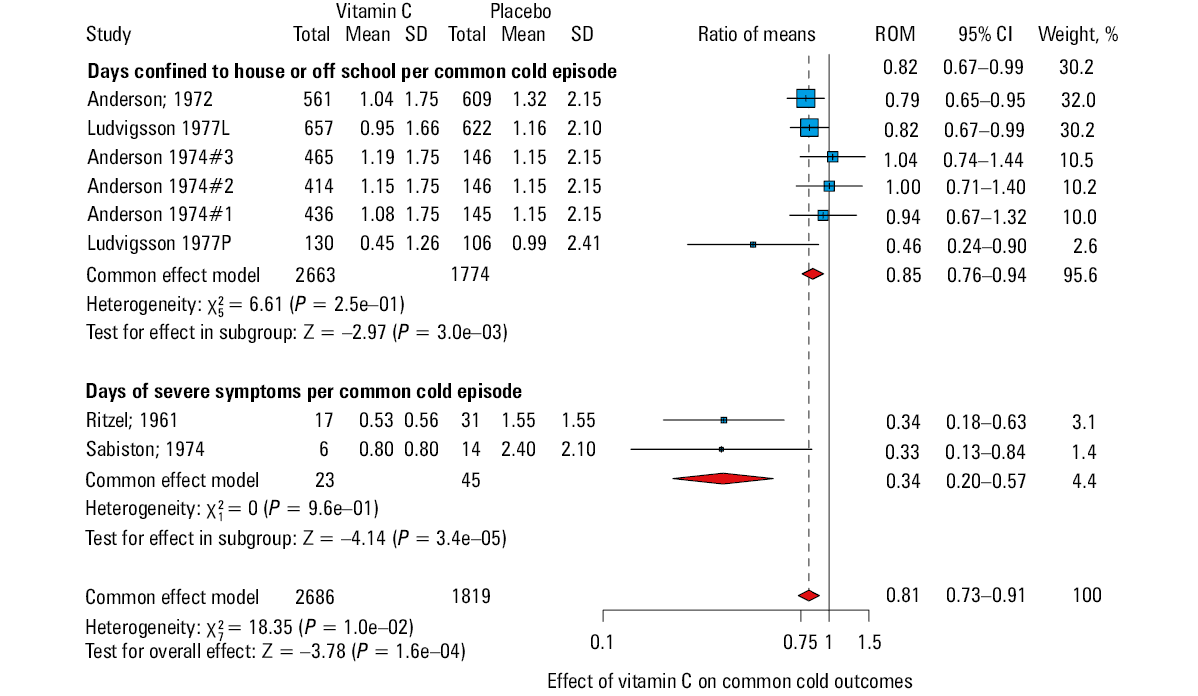
In contrast to the variation in the effects of vitamin C on common cold incidence, the effects on common cold duration and severity are more uniform. The 2013 Cochrane review found that in 17 trials with 7215 adults, regular vitamin C supplementation (≥0.2 g/day) shortened the duration of colds by 7.7% (95% CI, 3.7%–12%), and in 10 trials with 1532 children, regular supplementation (≥1 g/day) resulted in a reduction of common cold duration by 18% (95% CI, 9%–27%).5
In the 2023 analysis, we focused on the effect of regular vitamin C supplementation at a dose ≥1 g/day on common cold severity.16 In 15 RCTs with 6244 participants, vitamin C decreased the severity of colds occurring during the supplementation period by 15% (95% CI, 9%–21%) (Figure 2). In a direct comparison of the effect of vitamin C on the total duration of colds and the severity of cold symptoms, there was a significantly greater effect on severity.16
It is also useful to look at the evidence for the impact of vitamin C supplementation on the common cold by context. A substantial proportion of positive results for both incidence and severity of colds were obtained in studies carried out among military personnel and other groups living in similar conditions.41-43 Some comparisons found benefits for men but not for women.29,43,44
A large RCT by Anderson et al26 also found substantial differences in the benefits of vitamin C by other baseline variables. Vitamin C regularly administered at a dose of 1 g/day with a subsequent increase to 4 g/day during a cold was beneficial for those who had previously suffered from frequent colds or had regular contact with children, whereas there was no effect on those who rarely contracted colds or had less frequent contact with children (Table 2).
