Supervised telemedical monitoring in the heart failure population in the regions of social exclusion is associated with improved functional capacity and quality of life
Key words: e-health solutions, heart failure, quality of life, telemedicine

 CC BY 4.0
CC BY 4.0
Supervised telemedical monitoring in the heart failure population in the regions of social exclusion is associated with improved functional capacity and quality of life
Introduction: Telemedicine is intended to provide medical care to patients in remote areas.
Objectives: This study sought to investigate whether the application of e‑health solutions for patients with heart failure (HF) who live in the regions of social exclusion would improve their functional performance and quality of life (QoL).
Patients and methods: In this prospective, noncontrolled study carried out between June and December 2023, HF patients were enrolled in 14 primary care units located in 5 rural voivodeships in eastern Poland. All patients were evaluated at baseline and after 3 months using the New York Heart Association (NYHA) scale, Chronic Heart Failure Questionnaire (CHFQ), and EuroQol Visual Analog Scale (EQVAS), and monitored by a general practitioner under the supervision of a cardiologist.
Results: In 429 patients with HF, more than 100 000 telemedical examinations / consultations were performed resulting in 575 treatment modifications. During the 3‑month program, 1 patient died. Simultaneously, an improvement in the NYHA scale by a median of 1 class (interquartile range, 0–1; P <0.001) was identified. A 6% improvement in QoL was found in the emotional function measured by the CHFQ (P <0.001), and a 7.7% improvement was observed in subjective health status measured by the EQVAS (P <0.001). A history of atrial fibrillation (odds ratio [OR], 1.539; 95% CI, 1.021–2.353) and no history of cancer (OR, 2.793; 95% CI, 1.224–6.369) were associated with the NYHA class improvement.
Conclusions: The applied telemedical model of care under the specialist supervision was associated with an improvement in the NYHA class and QoL in the HF population from the regions of social exclusion.
Introduction
Despite significant progress in diagnostic and therapeutic methods, heart failure (HF) continues to be a huge challenge in developed societies. Poland, as other Central European countries, is characterized by a relatively high incidence of HF with a prevalence of about 3.2% in the general population and 140 000 deaths per year.1-5 Beyond the clinical aspects and cardiovascular mortality, health services, even in developed countries, must also consider the economic aspect of the HF epidemic, primarily associated with hospitalization costs, which can allocate up to 90% of the total budget for HF treatment.
The application of e‑health solutions and dedicated telemedicine programs has become the current standard for chronic HF patients, resulting in a reduction in mortality and cardiovascular morbidity.6,7 The number of virtual visits, as an alternative to in‑person visits, has increased exponentially during the COVID‑19 pandemic.8 Noninvasive remote monitoring with wearable sensors has become an effective tool for predicting HF exacerbation, and enables accurate estimation of the risk of HF rehospitalization.9 Furthermore, remotely assessed basic parameters, such as body weight, blood pressure (BP), heart rate, selected laboratory parameters, and data from an implantable cardiac device enable successful remote management for two‑thirds of worsening HF patients without hospitalization.10 The available evidence also provides economic arguments for the implementation of easy‑to‑use telemedicine e‑solutions.11-13
Social exclusion is common in the regions with more difficult access to specialist ambulatory care and a lower income per capita, as compared with academic centers and more developed regions. Limited scientific data focused on nonurban areas indicate lower rates of main HF drug use and a worse prognosis in comparison with metropolitan centers. Consequently, rural residence has become a negative factor for the HF population.14
Therefore, we decided to investigate whether the application of telemedicine and e‑health solutions under specialist supervision in the patients with HF who live in the remote regions of social exclusion would improve their performance and quality of life (QoL). This study was carried out as part of the Polish pilot program entitled “Reducing social inequalities in health through the use of telemedicine and e‑health solutions” in cardiology (grant No. 2168 to the Hospital of the Ministry of Internal Affairs and Administration in Rzeszów).
