Successful 2-stage percutaneous coronary intervention strategy with delayed stent optimization in late-presenting ST-segment elevation myocardial infarction

 CC BY 4.0
CC BY 4.0
Successful 2-stage percutaneous coronary intervention strategy with delayed stent optimization in late-presenting ST-segment elevation myocardial infarction
A 70‑year‑old man with a history of arterial hypertension, hyperlipidemia, and psoriasis was admitted due to acute chest pain lasting more than 48 hours. He had experienced exertional angina for the previous 4 months with progressive worsening of symptoms prior to admission. The electrocardiogram showed Q waves with ST‑segment elevation of 1 to 2 mm in leads II, III, and aVF. After pretreatment with aspirin and unfractionated heparin, an urgent coronary angiography via the right radial approach confirmed acute occlusion of the proximal right coronary artery (RCA) with good collateral flow from the left coronary artery (Figure 1A). Additionally, severe stenoses were detected in the left anterior descending (LAD) and circumflex arteries. A loading dose of ticagrelor was administered. Despite late presentation, intervention on RCA was attempted due to ongoing ischemia and good collateral flow. Using a 6‑F JR guiding catheter, a hybrid coating guidewire was advanced to the distal vessel with support from a 2 mm × 20 mm balloon catheter. Two passes with a 6‑F aspiration catheter were performed, retrieving large thrombus fragments (Figure 1B). When the aspiration catheter could not cross the midportion of the vessel, low‑pressure inflations with a 2.5 mm × 20 mm balloon catheter were performed, followed by repeated aspiration thrombectomy, yielding additional thrombus fragments. Further inflations up to 16 atm achieved TIMI (thrombolysis in myocardial infarction) grade 3 flow to the distal vessel. Initially, deferred stenting was planned due to uncertainty about the true vessel size and risk of no‑reflow / distal embolization from residual thrombus (Figure 1C). However, vessel reocclusion on control angiogram necessitated immediate stenting. An intentionally undersized 3 mm × 40 mm sirolimus‑eluting stent was deployed at 16 atm, with the sizing based on the distal reference vessel diameter (Figure 1D). Complete flow was maintained and the symptoms resolved.
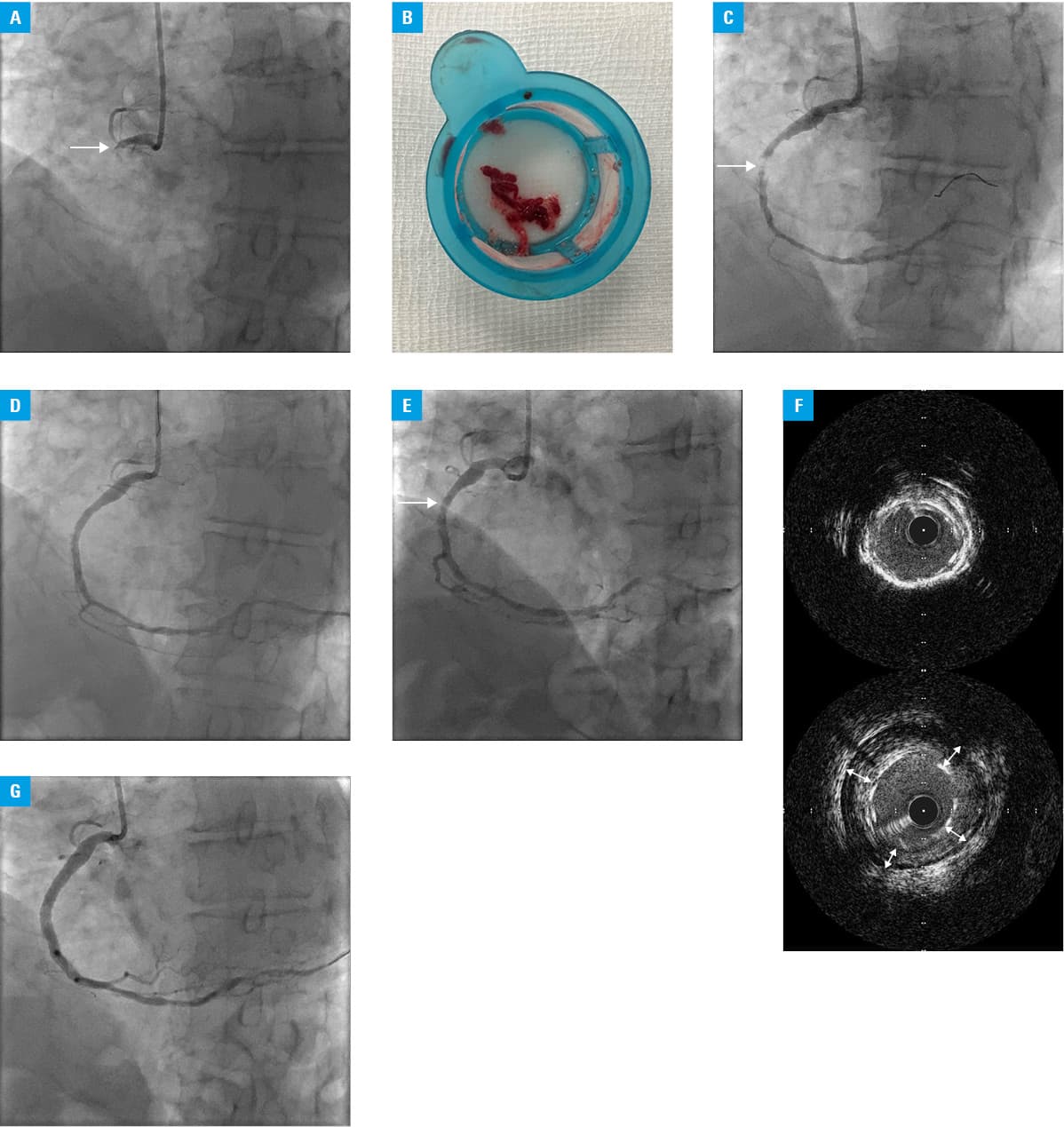