Although there is strong evidence that vitamin C alleviates and shortens colds when taken regularly, the cost vs benefit does not unequivocally justify year‑round supplementation, as adults only contract about 2 colds per year on average. For people who do not have colds particularly frequently, starting high doses of vitamin C therapeutically, soon after the onset of symptoms, seems more reasonable than taking it regularly. However, findings from the therapeutic high‑dose vitamin C trials are inconsistent.
Three RCTs45-47 demonstrated that therapeutic vitamin C was beneficial, and that there was a dose‑response relationship with a dose up to 6–8 g/day,1,2,5,48-50 but other trials found no benefit.5,49 In therapeutic trials, there are methodological issues that can lead to false negative conclusions, such as starting vitamin C too long after the onset of symptoms, or stopping vitamin administration early.5,49 One therapeutic trial found that taking 6 g/day of vitamin C was beneficial when started within 24 hours of symptoms appearing, but not so if started later.51 In addition, early and abrupt discontinuation of vitamin C caused actual harm to the patients in a few sepsis trials (see section on sepsis). It is noteworthy that none of the therapeutic trials studied children, whereas the regular supplementation studies have on average found a considerably greater benefit for the pediatric population.5,49
In individuals who tend to suffer from colds associated with significant physical exercise, it would be worthwhile testing whether vitamin C has an impact. Given the benefits observed in the regular vitamin C supplementation trials and the abovementioned therapeutic trials, it seems reasonable for common cold patients to take 6–8 g/day of vitamin C divided into several smaller doses immediately after the onset of cold symptoms. Such doses have been used in RCTs, although much higher therapeutic doses (>15–30 g/day) have been proposed.52,53 Nasal application of vitamin C has also been suggested,54 but not tested in RCTs.
Common cold–induced asthma
Given the evidence indicating that vitamin C has a greater effect on the more severe forms of the common cold than on a runny nose,16 it seems plausible that it may impact some of the complications of the common cold. A systematic review identified 3 trials on the possible effects of vitamin C on common cold–induced asthma.55
Anah et al56 studied 41 asthmatic individuals in Nigeria. The participants had histories of exacerbated asthma attacks during the rainy season. In all cases, their attacks were precipitated by respiratory infections, which started with a sore throat and dry cough. The 14‑week trial was conducted during the rainy season. The vitamin C dose was 1 g/day. During the follow‑up, there were 35 asthma attacks in the 19 placebo participants, and 9 attacks in the 22 vitamin C participants, yielding a RR of 0.22 (95% CI, 0.06–0.81). The effect on severe and moderate asthma attacks was even greater, with a RR of 0.11 (95% CI, 0.02–0.48).55
In a crossover study performed in Germany, Schertling et al57 studied 23 adult participants with a diagnosis of infection‑related asthma. The 5‑week study was composed of 2 periods of 2‑week intervention (5 g/day of vitamin C or placebo) and a 1‑week washout between them. Bronchial reactivity using histamine sensitivity testing was carried out in the middle of each 2‑week intervention. In the histamine sensitivity test, 91% of the participants were sensitive to histamine after the week of placebo, whereas 39% were sensitive after the week of vitamin C, with a difference of 52 percentage points (P <0.001).55 A daily asthma symptom score was evaluated and found to be slightly lower during the vitamin C period.
Bucca et al58 studied the effect of vitamin C on histamine bronchial responsiveness in 9 adult participants, all of whom suffered from the common cold. Bronchial responsiveness was measured at the start of the trial and 6 weeks later, when all participants had recovered from the cold. On both study days, histamine sensitivity was measured before and 1 hour after a single 2‑g dose of vitamin C. The interaction between the vitamin C effect on histamine sensitivity (before / after vitamin C administration) and the presence of the common cold (yes / no) was significant (2‑tailed P = 0.003).55
Lower respiratory tract infections
Two trials found that vitamin C administration significantly reduced the incidence of “chest / throat colds,” while there was no effect on the incidence of “nose colds” (Table 2).23,26,29 In both trials, about two‑thirds of all colds were “nose colds.” Thus, when the 2 types of colds are combined in the analysis, the possible effects on symptoms originating from the lower airways are masked. Kimbarowski and Mokrow59 studied soldiers who were hospitalized for influenza A and showed that vitamin C prevented pneumonia as a complication of influenza59 (see the section on pneumonia).