Patients and methods
Study population and design
The study was prospectively designed as an open‑label trial, without any control group, carried out by cardiologists from the College of Medical Sciences at the University of Rzeszow, Poland between June and December 2023. The recruitment was carried out only among outpatients of general practitioners (GPs), and was preceded by a promotional campaign. Finally, 14 primary care units from 5 voivodeships were invited to participate in the project, with particular emphasis on the areas of social exclusion. More than half (52.7%) of the enrolled patients were from the Subcarpathian voivodeship. We defined the area of social exclusion as a region where: 1) average monthly gross remuneration per person was below 80% of the average national gross income per person; 2) total income per person was below 80% of the national income per person; and 3) the minimum distance from a city with a population over 100 000 citizens was at least 50 km. All the criteria were based on data from 2020. The main inclusion criterion was previously diagnosed HF, which was confirmed by a cardiologist on the day of enrollment. Information on the left ventricular ejection fraction was not required to include the patient in the study, unless HF was questionable. There were no formal or clinical exclusion criteria, except for the lack of possibility to continue the telemedicine model for the scheduled 3‑month period.
All included patients were classified according to the New York Heart Association (NYHA) scale at baseline and after 3 months of telemonitoring. QoL was also assessed at the same time points with 2 validated questionnaires, the Chronic Heart Failure Questionnaire (CHFQ)15 and the EuroQol Visual Analog Scale (EQVAS).16 The CHFQ quantifies disease‑specific health‑related QoL (HRQoL). The CHFQ version used in this study comprises 16 items with scales of 1 to 7 to assess the emotional and physical symptoms of HF. The numbers for specific items were summed up to form 3 subscales for dyspnea (5 items), fatigue (4 items), and emotional function (7 items). In both questionnaires, a higher score indicated a higher HRQoL.
The Local Ethics Committee at the University of Rzeszow approved the study protocol (2023/06/0032). All participants gave their informed consent. The study adhered to the STROBE reporting guidelines, and was supported by a grant from the Polish e‑Health Program and Norway resources dedicated to the regions of social exclusion.
Study intervention
After providing the informed consent, every patient eligible for the study was encouraged to undergo regular measurements of their body weight (once a day in the morning directly after using the bathroom),17 heart rate18 and BP (twice a day plus on request)19 within the 3‑month study period, using the same electronic scale (HW‑FIT001, Tech‑Med Technika Medyczna, Warsaw, Poland) and BP monitor model (HW‑HL001, Tech‑Med Technika Medyczna). During the recruitment visit, each patient was equipped with an electronic BP monitor and a scale, integrated with a global system for mobile communications (GSM) transmitter (BT‑HUB v. 4.1, Pro‑PLUS, Warsaw, Poland). Each time BP, heart rate, or body weight was measured, the result was automatically recorded on the data collection platform provided by the Pro‑PLUS company (Warsaw, Poland).
All patients were telemonitored by a selected center (Telemedycyna Polska, Katowice, Poland) open 24 hours a day, 7 days a week.20 In the case of significant abnormalities reported by the electronic devices, including abnormal weight gain of above 4% within 5 consecutive days, high BP of above 160/100 mm Hg or markedly low BP of below 90/60 mm Hg, a telephone intervention was performed. A paramedic, or in special cases a physician, was able to modify pharmacologic treatment for that particular day or propose a permanent change. Due to the study protocol, every patient underwent 3 visits on site (at baseline, at weeks 2–4, and the final visit) with a physician, and a teleconsultation with a cardiologist (at weeks 6–8; Figure 1). There were 2 additional video consultations between the GP and the cardiologist at week 2 and between the weeks 8 and 10. All drugs were prescribed by a physician and, if necessary, by the supervising cardiologist.
