Maturity-onset diabetes of the young type 5 as one of the least common forms of monogenic diabetes

 CC BY 4.0
CC BY 4.0
Maturity-onset diabetes of the young type 5 as one of the least common forms of monogenic diabetes
Maturity‑onset diabetes of the young (MODY) is the most prevalent form of monogenic diabetes inherited in the autosomal dominant manner.1 It primarily affects people aged 10–30 years. Young age and the absence of coexisting obesity often suggest type 1 diabetes, but its mild course (without episodes of ketoacidosis) can lead to misdiagnosis as type 2 diabetes. Depending on the mutation type, 13 subtypes of MODY are distinguished, differing in clinical presentation and prognosis.2 MODY 5 is one of the least common forms of MODY (1%), and it results from a mutation or deletion in the hepatocyte nuclear factor‑1β gene or a spontaneous de novo mutation.3
Aside from diabetes, the typical clinical presentation shows cysts and developmental abnormalities of the kidneys and the reproductive system (uterine or vaginal hypoplasia, bicornuate uterus in women, and hypospadias, cryptorchidism, or vas deferens agenesis in men).4 Other disorders in patients with this mutation include proteinuria, hypoproteinemia, hypomagnesemia, hyperuricemia, and liver dysfunction. Due to its rarity and ambiguous clinical course, it often remains undiagnosed or improperly treated.4
A 31‑year‑old man with a 14‑year history of genetically confirmed MODY 5 (de novo mutation) was admitted to our Department of Internal Medicine, Diabetology and Nephrology due to hyperglycemia. His medical history included renal cysts and hyperuricemia. In the past, he had undergone surgery for bilateral cryptorchidism and has had no offspring. Upon admission, the patient reported weakness, paresthesia, tremors, and hyperesthesia in the toes. His body mass index was 19 kg/m2. Physical examination indicted skin lesions consistent with necrobiosis lipoidica on the shins (Figure 1A).
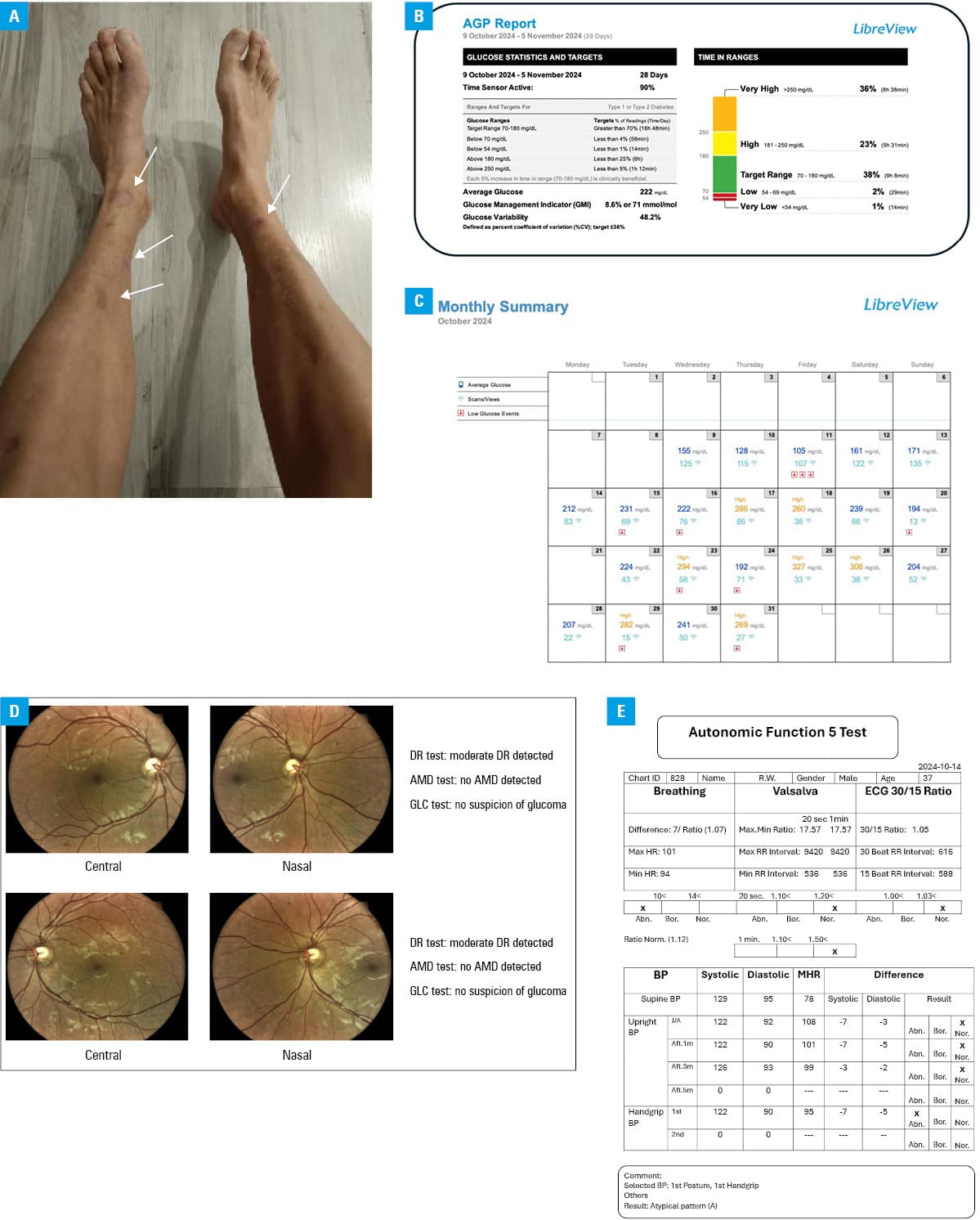
Abbreviations: Abn, abnormal; Aft, after; AMD, age‑related macular degeneration; BP, blood pressure; Bor, borderline; DR, diabetic retinopathy; ECG, electrocardiography; GLC, glaucoma; HR, heart rate; J/A, just after; MHR, mean heart rate; Nor, normal; Norm, norm; RW, patient’s initials
