Oral manifestations of systemic sclerosis: a grave challenge or a great opportunity for early and adequate diagnosis?



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Oral manifestations of systemic sclerosis: a grave challenge or a great opportunity for early and adequate diagnosis?
Systemic sclerosis (SSc) is a chronic, autoimmune, connective tissue disorder that, if left untreated, can be detrimental to the patient’s quality of life.1
SSc is characterized by 3 main pathologies: small vessel vasculopathy, presence of autoantibodies, and dysfunctional fibroblasts that excessively produce extracellular matrix.2-4 The etiology of the disease still remains unknown.3,4 Its oral manifestations are quite common. They can be, however, underreported by patients and underdiagnosed by doctors if overshadowed by graver systemic complications.5,6 Orofacial symptoms may include periodontitis, telangiectasias, mandibular resorption, bone lesions, and xerostomia.4 Due to frequently present microstomia and / or reduced mouth opening, dental hygiene and dental care may be restricted.7
The heterogeneous nature of the disease and lack of a definite single test to confirm or disprove its presence renders correct diagnosis challenging.2 It becomes even more difficult when patients are at an early stage of the disease, where the symptoms might not immediately point toward SSc.2 This can, however, prove to be a unique opportunity for oral health providers to improve the diagnostic process by observing early pathological lesions in the orofacial region brought by the disease.8 We present a case of a patient where suspicion of systemic SSc was raised by a dentist and later confirmed by a rheumatologist.
A 76‑year‑old woman presented to the Department of Periodontology and Clinical Oral Pathology of the University Dental Clinic in Kraków complaining of xerostomia, tenderness, and a chronic burning sensation of the oral mucosa, localized mainly on the tongue.
Medical history of the patient included hypertension, chronic coronary artery disease, and hypercholesterolemia treated with aspirin, metoprolol, ramipril, and rosuvastatin. The patient also suffered from gastroesophageal reflux disease and was treated with omeprazole.
The extra- and intraoral examination showed multiple, small telangiectasias on the skin of the cheeks and nose, deepening of wrinkles around the mouth, and reduced abduction of the lower jaw caused by the tightness and thickening of the skin and mucosa surrounding the lips (Figure 1A and 1B). Both corners of the mouth were affected by angular cheilitis, that is, there were small ulcerations of epidermis present on the overall erythematous skin (Figure 1C).
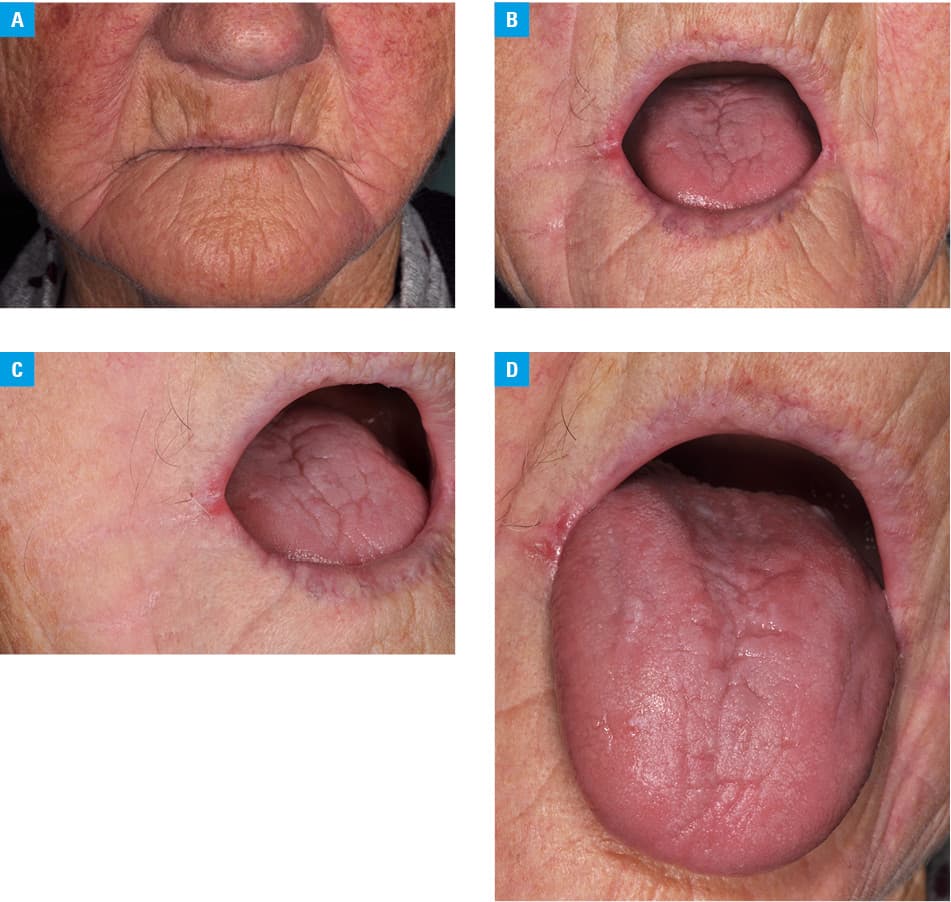
Intraorally, a substantial fibrous thickening of the tissue could be noticed on palpation of the cheeks. On the surface of the cheeks and soft palate, the mucous membrane was pale, with a few, small, red plaques, also classified as telangiectasias.