Dual antiplatelet therapy with aspirin and ticagrelor was continued and supplemented with a weight‑adjusted therapeutic dose of enoxaparin. Seven‑day follow‑up angiography confirmed optimal flow (Figure 1E). Using a 6‑F JR guiding catheter and a hybrid coating guidewire, intravascular ultrasound (IVUS) was performed, confirming proper wire position within the stent. While the distal stent segment showed optimal apposition, malapposition was noted in the proximal and midsegments (Figure 1F). High‑pressure inflations using 4.5 mm × 15 mm and 5 mm × 8 mm non‑compliant balloons (18–20 atm) were performed. Due to the edge dissection, a 5 mm × 15 mm sirolimus‑eluting stent was implanted. IVUS confirmed optimal apposition of the stents without evidence of distal embolization or compromised flow (Figure 1G). During the same procedure, successful IVUS‑guided percutaneous coronary intervention (PCI) with single everolimus‑eluting stent implantation was performed on the LAD. The patient was scheduled for medical therapy with planned PCI of the circumflex artery if angina persisted. He was discharged home 2 days later in a stable condition.
This case demonstrates a successful 2‑stage primary PCI approach for late‑presenting ST‑segment elevation myocardial infarction1 with high thrombus burden. Initial undersized stenting followed by delayed IVUS‑guided optimization reduced distal embolization risk, while ensuring optimal stent apposition.2-4 Though promising, this strategy requires careful patient selection due to temporary malapposition risks. In this case, the approach avoided additional costs and risks, as further revascularization was planned during the same hospitalization.
- Dziewierz A, Rakowski T, Mamas MA, et al. Impact of historical partitions of Poland on reperfusion delay in patients with ST‑segment elevation myocardial infarction referred for primary percutaneous coronary intervention (from the ORPKI Registry). Pol Arch Intern Med. 2024; 134: 16793. | Crossref
- Chyrchel M, Maruszak N, Pilch W, et al. Perfect optimization during coronary stent implantation ‑ is it always beneficial? Staged primary percutaneous coronary angioplasty in a young patient with acute myocardial infarction. Adv Interv Cardiol. 2022; 18: 303‑305. | Crossref
- Pradhan A, Bhandari M, Vishwakarma P, Sethi R. Deferred stenting for heavy thrombus burden during percutaneous coronary intervention for ST‑elevation MI. Eur Cardiol. 2021; 16: e08. | Crossref
- Fumanal‑Gracia M, Revilla‑Martí P, Linares‑Vicente JA, et al. Marinade technique: a strategy for thrombus burden reduction in acute coronary syndrome. Kardiol Pol. 2024; 82: 802‑803. | Crossref
ARTICLE INFORMATION