Immune thrombocytopenic purpura in a patient with left atrial thrombus and a history of mitral valve replacement

 CC BY 4.0
CC BY 4.0
Immune thrombocytopenic purpura in a patient with left atrial thrombus and a history of mitral valve replacement
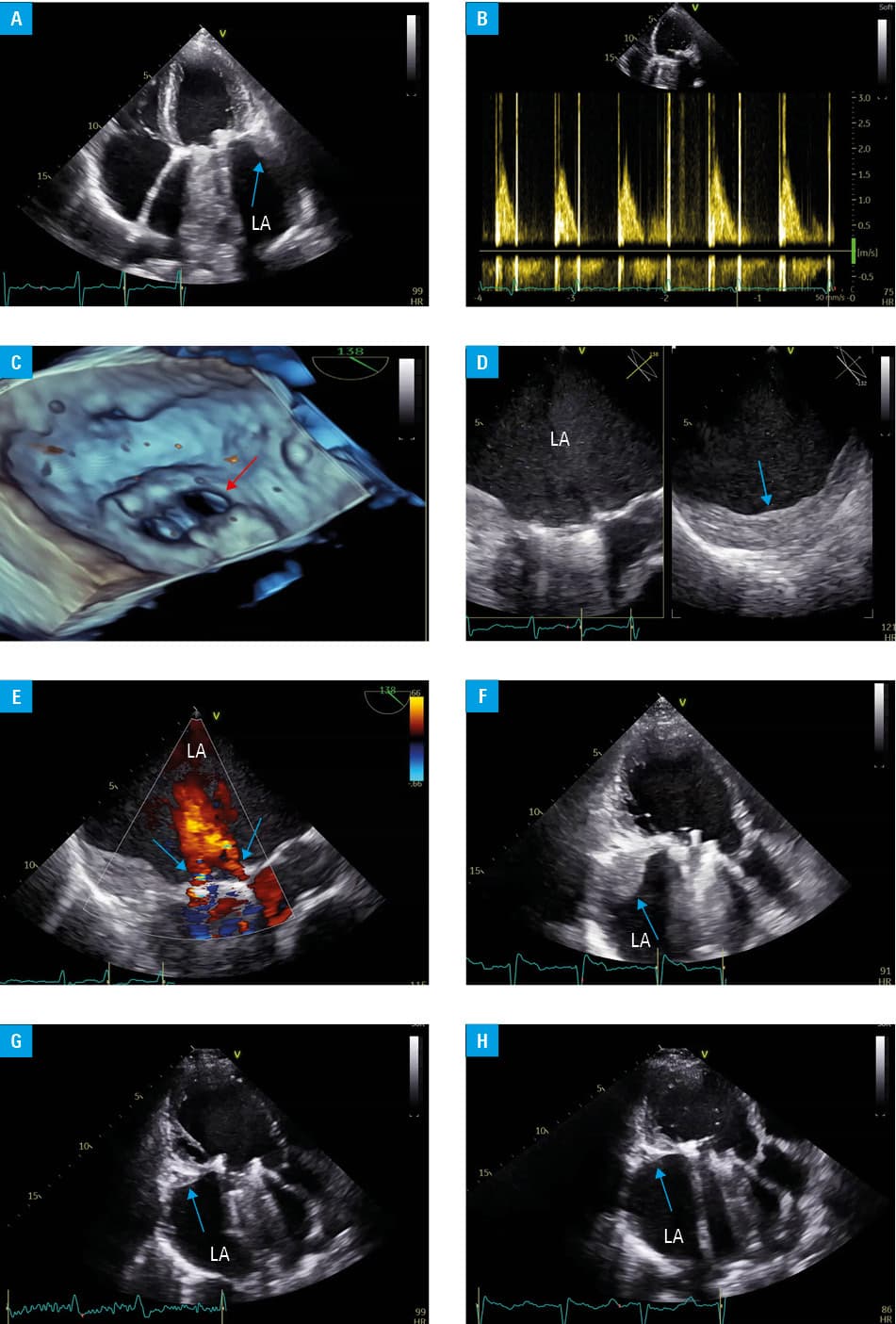
Idiopathic thrombocytopenic purpura (ITP) is an autoimmune disorder characterized by isolated thrombocytopenia (platelet count <100 000/µl) of unknown cause, associated with increased morbidity, mortality, and a high prevalence of complications and adverse effect of treatment.1,2 We present a case of a 40‑year‑old woman who previously underwent implantation of a double‑disc mechanical mitral valve Medeng‑2. She also had a history of rheumatic fever in childhood and persistent atrial fibrillation. The patient’s medical records indicated transient decreases in platelet counts (ranging from 10 000 to 20 000/µl), followed by their spontaneous increases, first reported in 2016. She was diagnosed with ITP in 2020 in Poland. The patient presented to our outpatient clinic because of a significant mitral valve leak suspected on transthoracic echocardiography (TTE), with minimal symptoms (New York Heart Association class I). She did not receive any anticoagulant treatment due to critically low platelet counts (1000/µl). TTE showed significant enlargement of the left atrium (LA; LA volume index of 264 ml/m2) with a large mural thrombus on the posterolateral wall of the LA (Figure 1A). Additionally, global left ventricular hypokinesis with reduced ejection fraction of 40% and normal mechanical mitral valve parameters (mean pressure gradient, 5 mm Hg) were confirmed (Figure 1B and 1C). Moderate‑to‑severe tricuspid regurgitation was also diagnosed, with pulmonary artery systolic pressure estimated at 40 mm Hg. Transesophageal echocardiography was performed, confirming the presence of a large thrombus in the LA and 2 mild‑to‑moderate regurgitant jets; however, the jets were classified as constructive (Figure 1D and 1E). Full guideline‑recommended treatment for heart failure was gradually introduced. ITP was initially treated with corticosteroids and immunoglobulins, but the desired effect was not achieved. Second‑line therapy with eltrombopag, a thrombopoietin receptor agonist, was started; unfortunately, it did not yield the anticipated efficacy either.1 Immunosuppressive therapy