The tongue was affected by atrophic glossitis—the whole dorsal surface was erythematous, covered by a thin layer of mucosa, with complete absence of filiform and fungiform lingual papillae (Figure 1D).
The patient was referred for further blood tests and a smear test from the oral mucosa. The results showed a slight hyperglycemia (5.7 mmol/l; reference range [RR], 3.9–5.5 mml/l) and increased glycated hemoglobin (6.8%; RR, 4%–6.4%), as well as abnormal liver enzymes (alanine transaminase, 43 U/l; RR, 0–35 U/l; aspartate aminotransferase, 65 U/l; RR, 11–24 U/l). Antinuclear antibodies were strongly positive (1:320). The smear confirmed oral candidiasis with substantial growth of Candida albicans, both on the surface of the tongue and in the corners of the mouth.
The patient was prescribed nystatin in the form of a suspension to use topically 100 000 IU per use, 4 times a day, for 3 weeks, as well as an ointment containing nystatin, hydrocortisone, boric acid, and glycerin to apply on the corners of the mouth. She was also referred to a rheumatologist for further testing to confirm the initial suspicion of SSc and evaluate for possible cardiac involvement and / or interstitial lung diseases. They are the main determinants of patient prognosis; therefore, it is mandatory to investigate heart and lung status in all SSc patients.3
The patient came for a check‑up visit after 6 weeks, noticing a marked improvement in the condition of oral mucosa. Previous symptoms of tenderness and burning of the mucosa resolved completely. Xerostomia, however, persisted. Clinically, there was also significant improvement. There were no ulcerations in the corners of the mouth and the erythema of the dorsal surface of the tongue subsided.
Consultations with a rheumatologist and dermatologist resulted in a confirmed diagnosis of limited SSc with skin, oral, and esophageal involvement. More detailed antinuclear antibody testing confirmed high levels of anticentromere B and antimitochondrial M2 antibodies. Capillaroscopy showed multiple pathological lesions in the microcirculation of the nailbeds and confirmed secondary Raynaud syndrome.
The patient continues to be monitored for new or recurrent oral manifestations of SSc. Due to her overall good management of the disease, no new systemic medication was introduced. The patient reported that her hypertension medication was switched to indapamide and amlodipine after the confirmation of the SSc diagnosis, possibly to better manage the Raynaud syndrome.
- Baron M, Hudson M, Tatibouet S, et al. The Canadian systemic sclerosis oral health study: orofacial manifestations and oral health‑related quality of life in systemic sclerosis compared with the general population. Rheumatology (Oxford). 2014; 53: 1386‑1394. | Crossref
- van den Hoogen F, Khanna D, Fransen J, et al. 2013 Classification criteria for systemic sclerosis: an American College of Rheumatology / European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2013; 72: 1747‑1755. | Crossref
- Lepri G, Di Battista M, Codullo V, et al. Systemic sclerosis: one year in review 2024. Clin Exp Rheumatol. 2024; 42: 1517‑1528. | Crossref
- Antonacci A, Praino E, Abbinante A, et al. Orofacial manifestation of systemic sclerosis: a cross‑sectional study and future prospects of oral capillaroscopy. Diagnostics (Basel). 2024; 14: 437. | Crossref
- Smirani R, Poursac N, Naveau A, et al. Orofacial consequences of systemic sclerosis: a systematic review. J Scleroderma Relat Disord. 2018; 3: 81‑90. | Crossref
ARTICLE INFORMATION