Medium-bore Lightning Flash catheter aspiration thrombectomy in acute pulmonary embolism: first experience in Poland

 CC BY 4.0
CC BY 4.0
Medium-bore Lightning Flash catheter aspiration thrombectomy in acute pulmonary embolism: first experience in Poland
This report describes a case of a 47‑year‑old man with obesity and hypertension who experienced an intermediate‑high‑risk (IHR) pulmonary embolism (PE) following prolonged immobilization due to long‑distance travel and gastroenteritis‑related dehydration. He was transferred from a remote hospital and had suffered from progressive dyspnea over the past 2 days despite receiving anticoagulation with a therapeutic dose of low‑molecular‑weight heparin. Upon arrival, he exhibited tachycardia at 105 bpm and hypoxia, with a respiratory rate of 26 bpm, necessitating 5 l/min of supplemental oxygen via nasal cannula to maintain oxygen saturation (SaO2) of 96%. He was normotensive (146/100 mm Hg), but had elevated troponin I levels (251 ng/l; reference range <34.2 ng/l). Echocardiography showed a severely enlarged right ventricle (RV) with reduced function and a right ventricular / left ventricular (RV/LV) diameter ratio of 2. Computed tomography pulmonary angiography confirmed severe RV dysfunction with an RV/LV ratio of 2.16 (69 mm/32 mm; Figure 1A), a saddle thrombus, and bilateral occluding clots in the proximal pulmonary arteries (PAs; Figure 1B). Given the persistent RV failure and high proximal clot burden, the local PE response ream qualified the patient for catheter‑directed mechanical thrombectomy (CDMT) with the novel Lightning Flash system (Penumbra, Alamdea, California, United States), which was used in Poland for the first time.
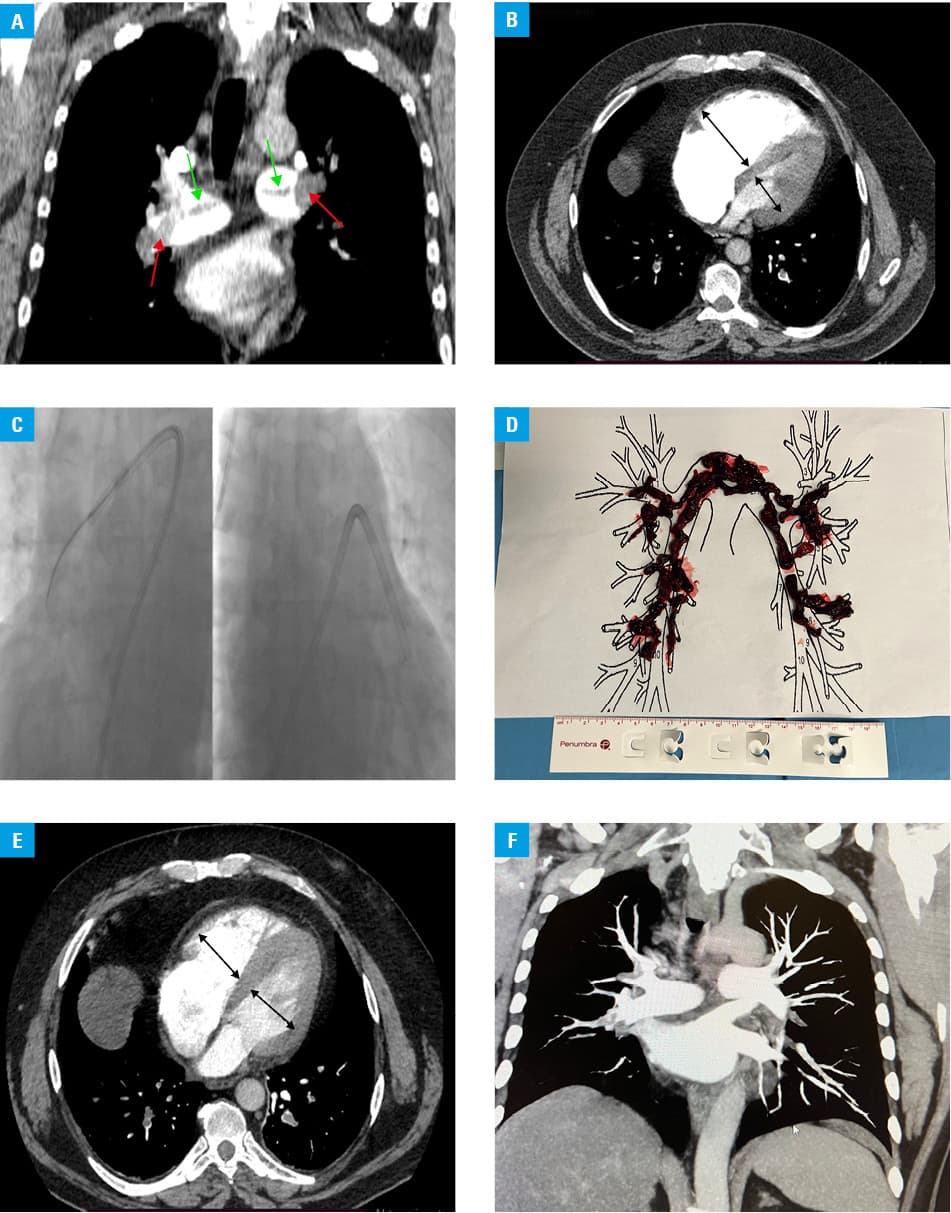
Under ultrasound guidance, the right femoral vein was accessed, and an 18‑F 30‑cm Cook sheath (Cook Medical, Bloomington, Indiana, United States) was introduced. After angiographic confirmation of the central location of thrombi, a 16‑F 100‑cm Lightning Flash HTORQ catheter was inserted into the right PA. The system was navigated using a 6‑F Select Access Catheter with a Bernstein tip design and a 0.035‑inch Amplatz guidewire (Boston Scientific, Marlborough, Massachusetts,United States; Figure 1C). The aspiration started with the catheter placed at the edge of the proximal thrombus. The Lightning Flash catheter was then torqued to capture thrombi in the right and left PAs and their lobar branches, effectively removing the clots from both sides (Figure 1D).
