A 73‑year‑old man was admitted to our endocrinology department for hormonal re‑evaluation of left adrenal incidentaloma, which showed a significant increase in size (a year earlier, 32 mm × 18 mm × 13 mm; on current computed tomography, 57 mm × 37 mm × 15 mm with fine calcifications noted for the first time; Figure 1A), but low density and contrast washout percentage typical of adenomas. The patient was asymptomatic. Earlier, his laboratory workup results showed no abnormalities indicative of hormonal activity of the adrenal tumor; however, during the current examination, he demonstrated increased urinary excretion of 3‑methoxytyramine (399 μg/24 h; reference range [RR] <220 μg/24 h) and features of mild autonomous cortisol secretion, evidenced by the overnight dexamethasone suppression test result of 2.6 μg/dl (RR <1.6 μg/dl). Other laboratory results were normal, although high‑normal excretion of metanephrine (267 μg/24 h; RR <297 μg/24 h) and normetanephrine (301 μg/24 h; RR <354 μg/24 h) were also recorded. Adrenocortical scintigraphy with 131I m‑iodobenzylguanidine (131I‑MIBG) demonstrated intense accumulation of the radiopharmaceutical in the tumor’s central part, which could suggest a neoplasm accumulating noradrenaline analogues. Due to a suspicion of pheochromocytoma, the patient was referred for urgent left adrenalectomy after prior pharmacological therapy with doxazosin.
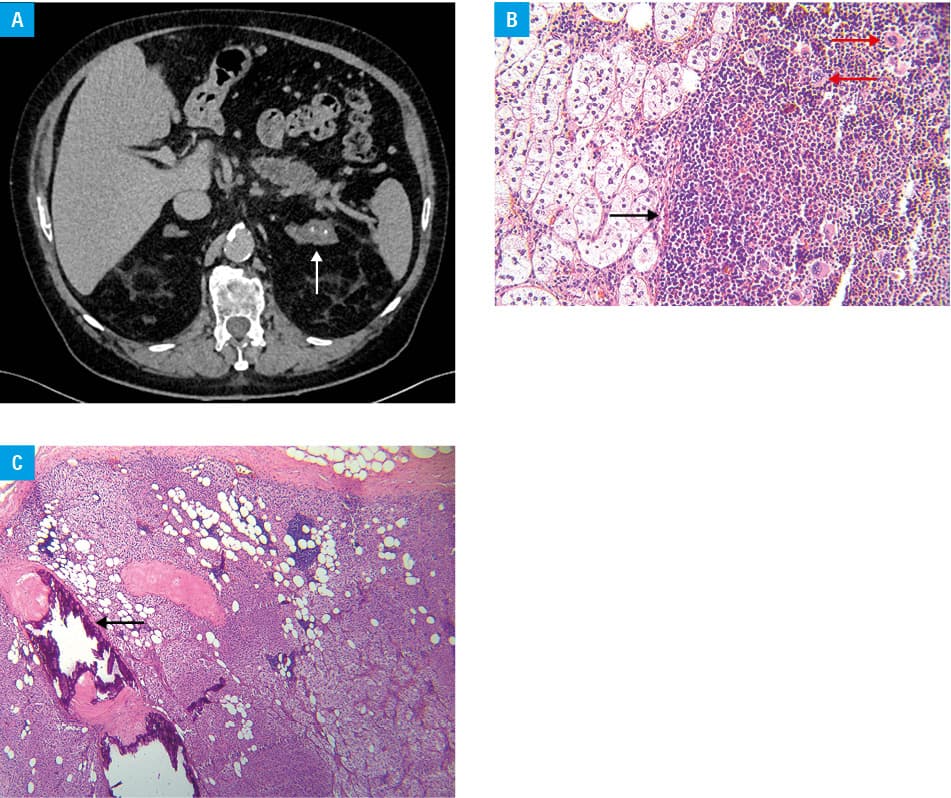
The urology department admitted the patient for left laparoscopic adrenalectomy. The operating urologist noted significant tumor cohesion, pronounced angiogenesis, marked inflammatory lesions, and extremely firm peritumoral tissue with an indistinct dissection plane. A lesion measuring 55 mm × 55 mm × 15 mm, along with a fragment of adipose tissue (19 mm × 8 mm × 5 mm), was sent for examination. Histopathological examination indicated that the tumor consisted of mature adipocytes and extramedullary trilineage hematopoietic cells (with increased number of megakaryocytes; Figure 1B) located in the adrenal gland cortex (findings corresponding with myelolipoma and diffuse adrenal hyperplasia) and exhibited features of osseus metaplasia in about 10% of the total tumor volume (Figure 1C). A diagnosis of pheochromocytoma or other malignant tumors was excluded. As mentioned earlier, no abnormalities (including those of calcium and phosphate metabolism) were observed during endocrine diagnostics; it was also confirmed that the patient did not take excessive calcium or vitamin D. Uncomplicated surgical recovery led to discharge on the third day.
Adrenal myelolipoma (AM) is a rare, benign adrenal gland tumor composed of mature adipocytes and hematopoietic cells. It may be caused by abnormal adrenal cortical adipose tissue expansion due to genetic abnormalities, hormonal imbalance, or aberrant responses to stress or trauma leading to localized adipogenesis.1,2 Most patients with AM do not require surgical intervention, and the prognosis is generally excellent. In our case, rapid growth of the tumor, high‑normal or increased excretion of catecholamine metabolites, and the results of 131I‑MIBG scintigraphy necessitated urgent adrenalectomy following pharmacological preparation, similar to protocols for pheochromocytoma cases.3,4 The reasons for the abnormal scintigraphy result remain unclear; osseus metaplasia is infrequently seen in the adrenal gland, making it challenging to determine any potential correlation.
There is a paucity of research papers addressing osseus metaplasia of the adrenal glands. We wish to underline this unique pathology presentation (to our knowledge, the second in the published literature, excluding malignant lesion case reports2), as its role in the outcome of adrenal incidentaloma is currently unknown.
- Tyritzis SI, Adamakis I, Migdalis V, et al. Giant adrenal myelolipoma, a rare urological issue with increasing incidence: a case report. Cases J. 2009; 2: 8863. | Crossref
- Kumar U, Priyadarshi S, Tomar V, Vohra R. Adrenal myelolipoma with osseous metaplasia and hypercortisolism. Urol Ann. 2017; 9: 71. | Crossref
- Janiak K, Józwik‑Plebanek K, Kamiński G. Recent guidelines for diagnostic and therapeutic management of accidentally detected adrenal tumours (incidentaloma) in adults. Endokrynol Pol. 2024; 75: 385‑394. | Crossref
- Siemińska L, Siemińska K, Marek B, et al. Adrenal tumours and subclinical adrenal hyperfunction. Endokrynol Pol. 2024; 75: 630‑642. | Crossref
ARTICLE INFORMATION