Can we predict coronary artery disease in patients with heart failure with preserved ejection fraction based on echocardiographic parameters of diastolic dysfunction? A preliminary report

 CC BY 4.0
CC BY 4.0
Can we predict coronary artery disease in patients with heart failure with preserved ejection fraction based on echocardiographic parameters of diastolic dysfunction? A preliminary report
Introduction
Revascularization and medical therapy are safe and effective methods of coronary artery disease (CAD) treatment.1 The conservative approach has recently gained more attention following comparative trials.2 According to recent guidelines,3 a multimodal imaging strategy is strongly recommended to diagnose chronic coronary syndrome (CCS). The anatomical and functional basis of CAD is postulated, along with bimodal therapeutic approaches, including conservative vs interventional treatment.
The limited availability of noninvasive imaging methods (eg, coronary computed tomography angiography) and tests enabling detection of stress‑induced myocardial ischemia (stress echocardiography, cardiac magnetic resonance imaging, single photon emission computed tomography, or positron emission tomography) indicates the need for more accessible tools in clinical practice.4 Computed tomography accurately depicts coronary anatomy, while echocardiography can be easily used due to its cost‑effectiveness and wide accessibility combined with the absence of ionizing radiation.
Stress echocardiography can be regarded as a reliable method for detection of regional myocardial ischemia, though it has some limitations, such as or dobutamine / vasodilator administration and the potential adverse effects.
In epicardial disease, left ventricular (LV) diastolic function impairment typically occurs earlier than systolic dysfunction. Such a scenario was confirmed in animal models, where diastolic dysfunction was followed by the onset of systolic deterioration during ischemic episodes.5 Several echocardiographic parameters have been evaluated in order to develop a more clinically applicable method for diastolic function assessment.6 In the current guidelines, there is no information regarding the association between LV diastolic dysfunction and CAD risk.7
This study aimed to establish the possible relation between diastolic dysfunction confirmed on echocardiography and epicardial atherosclerosis among patients presenting with CCS.
Patients and methods
The study included 81 patients (33 men [41%]) at a median (interquartile range [IQR]) age of 70 (62–75) years. All participants presented with stable angina and heart failure (HF) syndromes, and were admitted to a hypertension and internal medicine department for CCS diagnostics. They reported a history of constricting discomfort or chest pain originating during physical exertion or emotional stress, thus meeting the diagnostic criteria of angina.8 Additionally, all patients presented with HF symptoms, which were classified according to the New York Heart Association (NYHA) classification. Demographic data were recorded, and blood samples were collected for laboratory analysis.
All participants underwent cine angiography and were subsequently divided into subgroups based on the results. Group 1 comprised patients without CAD (non‑CAD group; n = 57). Group 2 included patients with any coronary artery stenosis (any CAD group; n = 24). A subset of patients presenting with significant CAD (≥50% lumen stenosis) was also distinguished from among the patients with any CAD (Group 3; n = 20).