The procedure was uncomplicated and resulted in substantial bilateral clot clearance. It also led to a decrease in mean PA pressure from 30 mm Hg to 22 mm Hg and an improvement in cardiac index from the baseline 1.7 l/min/m² to 2.1 l/min/m². The device’s in / out time was 10 minutes, which is shorter than the median procedural time of 30 minutes for other thrombectomy devices used in our center.1-3 The periprocedural blood loss was 350 ml.
Immediately after the procedure, the patient felt instant relief with improved vital signs and normalization of RV function, confirmed by the imaging studies (Figure 1E and 1F). Twenty‑four hours after CDMT, apixaban was initiated, and the patient was discharged home on the fourth day.
After this initial application of the Lightning Flash catheter in Poland, we emphasize its role as a therapeutic option for life‑threatening PE. Compared with other available systems, Lightning Flash allows for a rapid and precise detection and removal of large obstructive thrombi with controlled blood loss.4,5 This case demonstrates how advanced technology enables Lightning Flash to be minimally invasive while remaining highly effective. Thus, it has the potential to remove a greater thrombus volume with less device involvement time.
- Araszkiewicz A, Sławek‑Szmyt S, Jankiewicz S, et al. Lightning 12 ‑ an intelligent computer‑assisted vacuum aspiration thrombectomy system in the treatment of pulmonary embolism: an initial experience. Kardiol Pol. 2024; 82: 543‑546. | Crossref
- Araszkiewicz A, Sławek‑Szmyt S, Puślecki M, et al. Saddle thrombus transcatheter aspiration thrombectomy with novel large‑bore AlphaVac device. Kardiol Pol. 2024; 82:1025‑1026. | Crossref
- Sławek‑Szmyt S, Stępniewski J, Kurzyna M, et al. Catheter‑directed mechanical aspiration thrombectomy in a real‑world pulmonary embolism population: a multicenter registry. Eur Heart J Acute Cardiovasc Care. 2023; 12: 584‑593. | Crossref
- Peclat L, Fonseca JMFE, Barreto FTR, et al. Pulmonary aspiration thrombectomy with Lightning Flash catheter in a young patient with fibrosing mediastinitis. J Vasc Surg Cases Innov Tech. 2024; 11: 101672. | Crossref
- Coutas T, Mannarino M, Ventura M, et al. Technical aspects of Penumbra Indigo Lightning Flash System for mechanical thrombectomy of pulmonary embolism: a comprehensive review. J Endovasc Ther. 2024 Jul 26. [Epub ahead of print]. | Crossref
ARTICLE INFORMATION