Laboratory tests showed hyperglycemia (366 mg/dl; reference range [RR] <100 mg/dl); glycated hemoglobin level of 14% (RR <6.5%), reduced renal function (creatinine, 1.73 mg/dl; RR: 0.72–1.25 mg/dl; estimated glomerular filtration rate [eGFR], 45 ml/min/1.73 m2; RR >90 ml/min/1.73 m2), hypomagnesemia (1.1 mg/dl; RR, 1.6–2.6 mg/dl), and hypoproteinemia (5.5 g/dl; RR, 6.4–8.3 g/dl). The albumin‑to‑creatinine ratio exceeded 300 mg/g (RR <30 mg/g).
For the past 2 years, the patient was treated with neutral protamine Hagedorn insulin (22 units/day) and metformin (3000 mg/day). The patient’s diabetes was never well controlled, and he was not supervised by a diabetologist.
During hospitalization, metformin was reduced to 1000 mg/day based on the eGFR, and multiple daily injections of insulin were initiated (lispro and glargine, 45 units/day). Glucose monitoring was introduced (FreeStyle Libre‑2, Abbott Laboratories Poland, Warszawa, Poland; Figure 1B and 1C), and the patient received dietary and diabetic re‑education.
Fundus photography showed moderate diabetic retinopathy (Figure 1D). Peripheral diabetic polyneuropathy and autonomic neuropathy were also assessed and confirmed with the Ewing battery (Figure 1E). Pregabalin and α-lipoic acid were prescribed. Magnesium and a protein supplement were reintroduced.
This case report describes one of the least common forms of monogenic diabetes, that is, MODY 5. In this patients, progressive renal dysfunction, which results from congenital abnormalities and chronic poor glycemic control, lack of diabetic education, and long‑term poor treatment of diabetes may lead to the development of end‑stage renal disease.
An early and accurate diagnosis of the type of diabetes allows for better disease management, delaying or preventing complications, and facilitating genetic testing of the patient’s family.
- Gaál Z, Balogh I. Monogenic forms of diabetes mellitus. Exp Suppl. 2019; 111: 385‑416. | Crossref
- Sampathkumar G, Valiyaparambil PP, Kumar H, et al. Low genetic confirmation rate in South Indian subjects with a clinical diagnosis of maturity‑onset diabetes of the young (MODY) who underwent targeted next‑generation sequencing for 13 genes. J Endocrinol Invest. 2022; 45: 607‑615. | Crossref
- Owen K, Hattersley AT. Maturity‑onset diabetes of the young: from clinical description to molecular genetic characterization. Best Pract Res Clin Endocrinol Metab. 2001; 15: 309‑323. | Crossref
- Anık A, Çatlı G, Abacı A, Böber E. Maturity‑onset diabetes of the young (MODY): an update. J Pediatr Endocrinol Metab. 2015; 28: 251‑263. | Crossref
ARTICLE INFORMATION