COVID‑19
The common cold is a condition defined by symptoms. While a wide variety of viruses cause such symptoms, they can also be caused by a few bacteria, such as mycoplasma.1,5 Given the etiological diversity of the common cold, it seems highly unlikely that the effects of vitamin C are limited to a specific virus or virus group. In light of the findings of the common cold trials, it seemed plausible that vitamin C may also have an impact on SARS‑CoV‑2 infection.60
During the COVID‑19 pandemic, there was an urgent need for an evidence‑based response and pressure for researchers to publish hastily. As a result, many journals lowered their quality thresholds.61 This created issues with study quality and much wasted research, including in the vitamin C and COVID‑19 field. Some preliminary studies were overinterpreted and propagated via social media; however, much of the resultant literature is irrelevant. While we have not performed a systematic review of vitamin C for COVID‑19, we provide some brief commentary on the findings of 2 relevant RCTs.
The COVID A to Z trial62 recruited 214 COVID‑19 outpatients. Oral vitamin C at a dose of 8 g/day was administered for 10 days, with the conclusion that “treatment with high‑dose… ascorbic acid… did not significantly decrease the duration of symptoms compared with standard of care.” However, this conclusion was inconsistent with the observations.50,63 Vitamin C actually increased the recovery rate by 70% (Figure 3).
![Change in mortality after abrupt termination of vitamin C administration. Risk ratio [RR] of 1 indicates the level of the control group. This Figure is based on the re-analyses of the LOVIT,, CITRIS-ALI,,, and Two Harmonized Randomized Clinical Trials with COVID-19 patients., In all trials, the vitamin C dose was 50 mg/kg body weight every 6 h for up to 4 days. In the CITRIS-ALI trial, a significant reduction in mortality was observed over the first 4 days, but the groups did not differ thereafter. The other 2 studies found no difference in mortality during the period of vitamin C administration, but after abrupt termination of the vitamin there was a significant increase in mortality for a few days, after which the difference leveled off. In each study, there was a significant difference in the RR before and after the end of the 4-day vitamin C administration period,,, indicating that abrupt termination of vitamin C had a harmful effect on mortality. Adapted from](/paim/_next/image/?url=https%3A%2F%2Fpamw.pl%2Fsites%2Fdefault%2Ffiles%2Fjson_zip_files%2Funcompressed%2F16926%2FIMAGES%2FKP_WEB__FIG_03.png&w=3840&q=75)
Adhikari et al64 undertook another RCT involving nonsevere COVID‑19 patients. The conclusion was that vitamin C did not affect survival or the number of organ support–free days. However, these outcomes are not appropriate for patients with nonsevere disease. The COVID A to Z trial62 measured the duration of symptoms, a more sensitive outcome for nonsevere diseases. Adhikari et al64 administered vitamin C for only 4 days, as compared with 10 days in the COVID A to Z trial. Given the substantial methodological differences, these 2 trials are not comparable.65 However, Adhikari et al64 also studied critically ill COVID‑19 patients (see section on sepsis).
Pneumonia
A century ago, Alfred Hess,66 a pediatrician working in the US, wrote a monograph on scurvy, and emphasized that increased risk of pneumonia was common in scurvy in both humans and guinea pigs66,67 (see extracts in Supplementary material). In 1927, a Polish‑born biochemist Casimir Funk, who coined the term vitamin[e], stated that an epidemic of pneumonia in the Sudan disappeared when antiscorbutic (vitamin C–containing) treatment was given to the numerous people with scurvy, which appeared at about the same time.68 After pure vitamin C became available, several reports claimed it was beneficial for treating pneumonia.69-72
The 2013 Cochrane review6 included 3 controlled trials on vitamin C for preventing pneumonia, and 2 controlled trials on its efficacy for treating pneumonia. We briefly summarize these trials, while longer summaries are available elsewhere.6
The Glazebrook trial37 was carried out in the UK before World War II. The authors wrote that “In a large training school under our observation there were some 1500 youths aged 15–20 years. For the most part they were drawn from the lower wage‑earning classes… The total intake of vitamin C varied from about 10 to 15 mg per student per day… Pure ascorbic acid powder was added to… the morning cocoa, and an evening glass of milk. The mixing was done in bulk in the kitchens before issue. The powder dissolved quickly and easily, and did not alter the appearance or taste of the vehicle.” The vitamin C dose was 0.05–0.3 g/day. “When a youth felt ill he was admitted to Sick Quarters unless his complaint was very mild… The admission to and discharge from the hospital was not under our control.” As to pneumonia: “These cases were subjected to special investigations by us (X‑rays, etc.) to establish certain criteria for the diagnosis.” During the follow‑up period, there were 17 cases of pneumonia in 1100 control participants, and no cases in the 335 vitamin C participants (RR = 0.0; P = 0.006).6
