Life-threatening postpneumonectomy syndrome with vascular distortion successfully treated with extracorporeal membrane oxygenation and tissue expander placement in a woman with lung cancer

 CC BY 4.0
CC BY 4.0
Life-threatening postpneumonectomy syndrome with vascular distortion successfully treated with extracorporeal membrane oxygenation and tissue expander placement in a woman with lung cancer
Postpneumonectomy syndrome (PPS) is a rare complication characterized by hyperinflation of the other lung, mediastinal shift, and tracheobronchial stenosis.1-3 We present a rare case of life‑threatening left‑sided PPS with distortion of pulmonary veins, successfully managed with multidisciplinary treatment.
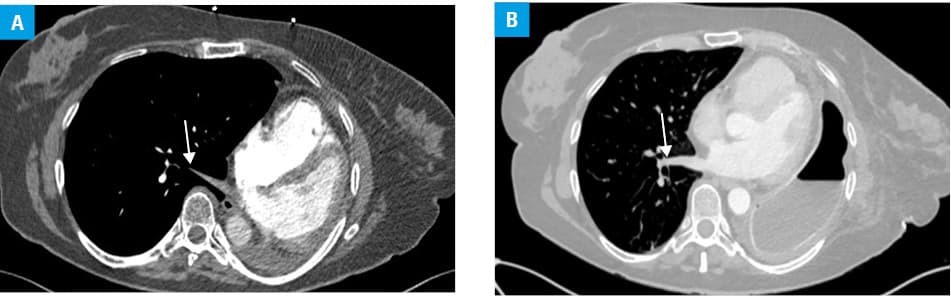
A 55‑year‑old woman, a current smoker with mild chronic obstructive pulmonary disease, underwent left intrapericardial pneumonectomy for T3N1 squamous cell lung cancer in February 2023. The patient started adjuvant chemotherapy, which was poorly tolerated and discontinued after the first course. In August 2023, the patient developed rapidly increasing dyspnea and respiratory failure. Chest computed tomography (CT) showed significant mediastinal shift to the left, major hyperinflation of the right lung, and significant torsion and compression of the right inferior pulmonary vein (Figure 1A). Echocardiography showed impaired diastolic left ventricular (LV) inflow. The A/E ratio of peak velocity blood flow (PVBF) from LV in early diastole (A) to PVBF in late diastole (E) caused by atrial contraction was 0.38 m/s to 0.48 m/s, suggesting diastolic dysfunction and slightly elevated LV pressure. Anticoagulant and cardiac treatment led to moderate improvement, but after 10 days the patient developed severe hypoxemic respiratory and circulatory failure. High‑flow oxygen and noninvasive ventilation proved ineffective, respiratory failure worsened, and the patient’s condition became critical. Tracheal intubation was considered futile since the main reason for the respiratory failure was the impaired right inferior pulmonary vein outflow. Following a multidisciplinary team decision, intubation with veno‑venous extracorporeal membrane oxygenation (V‑V ECMO) was performed as bridge management before the planned surgery. The next day, after ventilation stabilized, an 800 ml saline‑filled breast tissue expander was placed via rethoracotomy in the left pleural cavity. This resulted in the mediastinal shift to the right and significant normalization of the right inferior pulmonary vein diameter. The patient was weaned from ventilatory and circulatory support. Over the subsequent weeks, her clinical status improved spectacularly. Thoracic CT showed the mediastinal return to the normal position (Figure 1B). No further treatment was instituted. In December 2024, the tissue expander was replaced due to a small leak. Two years after the primary surgery, the patient remained fully active, with no cancer recurrence or symptoms of respiratory insufficiency.
PPS usually occurs after right pneumonectomy and typically presents as tracheal or bronchial stenosis due to mediastinal shift and torsion. Our patient developed a rare PPS variant with torsion and compression of the remaining pulmonary veins. Standard management of PPS involves implantation of an expander or prosthesis, which may allow for symptomatic relief through anatomical realignment of the mediastinum.4 However, mortality following surgical correction exceeds 6%, with a recurrence rate between 17% and 26%.4 In our case, intracardiac shunting was due to elevated right atrial pressure, disruption of the cardiac geometry, and compression of venous drainage from the opposite lung. Heart displacement caused severe narrowing of the pulmonary veins, which, combined with hyperperfusion of the only lung, resulted in a critical hemodynamic situation. The anatomical realignment of the mediastinum and alleviation of the pulmonary vein compression allowed for spectacular and durable recovery.
The presented case is unique, as it combines 3 rare situations: the occurrence of PPS after left‑sided pneumonectomy, pulmonary vein compression causing critical cardiovascular and respiratory failure, and a successful use of V‑V ECMO bridge therapy, allowing for tissue expander implantation.
- Shen KR, Wain JC, Wright CD, et al. Postpneumonectomy syndrome: surgical management and long‐term results. J Thorac Cardiovasc Surg. 2008; 135: 1210‑1216. | Crossref
- Macaré van Maurik AF, Stubenitsky BM, van Swieten HA, et al. Use of tissue expanders in adult postpneumonectomy syndrome. J Thorac Cardiovasc Surg. 2007; 134: 608‑612. | Crossref
- Birdi I, Bughai M, Wells FC. Surgical correction of postpneumonectomy stridor by saline breast implantation. Ann Thorac Surg. 2001; 71: 1704‑1706. | Crossref
- Christodoulides N, Fitzmaurice GJ, Bukowska I, et al. Post‑pneumonectomy syndrome: a systematic review of the current evidence and treatment options. J Cardiothoracic Surg. 2023; 18: 119. | Crossref
ARTICLE INFORMATION