with mycophenolate mofetil was discontinued after 3 months due to its ineffectiveness. On frequent follow‑up TTE studies, transvalvular gradients remained stable; however, progressive enlargement of the thrombus was observed (Figure 1F), necessitating intensification of ITP treatment to allow the initiation of anticoagulant therapy. Since June 2021, the patient has been treated with romiplostim (a thrombopoietin receptor agonist that stimulates megakaryocyte precursors), initially under a donation agreement with the manufacturer, and later through the Emergency Access to Drug Technologies program.3 This resulted in platelet count increase, allowing for the initiation of low‑molecular‑weight heparin therapy. Subsequent laboratory tests confirmed stable platelet counts above 50 000/µl, enabling reintroduction of warfarin. Further TTE examinations demonstrated a gradual reduction in the thrombus size (Figure 1G and 1H). The patient did not experience any thromboembolic events during the observation period. The platelet count has remained stable for 2 years, allowing for continued anticoagulation.
Hematologic disorders, particularly those involving platelets, such as ITP, pose a considerable challenge in the management of patients requiring anticoagulant therapy. The primary clinical manifestation of ITP is bleeding, though it could also be associated with thrombosis. In a study by Sarpatwari et al,4 the incidence of thromboembolic events in patients with ITP was 1.3‑fold higher than in matched controls over a 4‑year follow‑up.
- Taylor A, Westwood JP, Laskou F, et al. Thrombopoetin receptor agonist therapy in thrombocytopenia: ITP and beyond. Br J Haematol. 2017; 177: 475‑480. | Crossref
- Soetisna TW, Parna DR, Damayanti NMAS, et al. Initial thrombocyte concentrate transfusion in woman with chronic immune thrombocytopenia purpura (ITP) who underwent mitral valve replacement surgery: a case report. Am J Case Rep. 2023; 24: e938752. | Crossref
- Bussel JB, Soff G, Balduzzi A, et al. A review of romiplostim mechanism of action and clinical applicability. Drug Des Devel Ther. 2021; 15: 2243‑2268. | Crossref
- Sarpatwari A, Bennett D, Logie JW, et al. Thromboembolic events among adult patients with primary immune thrombocytopenia in the United Kingdom General Practice Research Database. Haematologica. 2010; 95: 1167‑1175. | Crossref
ARTICLE INFORMATION