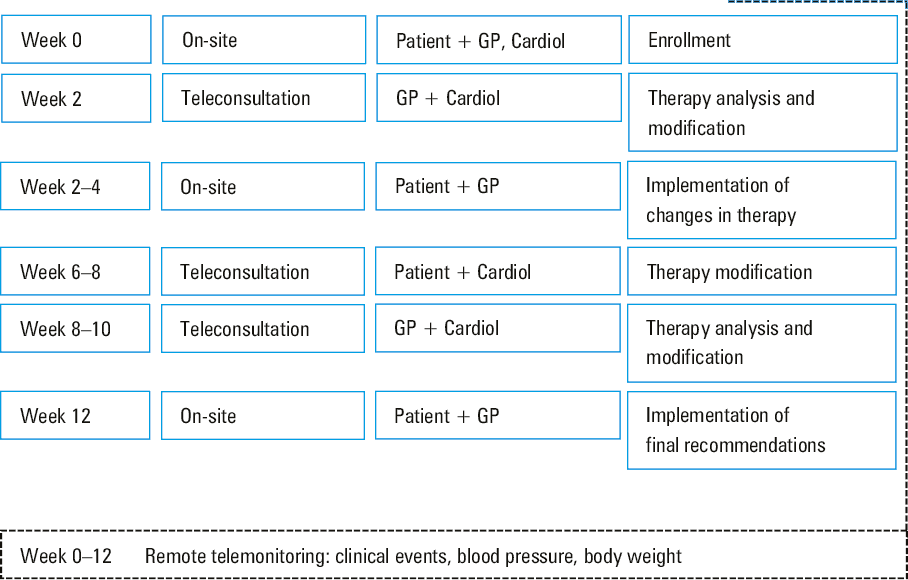
Abbreviations: GP, general practitioner; Cardiol, cardiologist
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics software, version 29.0.2.0 (IBM Corp, Armonk, New York, United States). Continuous variables were expressed as a median (interquartile range [IQR]) or mean (SD), while categorical variables were shown as a number (percentage). The normal distribution was assessed using the Shapiro–Wilk test. A comparative analysis between baseline and 3 months of follow‑up was performed using the paired t test or the Wilcoxon signed rank test for normally or non‑normally distributed variables, respectively. Intergroup differences were evaluated using the t test when normally distributed or the Mann–Whitney test for non‑normally distributed variables. Categorical variables were compared with the χ2 test. Differences between more than 2 groups were compared with the analysis of variance or the Kruskal–Wallis test for normally or non‑normally distributed variables, respectively. The Pearson or Spearman rank correlation coefficients were calculated to test the association between 2 variables having a normal or non‑normal distribution, respectively. All independent variables potentially associated with NYHA class improvement by at least 1 class, expressed as a difference between the 3‑month follow‑up and baseline assessment, were included in the multivariable logistic regression, while independent variables potentially associated with changes in the QoL parameters were included in the multivariable linear regression. A 2‑tailed P value below 0.05 was considered significant.
Results
Between June and September 2023, 1893 patients with a previous diagnosis of HF were invited to participate in this study by their physicians. Of the 1008 individuals who signed up for a recruitment meeting, 429 were confirmed by a cardiologist as patients and enrolled in the study. For 42 patients data were missing due to a lack of sufficient quality of the GSM signal in the patient’s place of residence, gaps in the patient’s questionnaires, or early discontinuation of the study on the patient’s side.
The baseline characteristics of the study group are shown in Table 1. The median (IQR) age of the study group was 72 (66–77) years, and men constituted 61.3%. The most common accompanying cardiovascular risk factors were hypertension, diabetes mellitus, and dyslipidemia. Approximately one‑third of the study group had a medical history of acute myocardial infarction, as well as coronary revascularization. Of the recruited patients, 3.1% were implanted with a cardioverter‑defibrillator.
Parameter | Value |
Data are shown as median (interquartile range) or as number (n/N) and percentage.
a P <0.001
Abbreviations: n/N, number of patients with a given feature / number of patients who had this feature assessed | |
Age, y | 72 (66–77) |
Men | 263 (61.3) |
History of cancer | 30/387 (8.3) |
Chronic obstructive pulmonary disease | 24/387 (6.2) |
Cardiovascular risk factors | |
Hypertension | 323/387 (83.4) |
Diabetes mellitus | 237/387 (61.2) |
Dyslipidemia | 141/387 (36.4) |
Smoking | 43/387 (11.1) |
Chronic kidney disease | 37/387 (9.6) |
Cardiovascular comorbidities | |
Previous myocardial infarction | 118/387 (30.5) |
Previous percutaneous coronary intervention | 92/387 (23.8) |
Previous coronary artery bypass surgery | 31/387 (8) |
History of stroke | 29/387 (7.5) |
History of implantable cardioverter‑defibrillator | 12/387 (3.1) |
Atrial fibrillation | 132/387 (34.1) |
Systolic blood pressure, mm Hg | |
At baseline | 135 (123–148) |
After 3‑month intervention | 131 (121–141) |
Difference between baseline and 3‑month follow‑up | 4 (–6 to 18)a |
Diastolic blood pressure, mm Hg | |
At baseline | 83 (76–93) |
After 3‑month intervention | 80 (74–88) |
Difference between baseline and 3‑month follow‑up | 3 (–5 to 11)a |
Heart rate, bpm | |
At baseline | 69 (62–77) |
After 3‑month intervention | 69 (62–78) |
Difference between baseline and 3‑month follow‑up | 0 (–6 to 6) |
Body weight, kg | |
At baseline | 84.1 (74.1–95.5) |
After 3‑month intervention | 85.5 (74.7–97) |
Difference between baseline and 3‑month follow‑up | 1.3 (–0.4 to 3.1)a |
Within the 3‑month study period, more than 100 000 telemedicine examinations or consultations were conducted, including body weight measurements, heart rate assessments, and daily BP examination. Of them, about 2% met the criteria for the alarm mode. The paramedics, independently or following a consultation with the physician on duty, performed 591 emergency telephone interventions that resulted in 575 pharmacotherapy changes.
