Atrial septostomy with venoarterial extracorporeal membrane oxygenation in cardiogenic shock: a bridge to heart transplantation

 CC BY 4.0
CC BY 4.0
Atrial septostomy with venoarterial extracorporeal membrane oxygenation in cardiogenic shock: a bridge to heart transplantation
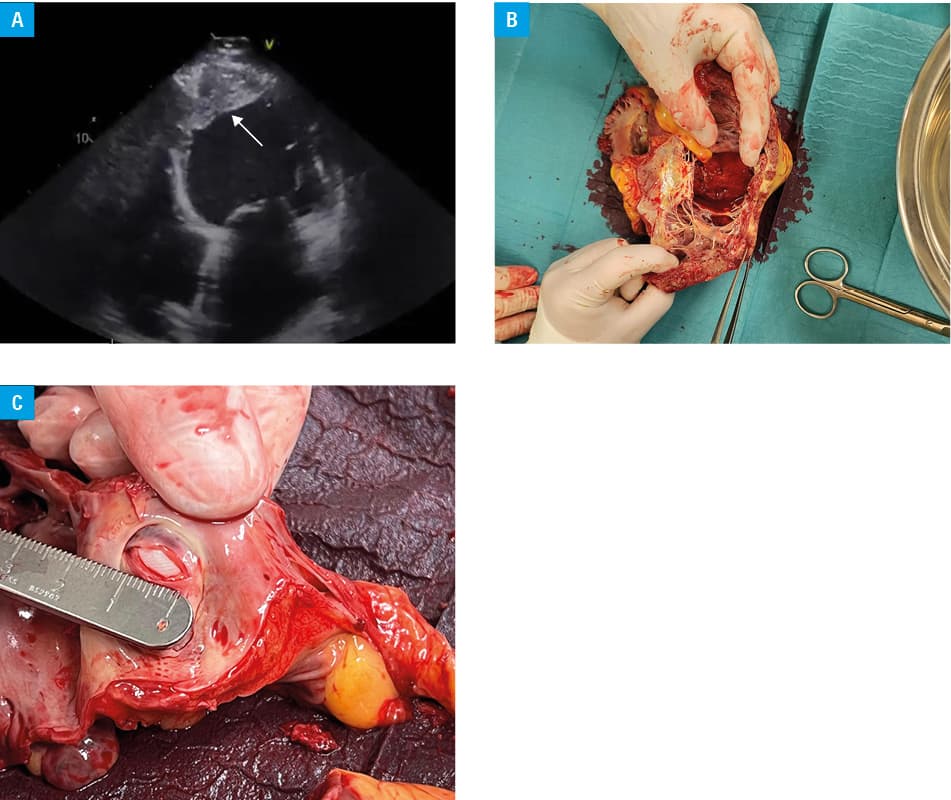
A 64‑year‑old man was admitted to a hospital with cardiogenic shock (CS) secondary to end‑stage heart failure. His medical history was significant for severe mitral regurgitation, prior myocardial infarction, and multiple percutaneous coronary interventions. Physical examination showed peripheral edema, pulmonary congestion, circulatory centralization, and undetectable blood pressure. Laboratory workup showed markedly elevated concentrations of N‑terminal pro‑B–type natriuretic peptide (20 610 pg/ml; reference range [RR] <125 pg/ml); troponin I (90 pg/ml; RR <34 pg/ml), and lactate (11 mmol/l; RR <2 mmol/l). Echocardiography showed severely reduced left ventricular (LV) ejection fraction, severe mitral regurgitation, mild tricuspid regurgitation, and thrombi within the LV. Based on the presence of hypotension and advanced hypoperfusion, the patient was classified as stage C according to the Society for Cardiovascular Angiography and Interventions (SCAI) shock stage classification. Initial management involved the administration of norepinephrine and dobutamine. However, hemodynamic stabilization was not achieved, and the patient was reclassified to stage D on the SCAI scale. The shock team recommended implementation of venoarterial extracorporeal membrane oxygenation (VA‑ECMO). Given the presence of LV thrombi, the patient was deemed suitable for LV unloading through atrial septostomy. In this context, intra‑aortic balloon pumping (IABP) can be considered as a potential method for LV unloading. However, due to the risk of insufficient unloading provided by IABP, atrial septostomy was selected as the preferred approach. Following ECMO cannulation, a 12 mm × 40 mm peripheral balloon catheter was used for atrial septostomy. Over the subsequent days, clinical stabilization was observed. However, 5 days later, the patient developed progressive hypotension with an increasing lactate concentration requiring escalated vasopressor therapy. Ventricular tachycardia developed and was successfully managed with lignocaine and amiodarone. Additionally, bleeding from the vascular access sites necessitated transfusion of 3 units of blood. The shock team proposed implantation of a long‑term LV assist device. However, a day later, due to the availability of a heart donor, the patient was re‑evaluated and prioritized for heart transplant, which was performed 6 days after admission. Unfortunately, he developed several complications, including sepsis, graft failure, and subsequent multiorgan failure, ultimately resulting in death 25 days post‑transplant.
As mortality is high among patients who develop advanced CS while awaiting heart transplants, their management is challenging.1 Mechanical circulatory support can facilitate initial stabilization and serve as a bridge to definitive therapy.2 VA‑ECMO remains a critical rescue therapy for patients with advanced CS3; however, the increased LV afterload associated with VA‑ECMO necessitates strategies for LV unloading to prevent complications. Commonly employed techniques include IABP or microaxial pumps.4 Nonetheless, LV thrombus or aortic valve stenosis may preclude these mechanical approaches. Emerging data from observational studies suggest that percutaneous techniques, including creating a transatrial shunt, offer a viable alternative for LV decompression.5 The presented case was the third instance of atrial septostomy performed in our center. It demonstrated safety and efficacy of the procedure and its potential for facilitating hemodynamic stabilization during VA‑ECMO therapy (Figure 1A–1C). Given the limited frequency of these procedures, they should be performed in high‑volume centers with extensive experience and a highly specialized, well‑trained, multidisciplinary team to minimize the risk of complications.
- Barge‑Caballero E, Almenar‑Bonet L, Gonzalez‑Vilchez F, et al. Clinical outcomes of temporary mechanical circulatory support as a direct bridge to heart transplantation: a nationwide Spanish registry. Eur J Heart Fail. 2018; 20: 178‑186. | Crossref
- Basir MB, Lemor A, Gorgis S, et al. Early utilization of mechanical circulatory support in acute myocardial infarction complicated by cardiogenic shock: the national cardiogenic shock initiative. J Am Heart Assoc. 2023; 12: e031401.
- Rajsic S, Treml B, Jadzic D, et al. Extracorporeal membrane oxygenation for cardiogenic shock: a meta‑analysis of mortality and complications. Ann Intensive Care. 2022; 12: 93. | Crossref
- Gandhi KD, Moras EC, Niroula S, et al. Left ventricular unloading with impella versus IABP in patients with VA‑ECMO: a systematic review and meta‑analysis. Am J Cardiol. 2023; 208: 53‑59. | Crossref
- Baruteau AE, Barnetche T, Morin L, et al. Percutaneous balloon atrial septostomy on top of venoarterial extracorporeal membrane oxygenation results in safe and effective left heart decompression. Eur Heart J Acute Cardiovasc Care. 2018; 7: 70‑79. | Crossref
ARTICLE INFORMATION