Kimbarowski and Mokrow59 examined soldiers who were hospitalized for influenza A. “The studies were conducted with the use of soldiers almost all of whom were of the same age and received the same diet…” The allocation method was not reported but the trial groups were of similar size, so alternative allocation may have been used. The vitamin C dose was 0.3 g/day. “The diagnosis of influenza was based mainly on the clinical pictures and epidemiological data with serological confirmation in a series of cases involving the type A virus.” During the follow‑up period, there were 10 cases of pneumonia in 112 control participants, and 2 cases in the 114 vitamin C participants (RR = 0.2; P = 0.009).6
Pitt and Costrini25 examined US Marine recruits. “These 862 recruits were assigned randomly to either the vitamin C or placebo group… Pill taking was supervised and observed by the drill instructors in each platoon. Neither the recruits or drill instructors nor the physicians and corpsmen who treated the recruits were aware of which pill any individual was taking… The placebo Tablets were formulated from citric acid and were indistinguishable in appearance and taste from the vitamin C Tablets”. The vitamin C dose was 2 g/day. “Pneumonia developed in eight recruits… Each of these eight recruits had typical roentgenographic and physical signs of pneumonia…” During the follow‑up period, there were 7 cases of pneumonia in the 343 control participants, and 1 case in the 331 vitamin C participants (RR = 0.15; P = 0.02).6
These trials provide strong evidence that vitamin C has an effect on the risk of pneumonia in certain contexts, but they have limitations. All trials included only men; 2 focused on military personnel, and the third on boys in a boarding school. In the Glazebrook trial,37 dietary vitamin C intake was demonstrated to be very low, and in the trial by Kimbarowski and Mokrow,59 it was probably low, whereas in the trial by Pitt and Costrini,25 it was quite high based on plasma levels.6 In the Kimbarowski and Mokrow trial, pneumonia was a complication of influenza, but there is no information on the relationship between respiratory viral infections and pneumonia in the other trials. The Pitt and Costrini study examined individuals under heavy physical stress—a similar context to the trials described in Figure 1.
One further indication of the unusual conditions in the above 3 trials is the high incidence of pneumonia, with more than 30 cases per 1000 person‑years, as compared with 1–3 cases per 1000 person‑years in the general Western population.1,2,6 Evidently, the findings of these 3 trials cannot be extrapolated to the general population.
A cohort study performed in the US found no association between dietary vitamin C intake and pneumonia.73 However, the participants were male health professionals, which means their health literacy was above average and their work was mostly sedentary. In the study cohort, only 10% had a vitamin C intake below 0.095 g/day, as compared with 50% in the general population,40 illustrating the high average intake in the cohort. Finally, the incidence of pneumonia was just 3 per 1000 person‑years.73 Thus, the context for this cohort study is very different from the controlled trials. It seems highly unlikely that vitamin C would further decrease already low rates of pneumonia in the general Western population, but it may have an impact in certain circumstances. This pattern is similar to heterogeneity in vitamin E effects on pneumonia risk.14,15
The Mochalkin therapeutic trial9 was carried out in Russia. “The group of patients comprised 140 men diagnosed with acute pneumonia hospitalized during the first 2 days of onset of the disease.” It was a 3‑arm trial with 1 control and 2 vitamin C arms. The use of a placebo was not mentioned and probably not implemented, but the comparison of the 2 vitamin C arms is informative. Vitamin C was administered for 10 days at doses of 0.25–0.8 g/day in the low‑dose group and 0.5–1.6 g/day in the high‑dose group. In the low‑dose vitamin C group, the mean duration of hospital stay was 19.1 days, as compared with 15.1 days in the high‑dose group, with a reduction by 4 days (95% CI, 2.2–5.8 days).6
The therapeutic trial by Hunt et al10 was carried out in the UK. “The patients enrolled into this… study were suffering from acute bronchitis (often acute exacerbation of chronic bronchitis) or bronchopneumonia… the patients commenced placebo or vitamin C therapy to which they were allocated on a randomized ‘double‑blind’ basis… The vitamin C and placebo Tablets were indistinguishable from each other by look or taste.” The vitamin C dose was 0.2 g/day. In the 27 most severely ill patients, vitamin C decreased the pneumonia severity score (ranging from 3 to 9) by 2.38 units (P = 0.01), whereas it had no effect on the 30 less severely ill patients.1,6 The authors also found a difference in mortality between the 2 groups: there were 5 cases of death in the placebo group, but only 1 death in the vitamin C group (P = 0.059).
In our search for recent trials, we identified 2 relevant RCTs.11,12
In a trial involving 82 pneumonia patients, Mahmoodpoor et al11 administered 4.8 g/day of vitamin C intravenously for 4 days. In the vitamin C group, there was a 55% decrease in the duration of mechanical ventilation (P <0.001). There were 12 and 7 deaths in the placebo and vitamin C groups, respectively, during follow‑up (P = 0.1).
In a trial with 75 pneumonia patients, Chambers et al12 administered 7.5 g/day of vitamin C intravenously, after which 3 g/day were administered orally for a week. In the vitamin C group, there was a 51% decrease in the time from the start of treatment to discharge (P = 0.049). There were 2 and 0 deaths in the placebo and vitamin groups, respectively (P = 0.13).
The Mochalkin trial9 had methodological shortcomings and was not well reported. The methods in the 3 other trials were sound, but the studies were small. Results from all 4 trials strongly suggest that larger trials on the efficacy of vitamin C for treating lower respiratory tract infections should be encouraged to enable definite conclusions to be drawn.
In the interim, given that vitamin C is safe and inexpensive, and that pneumonia patients have reduced vitamin C levels,1,2,6,9-12 it may be reasonable to administer vitamin C to patients with pneumonia while awaiting further research.
Sepsis
There has been a long interest in the relationship between vitamin C and sepsis.74 Pneumonia is a common cause of sepsis, which makes it relevant to this discussion. Sepsis patients have decreased plasma vitamin C levels and the metabolism of infused vitamin C is markedly different in sepsis patients and healthy controls.75 While we have not performed a systematic review of vitamin C for sepsis, there are some comments on a few studies that we consider worth making.
Interest in vitamin C and sepsis exploded in 2017, when Marik et al76 published a before‑after study showing that patients with sepsis who were treated with vitamin C together with thiamine and hydrocortisone had lower mortality than the patients with sepsis treated before the introduction of the intervention. In the 5‑year period from 2012 to 2016, there were 54 PubMed reports on vitamin C and sepsis, whereas in the period from 2019 to 2023, there were 352 such reports.
Although the paper by Marik et al76 generated great interest, it has methodological shortcomings. Differences in a before‑after comparison can arise from changes in other treatments over time or from changes in the types of patients. Moreover, the study was not on vitamin C alone; thiamine and hydrocortisone can have effects of their own, and can interact with vitamin C.77,78 In fact, a cohort study found that vitamin C alone appeared beneficial for sepsis patients, but vitamin C with hydrocortisone did not.79
After the publication of Marik’s paper, several further RCTs investigated administration of thiamine, hydrocortisone, or both together with vitamin C. However, such RCTs are not informative about the effects of vitamin C alone.77,78
The LOVIT trial80 is the largest RCT (n = 872) on vitamin C alone for sepsis. Vitamin C was administered intravenously at a dose of 16 g/day for an 80 kg person for 4 days, after which it was discontinued. There was no difference in mortality between the trial arms during vitamin C administration; however, after discontinuation, mortality increased significantly in the vitamin C arm (Figure 4). Thus, abrupt termination of high‑dose vitamin C may be harmful if the patient is still critically ill.81
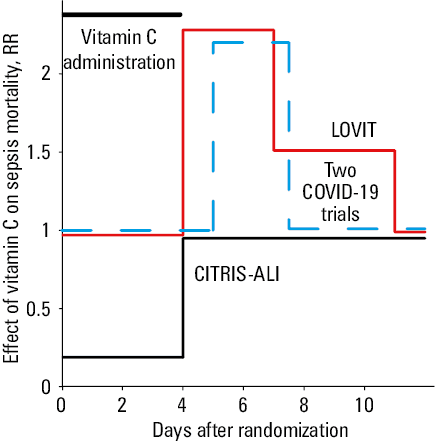
With the same dosage of vitamin C, a similar increase in mortality was seen after the abrupt discontinuation of vitamin C for critically ill COVID‑19 patients (n = 1568) (Figure 4).64,65
In the CITRIS‑ALI trial82,83 (n = 167), the same dosage of vitamin C was administered to patients with sepsis. Mortality decreased during the 4‑day vitamin C administration period, but the benefit ended when the vitamin was discontinued (Figure 4).84 The abstract was misleading, as it did not mention the effect on mortality.50,84
It is likely that the 4‑day vitamin C administration period was too short in these 3 RCTs. A cohort study found that vitamin C was beneficial for sepsis patients when the treatment lasted for at least 5 days, but shorter administration was ineffective.79 Although cohort studies should be interpreted with caution when looking at treatment effects, further trials on vitamin C for sepsis should avoid sudden discontinuation of vitamin C administration if the patient is still critically ill.65,78,81
Finally, vitamin C should not be considered as a potential treatment specific to sepsis; rather, it may be viewed as a support to a wide range of critically ill patients.85,86 Given this, the critically ill COVID‑19 patients are more relevant in the context of critically ill patients, than individuals with nonsevere COVID‑19.
Complex dose comparisons in vitamin C trials complicate interpretation
A significant problem in the interpretation of vitamin C trials arises from the fundamental difference between vitamin C and drugs. In a drug trial, the control group is not given the drug, which simplifies the interpretation of the findings. In contrast, it is impossible to select control participants who have a zero vitamin C intake and no vitamin C in their system. Thus, all vitamin C trials are comparing 2 different vitamin C levels. The lower dose is obtained through diet, and varies considerably among the trials. Furthermore, in some trials, the control group was given extra vitamin C, further confusing the comparisons.
To make the most informative comparison for public health, the control group should ideally receive the recommended vitamin C dose, for example, 0.04 g/day in the UK87 and 0.09 g/day for men in the US.40 However, dietary intake has been much higher in most trials, meaning that they are not a good test of whether the recommended doses are appropriate. The doses of vitamin C supplements given to the vitamin C groups have also varied extensively. Figure 5 shows examples of the variation in vitamin C doses in the control and vitamin C groups.
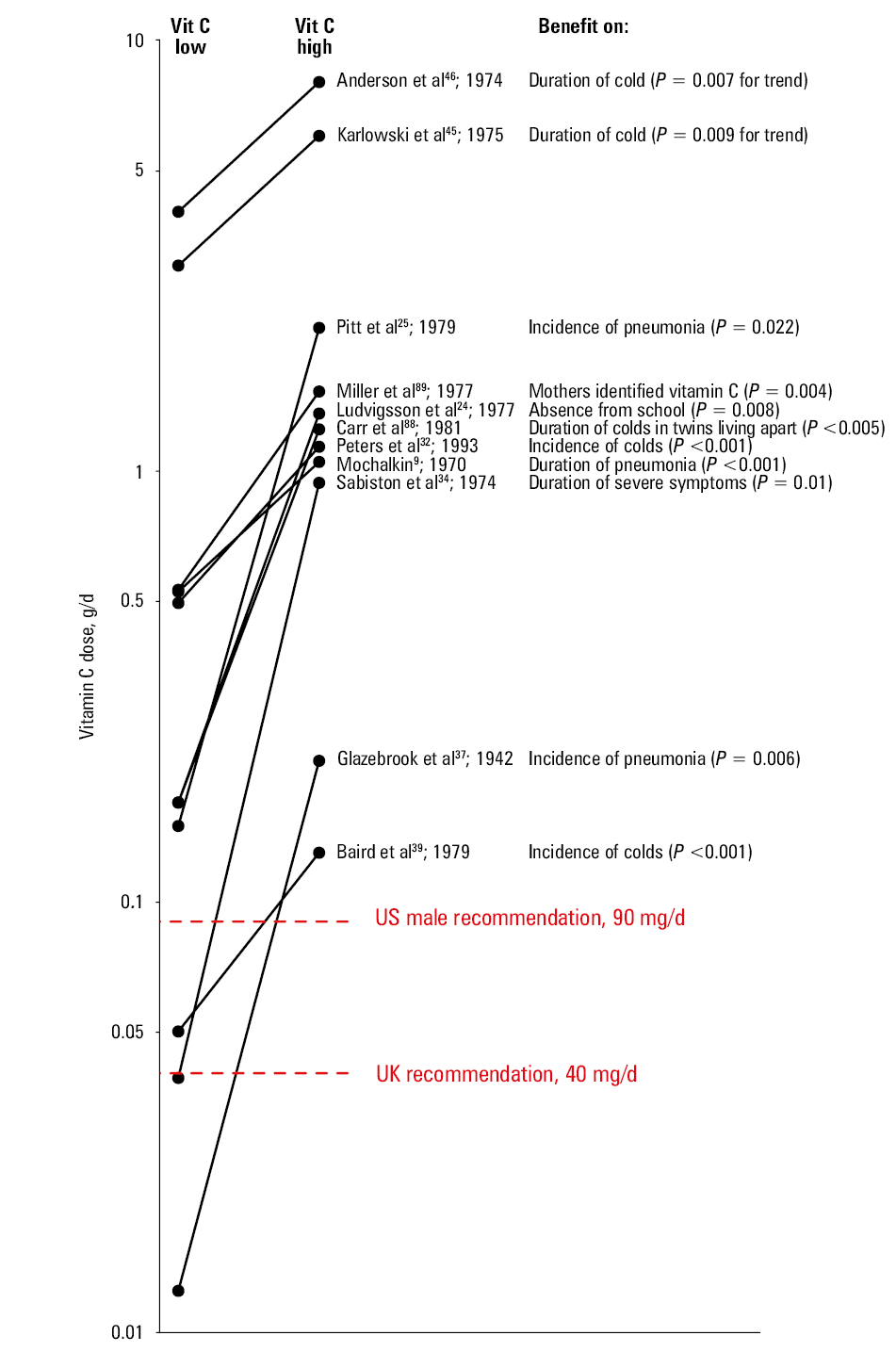
A particularly dramatic illustration is the pair of trials by Baird et al39 and Peters et al.32 Baird and colleagues estimated that the placebo group received 0.05 g/day of dietary vitamin C, with a total dose of 0.13 g/day in the vitamin C group (dietary and supplement together). Peters’ placebo group received 11 times the amount of vitamin C as Baird’s placebo group, and 4 times as much as Baird’s vitamin C group. Peters and colleagues administered 0.6 g/day of vitamin C to the vitamin group, resulting in a total dose of 1.1 g/day. Strangely enough, both trials found significant decreases in common cold incidence in the vitamin C groups. The benefit for men in the Baird trial is explained by the particularly low dietary intake of vitamin C,29,44 whereas the benefit in the Peters trial is explained by the heavy exertion of ultramarathon running.1,5,41 Such trials are incomparable, even though they both “test vitamin C.”
As noted above, the vitamin group in the study by Baird et al39 was administered 0.08 g/day of vitamin C. By comparison, the placebo group in the study by Carr et al88 was administered 0.07 g/day of vitamin C. The doses were similar, but on opposite sides of the comparison.
In the trial by Miller et al,89 at baseline, children excreted more than 0.3 g/day of urinary vitamin C, and the intake must have been even higher. In addition, the placebo group was administered 0.05 mg/day of vitamin C.
Karlowski et al45 compared 3 vs 6 g/day and Anderson46 compared single 4 vs 8 g doses, and in both cases the higher dose had a significantly greater effect on common cold duration (Figure 5).1,2,5,48-50 In these comparisons, the “low‑dose” groups had vitamin C levels 50–100 times the recommended level,40,87 yet there were still additional benefits from the higher dose.
A further problem related to vitamin C dose comparisons is the potential swapping of Tablets.2,16,49 Carr et al88 found a substantial difference in the effect of vitamin C between adolescent twins living together and those living apart, with vitamin C being effective in those living apart.88 This difference seems to be explained by the twins living together having swapped their Tablets. In the trial by Miller et al,89 among schoolboys in the placebo group, urinary vitamin C excretion increased during the study by 0.13 g/day (62%; 2‑tailed P = 0.03), whereas the increase in girls was only 0.027 g/day. Again, Tablet swapping seems a likely explanation for the increase in boys.
Safety of vitamin C
In general, vitamin C is considered safe in doses up to several grams per day. None of the published trials on vitamin C for the common cold reported that it might be harmful in doses that were tested, that is, up to 6–8 g/day.5,23-26,45,46,51 Although there has been speculation about the potential harm of large doses, most of the concerns have been shown to be unfounded.1,40 As to treating the common cold with vitamin C, Bee52 proposed a dose of 10 to 15 g/day for treating colds and Cathcart53 reported that he had orally administered over 30 g/day to common cold patients. Even though such uncontrolled observations do not provide valid evidence of benefit, they indicate the safety of such high doses.