Pharmacotherapy interventions
In this group of patients, before any intervention, β-blockers followed by angiotensin‑converting enzyme inhibitors (ACEIs) were the most frequently used medications (Table 2; Supplementary material, Table S1). Almost half of the patients were taking loop diuretics and oral anticoagulants, and one‑third were taking mineralocorticoid receptor antagonists (MRAs) and thiazide diuretics. One‑fourth of the study group used sodium‑glucose cotransporter 2 (SGLT‑2) inhibitors recommended in the guidelines21 for HF therapy.
Parameter | At baseline | After 3‑month program | Net change |
Data are shown as number and percentage.
Abbreviations: SGLT‑2, sodium‑glucose cotransporter 2 | |||
β-Blocker | 370 (86.7) | 390 (91.3) | 20 (4.7) |
Angiotensin‑converting enzyme inhibitor | 273 (63.9) | 297 (69.6) | 24 (5.6) |
Loop diuretic | 204 (47.8) | 207 (48.5) | 3 (0.7) |
Mineralocorticoid receptor antagonist | 158 (37) | 205 (48) | 47 (11) |
Thiazide diuretic | 146 (34.2) | 158 (37) | 12 (2.8) |
Sacubitril / valsartan | 18 (4.2) | 18 (4.2) | 0 |
Angiotensin receptor antagonist | 68 (15.9) | 60 (14.1) | –8 (–1.8) |
SGLT‑2 inhibitor | 107 (25.1) | 153 (35.8) | 36 (8.4) |
P2Y12 inhibitor | 43 (10.1) | 44 (10.3) | 1 (0.2) |
Oral anticoagulant | 170 (39.8) | 173 (40.5) | 3 (0.7) |
During teleconsultations or unscheduled pharmacological interventions resulting from abnormalities in the measured parameters, 575 changes in pharmacotherapy were made (Figure 2). A total of 222 pharmacotherapy modifications took place after the initial teleconsultation between the physician and the cardiologist, 182 during direct teleconsultation between the patient and the cardiologist, and 171 following a second teleconsultation between the physician and the cardiologist. Sometimes more than one drug was changed during a single consultation. Inclusion of a new drug was the most frequent modification of the pharmacotherapy (56.3%), followed by dosage increase (29%). Discontinuation or dose decrease were less frequent (8.3% and 6.3%, respectively).
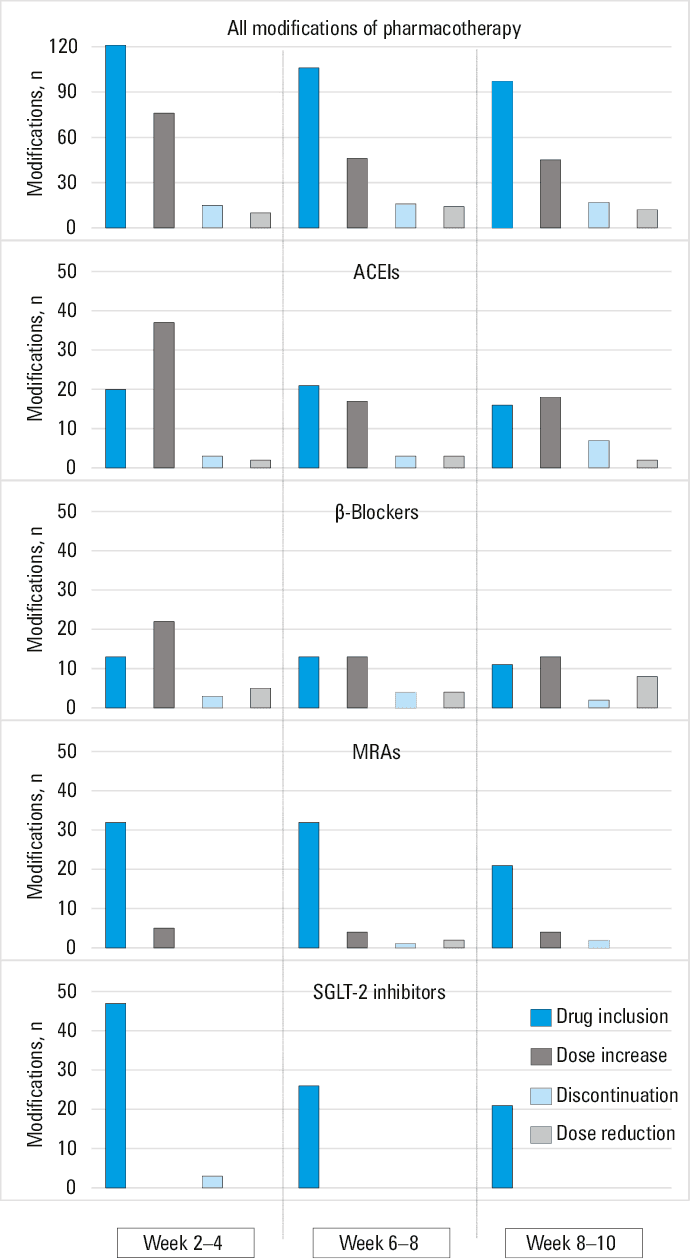
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; MRA, mineralocorticoid receptor antagonist; others, see Table 2
Pharmacotherapy was modified once in 20.3% of the patients, twice in 21%, and 3 or more times in 17.7% of the participants. In the remaining 41%, no modification of the pharmacotherapy occurred. Almost 80% of the modifications concerned 4 types of drugs that make up the main pillars of HF treatment, including ACEIs, β-blockers, MRAs, and SGLT‑2 inhibitors.
The pharmacotherapy interventions in the 3‑month program resulted in a net increase of the use of MRAs by 11%, of SGLT‑2 inhibitors by 8.4%, and of β-blockers by 4.7% (Table 2). However, at the end of the program, only β-blockers were used by more than 90% of the patients, and ACEIs by almost 70%, MRAs by 48%, and SGLT‑2 inhibitors by 35.8%.
Blood pressure and body weight changes
The median (IQR) decrease in systolic BP (SBP) following the program interventions was 4 (–6 to 18) mm Hg (P <0.001), and the decrease in diastolic BP (DBP) was 3 (–5 to 11) mm Hg (P <0.001). Heart rate did not change during the 3‑month program, and body weight decreased by a median (IQR) of 1.3 (–0.4 to 3.1) kg (P <0.001). Body weight loss and the decrease of SBP or DBP were not associated with changes of the NYHA class or QoL.
New York Heart Association class changes
Most of the study population (62.2%) was classified as the NYHA class II at the beginning of the study (Figure 3). In the whole group, an improvement in the NYHA class at the final visit, as compared with the baseline, was identified in 225 patients (52.4%), including an improvement by 2 classes in 66 patients (15.4%), and by 1 class in 159 participants (37%). As many as 202 patients (47.1%) did not experience any change in their NYHA class, and the NYHA class deteriorated in 3 individuals (0.7%; Figure 3). The NYHA class improved between the baseline and 3‑month follow‑up by a median (IQR) of 1 (0–1; P <0.001).
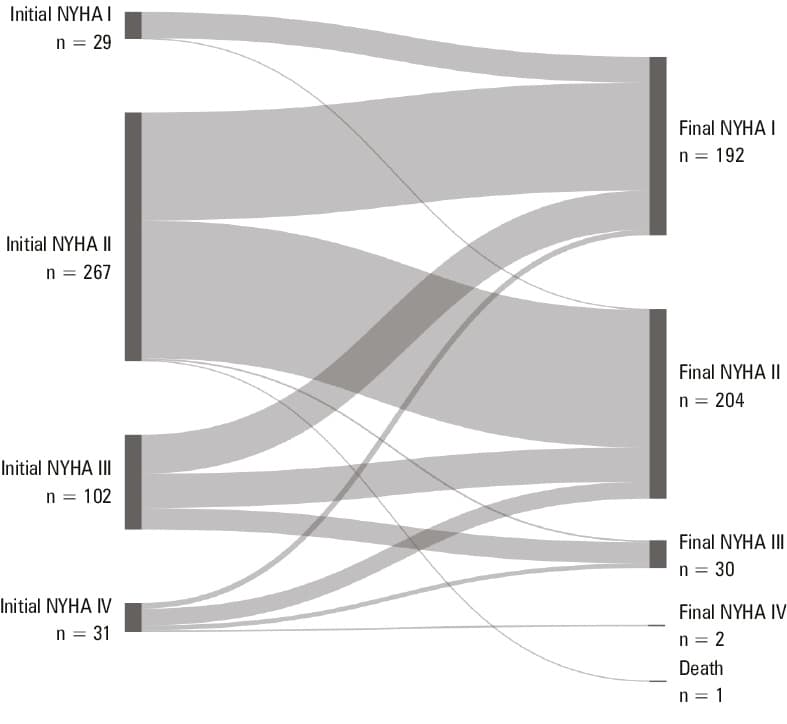
Abbreviations: NYHA, New York Heart Association
At baseline, the patients with a higher NYHA class more frequently had atrial fibrillation (AF; P = 0.002). After the 3‑month program, there was no substantial difference in the NYHA class between the patients with and without AF (P = 0.73), with its improvement being similar in both groups (P = 0.15).
For the cancer patients and the participants without cancer, there were no significant differences in the NYHA class at the beginning and end of the study. During the study, the NYHA class improvement was similar in both groups (P = 0.15).
The multivariable logistic regression showed that a history of AF and a lack of cancer were associated with an improvement in the NYHA class after the 3‑month program (Table 3).
Independent variables | OR | 95% CI | P value |
Negelkerke R2 = 0.137; P = 0.636 for the Hosmer–Lemeshow test
Abbreviations: OR, odds ratio | |||
Age, per 1 year | 0.984 | 0.964–1.004 | 0.12 |
Sex, male / female | 1.008 | 0.662–1.535 | 97 |
Atrial fibrillation, yes / no | 1.539 | 1.021–2.353 | 0.045 |
Cancer, no / yes | 2.793 | 1.224–6.369 | 0.02 |
Hospitalizations and mortality rate
In the initial questionnaire, the patients reported 41 hospitalizations within 3 months prior to the inclusion in the study, implying an incidence rate of 9.6% (95% CI, 6.9%–13%). During the 3‑month program, 1 patient was hospitalized for HF with an incidence rate of 0.2% (95% CI, 0%–1.3%), 3 patients for acute coronary syndrome, and 1 patient died (mortality rate, 0.2%; 95% CI, 0%–1.3%).
Quality of life changes
The average time between the initial and final completion of the questionnaire was 117 days. A marked improvement in the mean (SD) HRQoL between the initial and final visit was seen in the emotional function (by 1.04 [4.72] points; P <0.001), as measured by the appropriate CHFQ subscale, and in the subjective health state as measured by EQVAS (by 4.43 [21.51] points; P <0.001). The mean (SD) score on the dyspnea (–0.07 [10.95] point; P = 0.91) and fatigue (–0.1 [8.15] point; P = 0.83) subscales of the CHFQ did not show improvement after the 3‑month telemedical intervention.
The improvement in HRQoL, as measured by EQVAS, was independently associated with the physical improvement expressed as changes in the NYHA classification (Table 4). In addition, a history of AF but not the number of pharmacotherapy modifications was associated with favorable changes in HRQoL. Improvement in the emotional function was also associated with the degree of physical improvement expressed by changes in the NYHA scale (Table 4).
Dependent variables | Independent variables | β | 95% CI for β | P value |
Abbreviations: CHFQ, Chronic Heart Failure Questionnaire; EQVAS, EuroQol Visual Analog Scale; others, see Figure 3 | ||||
Change in the EQVAS score | Age, per 1 year | –0.191 | –0.427 to 0.044 | 0.11 |
Sex, male / female | –1.976 | –6.805 to 2.852 | 0.42 | |
Atrial fibrillation, no / yes | 6.162 | 1.021–11.303 | 0.02 | |
Cancer, no / yes | 3.886 | –4.839 to 12.611 | 0.38 | |
Pharmacotherapy modifications, n | –0.298 | –1.947 to 1.352 | 0.72 | |
Change in NYHA scale, n | –4.147 | –7.618 to –0.676 | 0.02 | |
Change in emotional function in the CHFQ | Age, per 1 year | –0.026 | –0.078 to 0.026 | 0.33 |
Sex, male / female | –0.837 | –1.891 to 0.218 | 0.12 | |
Pharmacotherapy modifications, n | –0.318 | –0.664 to 0.029 | 0.07 | |
Change in NYHA scale, n | –1.55 | –2.265 to –0.834 | <0.001 | |
Discussion
This study demonstrated that the 3‑month telemonitoring intervention, supervised by the GP and the cardiologist in the specific population of HF patients who live in rural areas, with often limited access to the health care system, resulted in a significant improvement of both physical capacity and QoL. The positive impact of this intervention on the physical performance was independently influenced by the presence of AF and no history of cancer. On the other hand, the observed functional benefit was not directly associated with the number of pharmacotherapy changes but rather with patient education and a multilevel, holistic approach to HF management, improving patient compliance and sense of security. Finally, an increase in physical activity independently guaranteed an improvement in QoL. Undoubtedly, the study findings provide arguments for the importance of meticulous and comprehensive telemonitoring of HF patients from rural areas.
A critical but often overlooked factor associated with poor HF outcomes is unrestricted access to specialized cardiac care, especially in small towns and rural areas far from major metropolitan centers and academic institutions.22,23 Over the last few years, innovative e‑health solutions have become more effective in diagnosis and therapy, decreasing inequalities in access to specialized medical care.24 The optimal follow‑up time of telemedicine projects is debatable. Although longer observation would provide more accurate results, in this project, the 3‑month follow‑up was established as the shortest expected to achieve any effects of the applied model.
Our results showed that more than half of such patients experienced an improvement in their functional status assessed by the NYHA classification, emphasizing the importance of a regular, structured consultation program, including teleconsultations and video consultations between the patient, the GP, and the cardiologist in the regions with limited access to specialized care. The study findings are in line with previous evidence demonstrating the effectiveness of telemonitoring in stabilizing or even improving the functional status of patients with HF.25-27 Furthermore, Inglis et al28 found that structured telephone support programs are associated with significant reductions in hospitalizations and all‑cause mortality. Cleland et al29 pointed out that patients receiving nurse telephone support or home telemonitoring had significantly lower 1‑year mortality rates (27% and 29%, respectively), as compared with those receiving usual care (45%).
In our study, there were 575 pharmacotherapy modifications. As a result, the use of β-blockers and ACEIs / sacubitril‑valsartan / angiotensin receptor antagonists achieved the levels recommended by the current guidelines.21 Simultaneously, the use of MRAs and SGLT‑2 inhibitors increased during the study period by approximately 10%; however, final levels of only 48% and 36% of the recommended use were achieved, respectively. This underuse may partly reflect the prevalence of HF with preserved left ventricular function in the study cohort, where these drugs are less frequently used, despite growing evidence of their benefit. Regardless of the high rate of pharmacotherapy adjustments, the number of modifications was not associated with the improvement in either NYHA class or the QoL parameters, suggesting the role of other possible factors. It cannot be ruled out that higher rates of MRA and SGLT‑2 inhibitor use would translate into improved NYHA class.
Lynga et al22 reported that daily electronic transmission of body weight and monitoring of its changes 3 times a week by a telephone network to a central internet‑based data server system may improve outcomes. All patients were recommended to weigh themselves daily and, in the case of a sudden weight gain above 2 kg in 3 days, to contact the HF clinic. The authors found that body weight monitoring did not reduce hospitalization or death rate in patients with HF. However, body weight management is critical in HF care, as fluid overload and weight gain are common problems that can exacerbate symptoms and lead to hospitalizations or early readmissions.30 Our study also focused on patient compliance, including regular weight and BP measurements. We found that continuous monitoring and regular interaction with health care professionals contributed to a significant median body weight loss by 1.3 kg (–0.4 to 3.1) as well as a decrease in SBP and DBP by 4 and 3 mm Hg, respectively. However, these changes did not correlate with the degree of NYHA class and QoL improvement.
The findings of our study indicate that telemedicine supports not only the physical performance of the patients but also the emotional and psychological challenges they face. The observed improvement in HRQoL is consistent with broader scientific findings, underscoring the potential of telemedical interventions to improve the outcomes in HF. Our results showed that the QoL betterment was independently influenced by changes in the NYHA classification. A meta‑analysis by Knox et al31 demonstrated a modest but significant improvement in HRQoL associated with telemedicine, as compared with routine care without remote solutions. Toukhsati et al32 pointed out that emotional health is closely related to patient self‑management and QoL in HF care. Although telemedicine algorithms seem to positively impact the QoL, the optimal duration of these interventions is still debated. Studies by Koehler et al33 and Arian et al34 showed that remote telemedical management improves both physical functioning and QoL over longer periods. These findings raise questions about whether a shorter 3‑month observation used in this study is sufficient to capture the benefits of telemedicine in HRQoL. Interestingly, Hagglund et al35 reported significant HRQoL improvements within a similar 3‑month follow‑up, suggesting that even shorter durations can be effective if well‑structured. The DIAL trial (Randomised Trial of Telephone Intervention in Chronic Heart Failure)36 demonstrated the superiority of telemedicine over traditional care, particularly by reducing the relative risk of hospitalization by 29%, which likely contributed to improved HRQoL. Additionally, HRQoL was identified as an independent predictor of all‑cause mortality and hospitalizations in patients with preserved or reduced ejection fraction.37
In our study population, the overall hospitalization rate was 9.6% within the 3‑month period prior to the enrollment, while the average 3‑month hospitalization rate in the Subcarpathian population was 11.4% during the first 3 quarters of 2023, and 10.7% for the year 2022, based on data from the National Health Fund. All of these indicators were numerically higher than the hospitalization rate in the 3‑month study period. Simultaneously, the quarterly death rate for patients with HF in the Subcarpathian voivodeship population, according to the official public payer data for the same period, was 1% and was also numerically higher than that observed in our study population.
Our study has several limitations. First, there was no control group without intervention; however, all clinical assessments were performed at baseline and after completing 3‑month follow‑up. Second, the patient assessment was based solely on clinical examination without the use of additional quantitative diagnostic tools, such as echocardiography or laboratory biomarkers. Third, seasonal effects on the study findings, with the highest incidence of cardiovascular disease observed during the colder winter months,38-40 cannot be excluded. Baseline assessments were obtained from June until September, and the 3‑month results were collected between September and December. In addition, better HRQoL outcomes are reported during the spring and summer than in the autumn and winter.41 Fourth, the results of the intervention are the effect of both e‑health model applied in this study and careful monitoring performed by the GPs and cardiologists. Finally, the exact mechanisms responsible for improving clinical aspects and QoL have not been analyzed.
In conclusion, the e‑health model applied in this study showed that telemonitoring, combined with a comprehensive patient‑oriented approach monitored by a GP under the supervision of a cardiologist, can significantly improve the functional status and QoL of HF patients in socially excluded regions. The study findings indicate that telemedicine can help reduce health care disparities by providing accessible and effective care to underserved populations. Further research should focus on the long‑term impact of telemedicine on HF outcomes, investigating the specific mechanisms by which e‑health solutions improve patient prognosis.
- Rywik TM, Wiśniewska A, Cegłowska U, et al. Heart failure with reduced, mildly reduced, and preserved ejection fraction: outcomes and predictors of prognosis. Pol Arch Intern Med. 2023; 133: 16522. | Crossref
- Niedziela JT, Rozentryt P, Nowak J, et al. Characteristics and outcomes for patients with heart failure diagnosed according to the universal definition and classification of heart failure. Data from a single‑center registry. Kardiol Pol. 2024; 82: 391‑397. | Crossref
- Puch‑Walczak A, Kunicka K, Jagiełło K, et al. Is the 2016 ESC diagnostic algorithm useful for assessing the prevalence of chronic heart failure in population‑based studies? Kardiol Pol. 2024; 82:175‑182. | Crossref
- Savarese G, Becher PM, Lund LH, et al. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. 2022; 118: 3272‑3287. | Crossref
- Szlacheta P, Malinowska‑Borowska J, Nowak JU, et al. Long‑term prognostic scores may underestimate the risk of death in patients with heart failure with reduced ejection fraction in whom red cell distribution width is elevated. Pol Arch Intern Med. 2023; 133: 16494. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION