A 38‑year‑old man with no history of chronic diseases was admitted to a hospital with ketoacidosis. He reported typical symptoms of diabetes mellitus (DM), such as polydipsia and polyuria, along with progressive weakness and impaired visual acuity that started about a week ago. Standard treatment for hyperglycemia was implemented, leading to an improvement in the patient’s general condition and normalization of metabolic parameters. The patient was diagnosed with class 3 obesity (body mass index, 52.1 kg/m2) complicated by type 2 DM (glycated hemoglobin, 14.5%; reference range [RR] <5.7%). Diabetes education, accompanied by individual nutrition management, was implemented, and an adequate physical activity plan was outlined. Combined pharmacotherapy with metformin, dapagliflozin, and dulaglutide was started. A therapeutic plan for the treatment of obesity was established, aiming for a reduction of 10% of baseline body weight within 3–6 months (–17 kg). Additionally, a comprehensive metabolic evaluation for complications of obesity was performed, showing atherogenic dyslipidemia, arterial hypertension, metabolic dysfunction–associated steatotic liver disease, hyperuricemia, and obstructive sleep apnea.
Hypercortisolemia was ruled out as a possible secondary cause of obesity. The thyrotropin level was at the lower limit of the RR (0.8 mIU/ml; RR, 0.55–4.78 mIU/ml), and the levels of free thyroid hormones were slightly reduced. Consequently, evaluation of other hormones of the hypothalamic‑pituitary axis was carried out, showing hypogonadotropic hypogonadism (luteinizing hormone, 0.23 mIU/ml; RR, 1.5–9.3 mIU/ml; follicle‑stimulating hormone, 1.21 mIU/ml; RR, 1.4–18.1 mIU/ml; total testosterone, 15 ng/dl; RR, 197–670 ng/dl) and hyperprolactinemia (prolactin, 5088.8 ng/ml; RR, 2.1–17.7 ng/ml). Common causes of hyperprolactinemia, such as drug‑induced, were excluded. The highly elevated prolactin level was indicative of an organic cause of pituitary gland dysfunction, rather than a functional one; therefore, magnetic resonance imaging of the pituitary gland was performed, showing a pituitary tumor with radiological features of macroadenoma, measuring 41 mm × 40 mm × 35 mm (anteroposterior [AP] × craniocaudal [CC] × laterolateral [LR]), with cystic lesions present, compressing the optic chiasm and invading both cavernous sinuses (Figure 1A and 1B). Based on this finding, pituitary macroprolactinoma presenting with hypothyroidism, hypogonadism, and bitemporal impairment of the visual field was diagnosed. Bromocriptine treatment was started, primarily due to its cost‑effectiveness, good tolerance, and early treatment effect, including a significant decrease in prolactin levels and improvement in vision. Additionally, levothyroxine substitution was initiated.