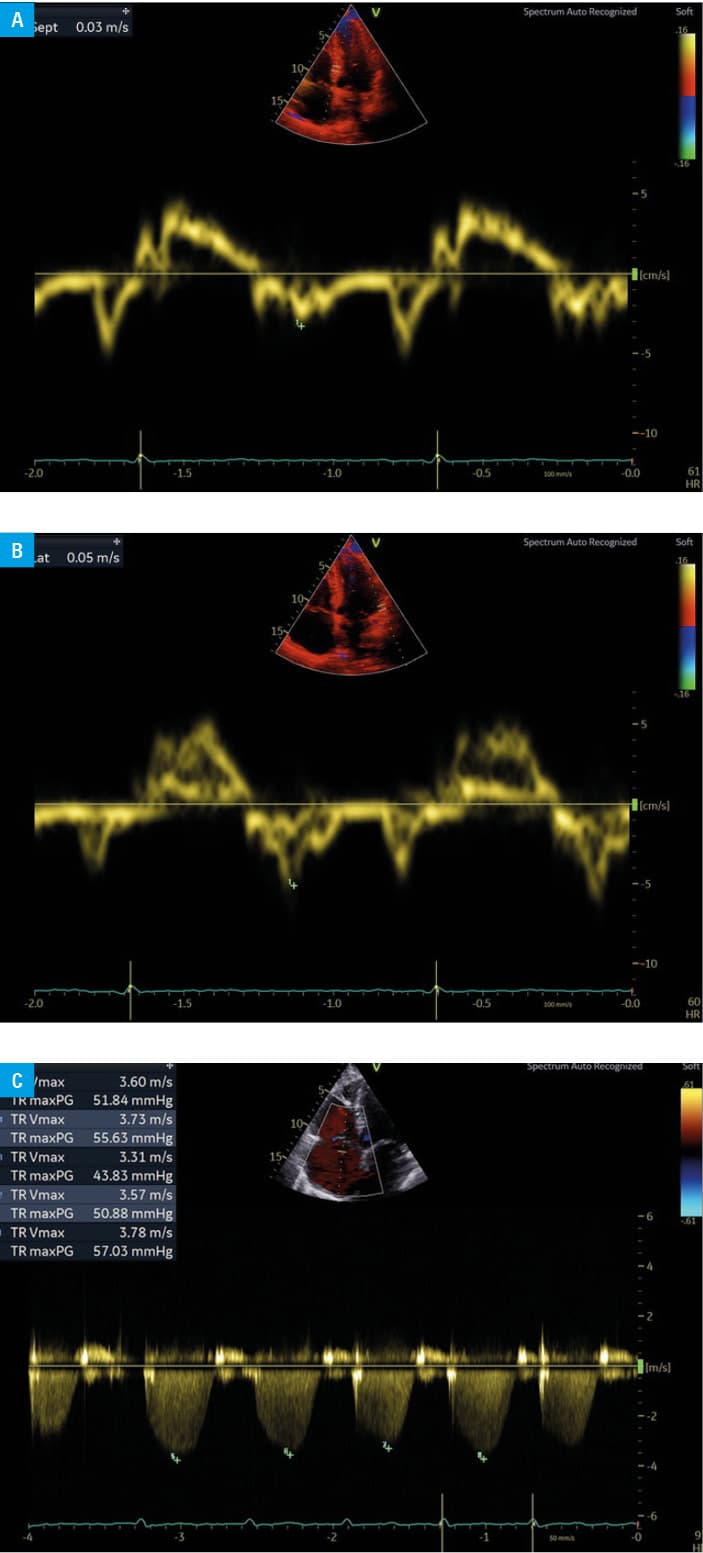
On admission, all patients underwent transthoracic echocardiography. The criteria for diastolic dysfunction were based on to the algorithm proposed by Nagueh et al,9 and comprised septal peak early mitral annular diastolic velocity (e′) below 7 cm/s, ratio of peak early diastolic transmitral flow velocity (E) to e′ greater than 14, and maximum tricuspid regurgitation gradient (TRmax PG) above 31 mm Hg (Figure 1A–1C).
Statistical analysis
Continuous variables were reported as mean (SD) or median and IQR, depending on the distribution. Qualitative variables were presented as sum or percentage. Normality of the distribution of the variables was checked with the Shapiro–Wilk test. The Mann–Whitney test or Fisher exact test was used for intergroup comparisons. Logistic regression was performed to identify the predictors of CAD, including demographic characteristics (sex, age), clinical status (NYHA and Canadian Cardiovascular Society classes), comorbidities (obesity [body mass index >30 kg/m2], arterial hypertension, dyslipidemia, diabetes mellitus, peripheral artery disease [PAD]), laboratory test results (low‑density lipoprotein cholesterol [LDL‑C], high‑density lipoprotein cholesterol [HDL‑C], lipoprotein[a], and creatinine levels), and echocardiographic criteria for HFpEF (septal e′ + E/e′ + TRmax PG). The receiver operator characteristic (ROC) analysis was performed, with the area under the curve (AUC) and F‑measure calculations for predicting CAD in patients with CCS. Statistical analysis was performed using Statistica 13 package (TIBCO, Palo Alto, California, United States). P values below 0.05 were considered significant.
Ethics statement
Informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Poznan University of Medical Sciences, Poznań, Poland (protocol code 694/20 as of November 11, 2020) for studies involving humans.
Results
With respect to clinical status, a majority of the participants were in NYHA class I/II (n = 71 [87%]), followed by NYHA class I (n = 4 [5%]) and NYHA class II or II/III (n = 3 [4%] in each class). The distribution of Canadian Cardiovascular Society classes was as follows: class I, n = 19 (23%); class I/II, n = 51 (63%); class II, n = 11 (14%). The most frequent comorbidities comprised dyslipidemia (n = 76 [94%]), arterial hypertension (n = 73 [90%]), diabetes mellitus (n = 9 [11%]), and PAD (n = 13 [16%]). There were 22 active smokers (27%) in the study population (Supplementary material, Table S1).
Pharmacotherapy was carefully evaluated in all patients on admission. There were no differences between the non‑CAD and any CAD groups regarding the prevalence of treatment with β-blockers (P = 0.99), angiotensin‑converting enzyme inhibitors (P = 0.33), angiotensin receptors blockers (P = 0.97), calcium channel blockers (P = 0.71), sodium‑glucose cotransporter‑2 inhibitors (P = 0.85), loop diuretics (P = 0.57), or aspirin (P = 0.77). The lipid‑lowering agents included statins (P = 0.3) and ezetimibe (P = 0.17) (Supplementary material, Table S2).
Laboratory workup
Peripheral blood samples were collected from all patients, with no significant differences regarding complete blood count analysis, kidney and liver function parameters, or fasting glucose levels. The possible differences in lipid profile were analyzed, showing higher serum total cholesterol concentrations (P = 0.01) in the non‑CAD group. There were no differences regarding HDL‑C (P = 0.42), LDL‑C (P = 0.051), triglycerides (P = 0.31), or lipoprotein(a) (P = 0.35) concentration between the groups, as shown in Supplementary material, Table S3.
Transthoracic echocardiography
All patients underwent a transthoracic echocardiography examination performed by experienced cardiologists, and the results are presented in Supplementary material, Table S4. Combined presence of septal e′ below 7 cm/s, E/e′ ratio above 14, and TRmax PG above 31 mm Hg was found to be different between non‑CAD and any CAD groups (P = 0.01). A difference in these combined echocardiographic parameters was also noted between the patients without CAD and those with significant CAD (P = 0.02).
Multivariable models for coronary artery disease prediction
Model predicting any coronary artery disease
The multivariable model identified male sex (odds ratio [OR], 3.25; 95% CI, 1.1–9.62; P = 0.03), coexistence of PAD (OR, 4.1; 95% CI, 1.05–15.99; P = 0.04), and meeting the echocardiographic criteria for diastolic dysfunction (septal e′ <7 cm/s, E/e′ ratio >14, and TRmax PG >31 mm Hg; OR, 17.8; 95% CI, 1–316.7; P = 0.05) as predictors of any CAD occurrence (Supplementary material, Table S5). The ROC curve for these 3 factors showed an AUC of 0.708 and an F‑measure of 0.333.
Model predicting significant coronary artery disease
The multivariable model identified male sex (OR, 5.03; 95% CI, 1.56–16.26; P = 0.007) and combined echocardiographic parameter (septal e′ <7 cm/s, E/e′ ratio >14 and TRmax PG > 31 mm Hg; OR, 13.28; 95% CI, 1.1–159.79; P = 0.04) as predictors of significant CAD (Supplementary material, Table S6). The ROC curve for these factors showed an AUC of 0.723 and an F‑measure of 0.261.
Discussion
Our analysis points out the possible role of echocardiographic parameters of diastolic dysfunction in CAD prediction among patients with CCS. To our best knowledge, this is the first study revealing the utility of an echocardiographic algorithm describing diastolic dysfunction in CAD identification among patients with stable angina symptoms. We also confirmed male sex as a robust CAD predictor, along with the coexistence of PAD. The algorithm for diagnosing diastolic dysfunction based on 3 echocardiographic parameters is a useful noninvasive tool that can aid in CAD prediction.
The study confirmed the presence of sex‑related differences in CAD epidemiology. The increased prevalence of cardiac disorders among men has been confirmed regardless of the race. On the contrary, women are characterized by greater prevalence of nonobstructive epicardial disease. The sex‑specific aspects are considered in the pathophysiology of both macro- and microvascular dysfunction.10 Men account for up to 75% of the population of patients with CAD.11 On the other hand, there is a growing recognition of sex‑specific determinants of inferior outcomes in women.12
Previous analysis found that atherosclerotic involvement of various vascular beds in the same patient can be regarded as a potential negative prognostic factor for future CAD events. Those patients benefited the most from combined antiplatelet and oral anticoagulant therapy.13
Another CAD predictor identified in the study was a combination of echocardiographic parameters indicating diastolic dysfunction, that is, septal e′, E/e′ ratio, and TRmax PG. While systolic dysfunction has been commonly related to CAD, noninvasive assessment of patients with preserved ejection fraction remains challenging. LV diastolic dysfunction may accompany significant epicardial disease even in the absence of contractility disturbances. The diastolic function abnormalities may precede systolic dysfunction and, therefore, can be regarded as an early and sensitive marker of ischemia. Elevated LV filling pressure and increased mean wedge pressure are characteristic features of diastolic dysfunction. In a population of patients with similar clinical characteristics, echocardiographic parameters, primarily the algorithm including septal e′, E/e′ ratio, and TRmax PG, revealed disorders in coronary perfusion pressures, predicting both CAD occurrence and significance. Coronary plaque burden has been significantly associated with diastolic remodeling,14 and the extent of CAD has been related to worsening diastolic function. In our study, single diastolic parameters were recorded in individual patients; however, a combination 3 measurements related to potential myocardial ischemia was found relevant for CAD prediction.
In clinical practice, the E/e′ ratio is considered the most reproducible method for LV filling pressure estimation. Based on our analysis, it could be regarded as a potential CAD predictor. Transmitral flow velocity ratio reflects changes in the LV long‑axis dimension and volume, and may indicate myocardial relaxation. It is the most often used parameter for the assessment of LV filling pressures, which, in turn, are elevated in myocardial ischemia. Thus, this diastolic measurement may reflect myocardial impairment in CAD.
Previous studies also indicated the clinical utility of the E/e′ ratio in diagnosing CAD in patients with HFpEF.15
TRmax PG, aside from being recommended as the main parameter for estimating pulmonary artery pressure, can also aid in predicting CAD in patients presenting with HFpEF and diastolic dysfunction. CAD may impair early LV relaxation and increase left atrial pressure, thus leading to elevated pulmonary pressure, detected by TRmax PG increase.
Limitations
This was a single‑center study with a limited number of patients presenting with CCS. Our results point out the potential utility of one of the echocardiographic algorithms for diastolic dysfunction diagnosis for CAD prediction. Further studies are required to confirm possible correlations.
Conclusions
The echocardiographic criteria for diastolic dysfunction based on decreased septal e′ and E/e′ ratio values combined with increased TRmax PG may indicate an increased risk for CAD occurrence in the male HFpEF population.
- Parma Z, Young R, Roleder T, et al. Management strategies and 5‑year outcomes in Polish patients with stable coronary artery disease versus other European countries: data from the CLARIFY registry. Pol Arch Intern Med. 2019; 129: 327‑334. | Crossref
- Rakisheva A, Marwan M, Achenbach S. The ISCHEMIA trial: implications for non‑invasive imaging. Anatol J Cardiol. 2020; 24: 2‑6. | Crossref
- Vrints C, Andreotti F, Koskinas KC, et al; ESC Scientific Document Group. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024; 45: 3415‑3537.
- Bergamaschi L, Pavon AG, Angeli F, et al. The role of non‑invasive multimodality imaging in chronic coronary syndrome: anatomical and functional pathways. Diagnostics (Basel). 2023; 13: 2083‑2102. | Crossref
- Hoffmann R, Hanrath P. From systole to diastole: will the detection of regional diastolic dysfunction allow recognition of coronary artery disease at an earlier stage? Eur Heart J. 1999; 20: 476‑477.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION