Blunt cardiac injury followed by an unusual late course of intramyocardial dissecting hematoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Blunt cardiac injury followed by an unusual late course of intramyocardial dissecting hematoma
Blunt cardiac injury involves pathologies that typically occur during or shortly after high‑impact chest trauma, from a clinically silent event to acute coronary syndrome, arrhythmias, and even a fatal cardiac wall rupture.1,2
A 57‑year‑old man, admitted in July 2021 with sustained ventricular tachycardia (sVT; Figure 1A), was successfully treated with amiodarone and electric cardioversion. His medical history included a motorcycle accident in 2017, femur transplant surgery in January 2021, and hospitalization for sVT in June 2021. The latter involved chest X‑ray and echocardiography, revealing a tumor in the left ventricle (Figure 1B and 1C). The diagnostic workup was incomplete due to the patient’s request for discharge.
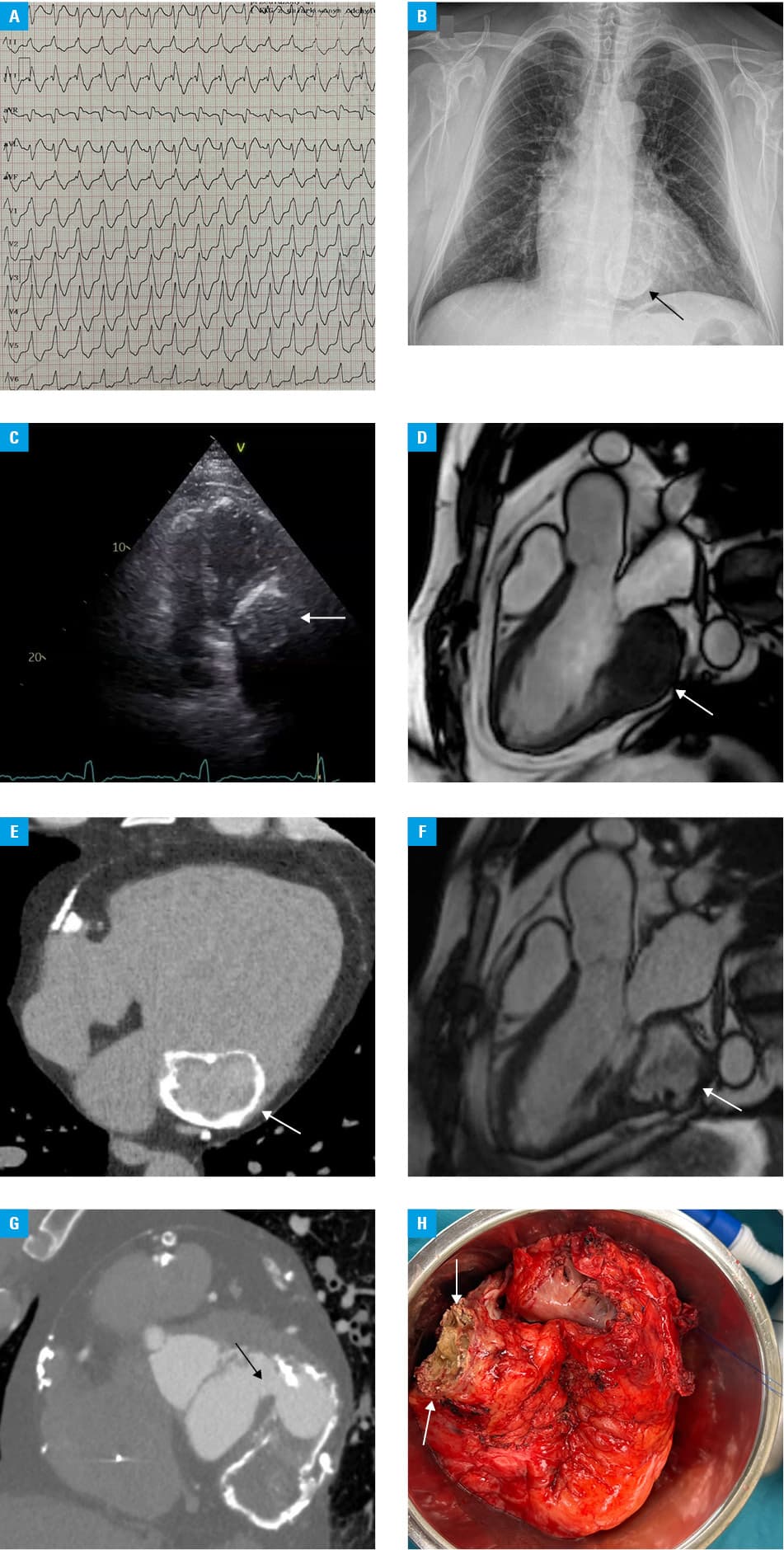
During the current hospitalization, advanced cardiac imaging with magnetic resonance (CMR) confirmed the presence of a dyskinetic tumor‑like lesion in the basal inferior and lateral segments of the left ventricle (Figure 1D). There was no contrast flow and enhancement inside the mass, confirming its avascular structure, while a uniform late gadolinium enhancement was present around the entire periphery of the lesion. This study also revealed 2 smaller tumors with a similar morphology, 1 in the area of the pulmonary valve (10 mm × 13 mm) and the other at the level of the tricuspid valve ring (6 mm × 6 mm). Computed tomography (CT) showed circumferential calcifications around the tumor (Figure 1E). Additionally, coronary angiography showed significant coronary artery disease.
Given the patient’s trauma history, a diagnosis of a calcified, encysted intramyocardial dissecting hematoma (IDH) was considered likely. A recommendation by a heart team included percutaneous coronary intervention (PCI) of the left main artery and catheter ablation of arrhythmias, while the tumor was deemed inoperable and scheduled for regular follow‑up. Over the next 6 months, the patient experienced recurrent episodes of sVT, originating, according to the electrophysiological studies, from the tumor site, unsuccessfully treated with ablations, and ultimately completed with the implantation of a cardioverter‑defibrillator in February 2022. Follow‑up CMR and CT scans showed stable tumor size, with evolving density suggesting IDH progression (Figure 1F).
Imaging examinations in November 2022 showed substantial transformation of the well‑defined tumor structure into an aneurysm filled with fresh blood, communicating with the left atrium (Figure 1G). Due to the risk of a fatal cardiac wall rupture, recurrent sVT, futility of noninvasive treatment, and no option for surgical tumor resection, the patient underwent heart transplantation (Figure 1H). Histopathologically, a post‑traumatic aneurysm involving left atrial and partially left ventricular walls was confirmed.
IDH is defined as a cavity filled with blood between the myocardial layers due to a partial rupture of the ventricular wall. It may occur as a mechanical complication of acute myocardial infarction or PCI, but rarely as a result of chest trauma, and may be associated with late presentation.1,3,4 Although treatment is not standardized, a surgical approach or even heart transplantation should be considered due to the risk of complete myocardial rupture and high mortality.3 Multimodality imaging plays a crucial role in close monitoring and guiding therapy in such patients.2,5 Echocardiography is the first‑line diagnostic tool, which should be followed by CMR and CT for better tissue characterization and precise assessment of the anatomical conditions.
- Książczyk M, Wcisło T, Warchoł I, et al. Inferior ST‑segment elevation myocardial infarction and intramyocardial dissecting hematoma following blunt chest trauma. Kardiol Pol. 2024; 82: 228‑230. | Crossref
- Nair L, Winkle B, Senanayake E. Managing blunt cardiac injury. J Cardiothorac Surg. 2023; 18: 71. | Crossref
- Rossi MP, de Abreu M, Reyes G, et al. Intramyocardial dissecting hematoma: a mechanical complication needing surgical therapy? JACC Case Reports. 2022; 4: 1443‑1448. | Crossref
- Kądzioła O, Mołek P, Zalewski J, et al. Apical intramyocardial dissecting hematoma: a rare complication of acute myocardial infarction. Pol Arch Intern Med. 2021; 131: 16055. | Crossref
- Alyousef T, Malhotra S, Iskander F, et al. Left ventricular intramyocardial dissecting hematoma: a multimodality imaging diagnostic approach. Circ Cardiovasc Imaging. 2021; 14: e012410. | Crossref
ARTICLE INFORMATION