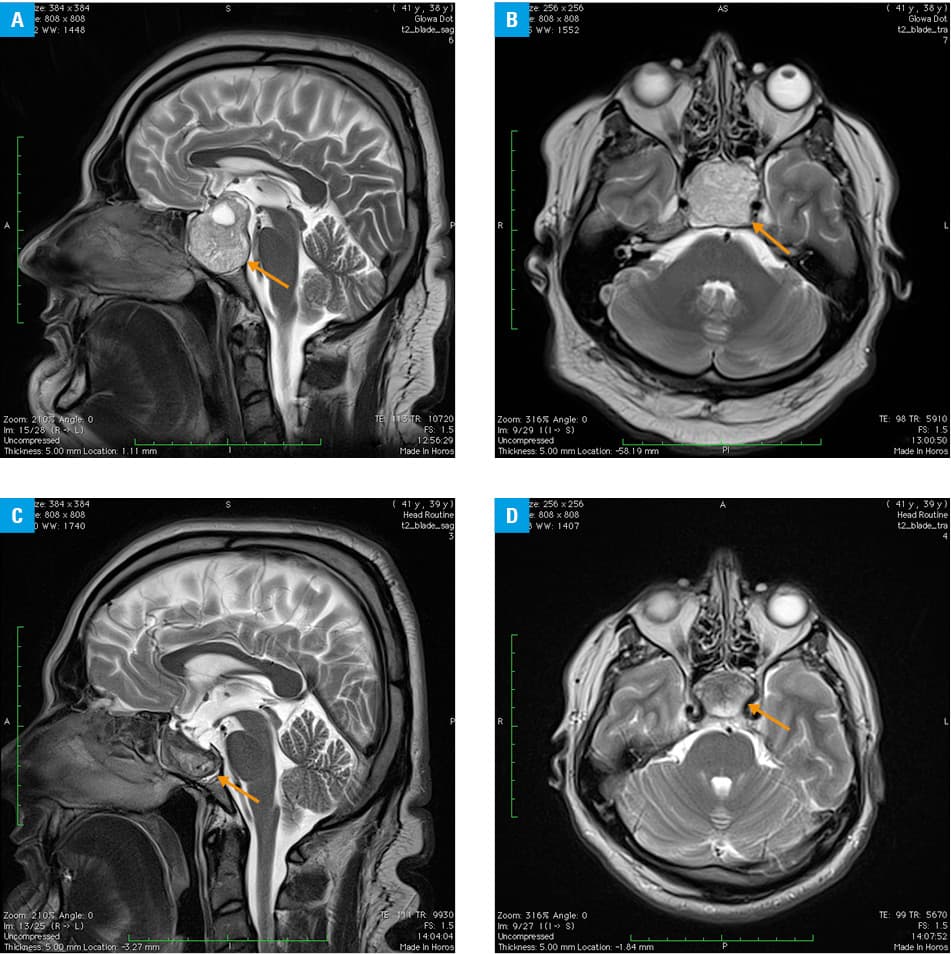
After a 3‑month follow‑up, the patient achieved the weight reduction goal (–18 kg, including 14 kg of fat mass, and 4 kg of fat‑free mass) and received adequate pharmacotherapy for the treatment of obesity complications and sufficient levothyroxine substitution. Of note, the prolactin level was persistently elevated (464.9 ng/ml) despite bromocriptine therapy at a dose of 30 mg/d. Accordingly, dual dopamine agonist therapy (bromocriptine 30 mg/d + cabergoline 2 mg/week) was implemented, which, after another 3 months, resulted in normalization of prolactin levels and reduction of pituitary tumor dimensions by approximately 40% (33 mm × 18 mm × 38 mm [AP × CC × LR]), along with a significant improvement in vision (Figure 1C and 1D). The treatment was well tolerated; echocardiography showed no signs of heart valve damage. Due to the lack of normalization of testosterone concentration despite achieving normal prolactin levels, testosterone substitution therapy was initiated.
Obesity is a global health pandemic with a steadily increasing prevalence.1 It is associated with numerous negative health consequences.2 This case aimed to highlight the importance of diagnosing complications3 and secondary causes of obesity, such as hypogonadism caused by hyperprolactinemia due to macroprolactinoma.4 Co‑occurrence of obesity with hyperprolactinemia, most often functional, was previously reported in the literature.5 Therefore, it is important not to overlook comorbidities related to excessive body weight and their complications.
- The Lancet Gastroenterology Hepatology. Obesity: another ongoing pandemic. Lancet Gastroenterol Hepatol. 2021; 6: 411. | Crossref
- Płaczkiewicz‑Jankowska E, Czupryniak L, Gajos G, el al. Management of obesity in the times of climate change and COVID‑19: an interdisciplinary expert consensus report. Pol Arch Intern Med. 2022; 132: 16216. | Crossref
- Andolfi C, Fisichella PM. Epidemiology of obesity and associated comorbidities. J Laparoendosc Adv Surg Tech A. 2018; 28: 919‑924. | Crossref
- Ylli D, Sidhu S, Parikh T, et al. Endocrine Changes in Obesity. 2022. In: Feingold KR, Anawalt B, Blackman MR, eds. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. https://www.ncbi.nlm.nih.gov/books/NBK279053/. Accessed November 10, 2024.
- Auriemma RS, De Alcubierre D, Pirchio R, et al. The effects of hyperprolactinemia and its control on metabolic diseases. Expert Rev Endocrinol Metab. 2018; 13: 99‑106. | Crossref
ARTICLE INFORMATION