A further example of safety of high‑dose vitamin C is a randomized trial with burn patients who were administered 66 mg/kg per hour intravenously during the first 24‑hours, beginning as soon as possible after admission.90 This corresponds to 126 g/day for a patient with a weight of 80 kg. There was no substantial harm, but rather a significant reduction in the length of mechanical ventilation was observed,86,90 mediated by reduction in resuscitation fluid volume requirements and wound edema. The severity of respiratory dysfunction was also reduced. Intravenous administration of vitamin C leads to much higher plasma levels than oral administration, and so there does not seem to be a cause for concern about oral dosages of 6–8 g/day for treating common cold patients.
There are few reports of severe harm caused by high‑dose vitamin C administration, but they can usually be attributed to other coinciding medical conditions, such as glucose‑6‑phosphate dehydrogenase deficiency or severe kidney diseases.40 For an ordinary person, gastrointestinal disturbances, such as nausea, abdominal cramps, and diarrhea, are the most common adverse effects of high vitamin C intake.40,53 However, these adverse effects resolve when the dose is reduced, and they do not cause any long‑term harm.
Bias against vitamin C and flawed reports
After vitamin C was identified and the pure substance became available, there was much interest in its potential effects on respiratory infections. Many physicians were enthusiastic about the apparent benefits. However, the interest waned over time. This is baffling, since many rather large trials have demonstrated that vitamin C can be effective (Table 2). There are several potential reasons why the interest in vitamin C waned.1,2,50,91
Firstly, many physicians are not familiar with vitamin C biochemistry. It was identified as the cure for scurvy, which is often considered a disease that only involves the connective tissues. However, the biochemistry of vitamin C is complex and not limited to collagen metabolism.2,40,50,91
Secondly, antibiotics were introduced in the mid‑20th century. They are the evidence‑based treatment of choice for patients with serious bacterial infections, and may have overshadowed vitamin C when considering potential treatments for infections more generally. However, antibiotics are not effective against viral infections, and there is evidence that vitamin C is beneficial in some situations, as described above.
Thirdly, 3 prominent papers were published in 1975—2 of them in the Journal of the American Medical Association—which strongly influenced the loss of interest in vitamin C and the common cold in mainstream medicine.1,2,5,50 The 3 papers were later shown to be flawed,1,48,50,91-94 but that did not reverse their lasting impacts. Few RCTs have been initiated since the mid‑1970s.1,2,50
Fourthly, vitamin C is usually associated with complementary and alternative medicines, which may imply that there is a lack of evidence for its efficacy. However, such a classification may more likely be explained by the lack of requirement for a prescription, rather than an absence of evidence from RCTs.50,95
Nevertheless, the effect of vitamin C on respiratory infections has been a popular topic, particularly among lay people, and several analyses of empirical data have been published. Unfortunately, many of them are erroneous, even to the extent that some have been retracted.96-100
Conclusions
The trials discussed in this review strongly indicate that vitamin C has an effect on respiratory infections in certain contexts. There appears to be heterogeneity in the effects in the same way as is observed for vitamin E.14,15 There is no rationale for the general Western population to take vitamin C regularly with the goal of reducing the incidence of cold episodes. However, there is consistent evidence from regular supplementation trials that vitamin C has an effect on common cold severity and duration. Given this, if a person suffers from frequent colds, it is reasonable to test individually whether they may benefit from vitamin C supplementation during the winter. For all common cold patients, it is not unreasonable to test whether 6–8 g/day therapeutic vitamin C appears beneficial, starting soon after the onset of symptoms. Further research is needed; however, the fact that vitamin C is safe and inexpensive makes testing at the individual level practical.
- Hemilä H. Do vitamins C and E affect respiratory infections? PhD thesis. University of Helsinki, Helsinki, Finland; 2006. | Crossref
- Hemilä H. Vitamin C and infections. Nutrients 2017; 9: 339. | Crossref
- Li W, Maeda N, Beck MA. Vitamin C deficiency increases the lung pathology of influenza virus‑infected gulo-/- mice. J Nutr. 2006; 136: 2611‑2616 | Crossref
- Murphy BL, Krushak DH, Maynard JE, et al. Ascorbic acid (vitamin C) and its effects on parainfluenza type 3 virus infection in cotton‑topped marmosets. Lab Anim Sci. 1974; 24: 229‑232. | Crossref
- Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev. 2013; 2013: CD000980. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION