Does high compliance with the enhanced recovery after surgery protocol improve 5-year survival? A cohort study of 468 nonmetastatic colorectal cancer patients
Key words: colorectal cancer, ERAS protocol, perioperative care

 CC BY 4.0
CC BY 4.0
Does high compliance with the enhanced recovery after surgery protocol improve 5-year survival? A cohort study of 468 nonmetastatic colorectal cancer patients
Introduction: Well‑documented immediate benefits of the enhanced recovery after surgery (ERAS) protocol highlight the need to explore its long‑term impact, particularly on survival outcomes in colorectal cancer.
Objectives: The aim of this study was to analyze the impact of the ERAS protocol compliance on the long‑term outcomes after laparoscopic colorectal resection.
Patients and methods: Data from 468 patients who underwent laparoscopic colorectal resection between 2013 and 2017 were prospectively collected. The patients were divided into 2 groups based on their adherence to the ERAS protocol, that is, group 1 with a compliance rate below 80% and group 2 with a compliance rate of 80% or higher. The association between the ERAS protocol compliance and 5‑year survival was assessed using the Kaplan–Meier method with log‑rank tests. Additionally, a survival analysis was performed separately for groups depending on cancer stages.
Results: The group 1 consisted of 128 patients, while the group 2 included 340 individuals. There were no significant differences between the groups in terms of sex, age, body mass index, American Society of Anesthesiologists scale, or comorbidities. The Kaplan–Meier curve and log‑rank test analyses indicated that the 2 groups of ERAS protocol adherence did not significantly differ in terms of 5‑year overall survival. In the patients with American Joint Committee on Cancer (AJCC) stage 1–2, those with ERAS compliance of 80% or higher had a significantly better 5‑year survival rate than those with compliance below 80%, indicating that greater adherence to the ERAS protocol is associated with improved survival outcomes. In the case of AJCC stage 3 patients, the ERAS compliance did not significantly alter survival rates.
Conclusions: High adherence to the ERAS protocol appeared to improve the 5‑year survival rate in the patients with AJCC stage 1–2 colorectal cancer.
What's new?
This study demonstrates that coordinated perioperative care, as implemented through the enhanced recovery after surgery protocol, is associated with a significant improvement in 5‑year survival rates for colorectal cancer patients with early‑stage disease (American Joint Committee on Cancer stage 1–2). However, no significant survival benefit was observed across all cancer stages, likely reflecting the dominant influence of tumor progression on long‑term outcomes. In patients with early‑stage disease, the impact of high‑quality perioperative care becomes more pronounced, underscoring its critical role in optimizing recovery and survival. These findings highlight the importance of adhering to structured, multidisciplinary care protocols in improving long‑term outcomes for patients with early‑stage colorectal cancer.
Introduction
Colorectal cancer is a health care system challenge that significantly contributes to global morbidity and mortality rates.1,2 Given complexity of this disease, there is an ongoing demand for innovative approaches to improve patient outcomes. The enhanced recovery after surgery (ERAS) protocol has transformed perioperative care, representing a significant paradigm shift in the management of colorectal cancer patients.3-5 Characterized by its evidence‑based and multidisciplinary strategies, the ERAS protocol stands as a notable advance in perioperative care for colorectal cancer.6,7 By prioritizing optimal perioperative care, minimizing complications, and facilitating a rapid recovery of surgical patients, ERAS has been widely adopted in clinical practice.3,8,9
The ERAS protocol has demonstrated substantial improvements in short‑term outcomes for colorectal surgery patients.10,11 Studies have reported a 30%–50% reduction in postoperative complications, such as infections, ileus, and anastomotic leaks. Additionally, ERAS has been associated with 20%–30% shorter hospital stays and 25%–40% faster recovery in comparison with traditional protocols.12 Patients following the ERAS protocol also resume oral intake 24 to 48 hours earlier and require 30%–50% less analgesic use, contributing to improved comfort and faster recovery.13,14 These numbers highlight the significant impact of ERAS on enhancing patient outcomes.
While the immediate benefits of ERAS in postoperative recovery are well documented and widely acknowledged, it is essential to investigate its long‑term implications, particularly its influence on the survival rates. The existing literature on this topic has yielded conflicting results.15-17
This study builds on earlier findings by Pisarska et al,18 who demonstrated a significant association between compliance with the ERAS protocol and improved 3‑year survival following laparoscopic surgery for nonmetastatic colorectal cancer. Those prior analyses highlighted the importance of adherence to ERAS principles in achieving better short- and mid‑term outcomes. By extending the follow‑up to 5 years, the current study aims to provide a more comprehensive understanding of long‑term survival, and further validate the rationale behind the 80% compliance threshold used in the stratified analysis.
This study aimed to investigate a crucial aspect of the ERAS protocol implementation: its potential impact on 5‑year survival rates among patients diagnosed with colorectal cancer.
Patients and methods
Patients and study design
The work was designed as a prospective observational study. Patients with colorectal cancer eligible for elective laparoscopic surgery at a tertiary referral center for surgical oncology were prospectively included between January 2013 and December 2017, with a follow‑up period of 5 years from the date of surgery. Initially, a total of 584 individuals undergoing treatment for colorectal cancer were eligible for the study. The patients were excluded if they were qualified for an open surgery (n = 7), emergency surgery (n = 13), or transanal endoscopic microsurgery (n = 7), had stage 4 of the disease according to the American Joint Committee on Cancer (AJCC) classification (n = 41), multivisceral resection (n = 12), concomitant inflammatory bowel diseases (n = 3), stayed in the intensive care unit immediately after surgery (n = 5), and had no follow‑up data (n = 28). After considering the abovementioned criteria, a total of 468 patients were selected for the final analysis. A detailed flowchart of the patient classification is presented in Figure 1.
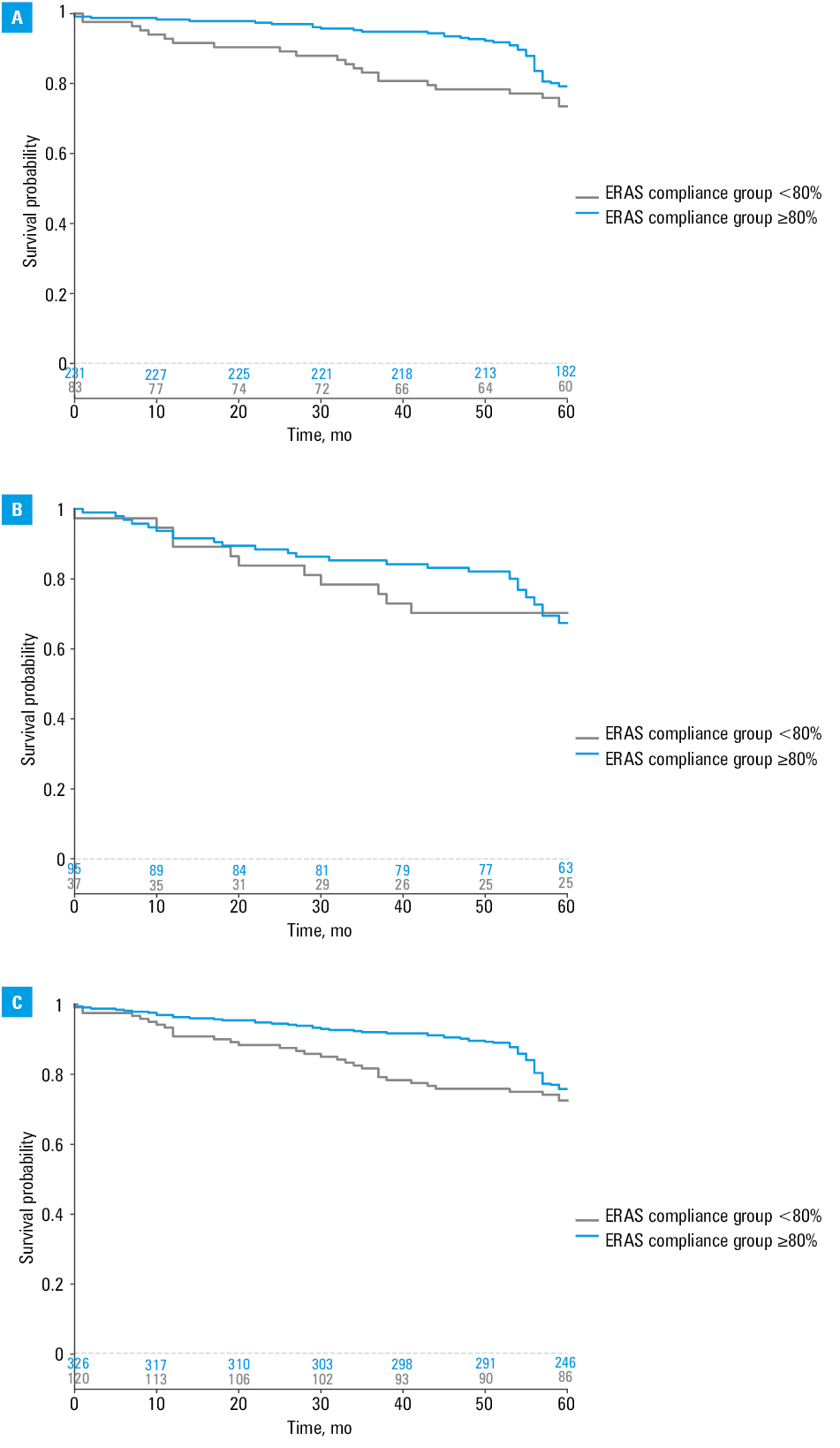
![Kaplan–Meier curves comparing 5-year survival in patients with AJCC colorectal cancer (group 1 with low [<80%] and group 2 with high [≥80%] compliance with the ERAS protocol); A – AJCC stage 1–2; B – AJCC stage 3;
C – AJCC stage 1–3
Abbreviations: see Figure 1 and Table 2](/paim/_next/image/?url=https%3A%2F%2Fpamw.pl%2Fsites%2Fdefault%2Ffiles%2Fjson_zip_files%2Funcompressed%2F16960%2FIMAGES%2FKP_WEB__FIG_01.png&w=3840&q=75)
Abbreviations: AJCC, American Joint Committee on Cancer
In our unit, laparoscopic surgery was the standard approach for all elective procedures during the study period. Perioperative care adhered to the predefined ERAS protocol comprising 16 components (Table 1). The guidelines for implementing these measures and hospital discharge criteria were established in alignment with the recommendations of the ERAS Society.14,16 Laparoscopic colonic and rectal resections were conducted in accordance with established oncological principles, as previously detailed in the literature.19
Abbreviations: iv, intravenous; TAP, transverse abdominis plane; TME, total mesorectal excision; sc, subcutaneous |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Compliance was calculated as the number of pre- and intraoperative interventions fulfilled divided by 13 (number of protocol elements included), similarly to Gustafsson et al.16 The patients were divided into 2 groups based on the ERAS protocol compliance. Group 1 comprised patients with adherence below 80%, while group 2 consisted of individuals who maintained the adherence levels of at least 80%. We established this threshold based on the compliance target set in our clinic.20 It was based on the findings from our previous study, which showed that patients achieving this level of compliance experienced significant perioperative and survival benefits. A detailed description of the elements of the ERAS protocol used in our center, as well as a summary of the surgical technique with perioperative aspects, can be found in our previous publication.18
A primary outcome of the study was the 5‑year survival rate.
According to the European Society for Medical Oncology guidelines, regular follow‑up examinations are conducted every 3–6 months during the first 2 years, and every 6 months for the next 3 years.21 Survival was confirmed using the National Personal Identification Number database.
Ethics
The ethical standards outlined by the Helsinki Declaration and its amendments were strictly followed in this study, and approval for the research was obtained from the ethics committee of the Jagiellonian University Medical College (1072.6120.225.2017). The study was registered at ClinicalTrials.gov (NCT06342687).
Statistical analysis
Statistical analysis was performed using Statistica package, version 13 (Tibco, Palo Alto, California, United States) and IBM SPSS Statistics for Windows version 29.0 software (IBM, Armonk, New York, United States). Summary descriptive statistics were used to report quantitative parameters, using the mean and SD, if the variables followed a normal distribution. The median and interquartile range were used for skewed variables. To compare quantitative parameters between the groups, the t test or the Mann–Whitney test was conducted depending on normal distribution of a variable. Qualitative variables were described using frequencies and percentages. Differences between the groups were assessed using the χ2 test. When the assumptions of the χ2 test were not met, the Fisher exact test was applied.
For survival analysis, the Kaplan–Meier method was used. To verify whether the survival curves of the low and high (≥80%) ERAS protocol compliance group differed significantly, a log‑rank test (Mantel–Cox) was performed. To determine the impact of various factors on overall survival, the Cox regression analysis was conducted. The covariates considered in the analysis included age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) score, surgical approach, neoadjuvant therapy, tumor stage, and postoperative complications of the Clavien–Dindo grade 3 or higher. To compare the effect of the ERAS protocol compliance on the overall survival in the lower cancer stage group (AJCC, 1–2) and the high cancer stage group (AJCC, 3), we used the Breslow test (overall Wilcoxon).
Cox regression results are presented as hazard ratio (HR) with 95% CI for overall 5‑year survival. Univariable analysis was performed first, followed by multivariable analysis for significant variables.
A P value below 0.05 was considered significant.
Results
Group 1 involved 128 patients with ERAS compliance rate below 80%, while group 2 consisted of 340 patients with the compliance rate of at least 80%.
There were no significant differences between the groups in terms of sex, age, BMI, ASA scale, or comorbidities. As many as 18% and 27.4% of the patients in the group 1 and 2, respectively, received neoadjuvant treatment (P = 0.04). In the group 2, there was a higher proportion of patients with rectal cancer, although this disparity did not reach statistical significance. The data are summarized in Table 2.
Parameter | Group 1 (ERAS compliance <80%) | Group 2 (ERAS compliance ≥80%) | P value | |
Data are presented as number and percentage unless indicated otherwise.
Abbreviations: ASA, American Society of Anesthesiologists physical status classification system; BMI, body mass index; ERAS protocol, enhanced recovery after surgery protocol; others, see Figure 1 | ||||
Patients | 128 (27.4) | 340 (72.6) | – | |
Women | 58 (45.3) | 165 (48.5) | 0.54 | |
Men | 70 (54.7) | 175 (51.5) | ||
Age, y, mean (SD) | 65.2 (13.5) | 64.4 (12.9) | 0.27 | |
BMI, kg/m2, mean (SD) | 26.4 (4.5) | 26.7 (4.8) | 0.58 | |
ASA scale | 1 | 8 (6.3) | 11 (3.3) | 0.06 |
2 | 69 (53.9) | 227 (66.8) | ||
3 | 48 (37.5) | 97 (28.5) | ||
4 | 3 (2.3) | 5 (1.5) | ||
Any comorbidity | 96 (75) | 246 (72.4) | 0.57 | |
Cardiovascular disease | 47 (36.7) | 104 (30.6) | 0.21 | |
Hypertension | 67 (52.3) | 185 (54.4) | 0.69 | |
Diabetes mellitus | 30 (23.4) | 59 (17.4) | 0.14 | |
Pulmonary disease | 13 (10.2) | 30 (8.8) | 0.66 | |
Colon cancer | 83 (64.8) | 200 (58.8) | 0.24 | |
Rectal cancer | 45 (35.2) | 140 (41.2) | ||
Neoadjuvant treatment | 23 (18) | 93 (27.4) | 0.04 | |
AJCC stage | 1 | 43 (33.6) | 105 (30.9) | 0.66 |
2 | 45 (35.1) | 135 (39.7) | ||
3 | 40 (31.3) | 100 (29.4) | ||
Adjuvant chemotherapy | 34 (26.6) | 86 (25.3) | 0.78 | |
Tumor grade | G1 | 22 (17.2) | 64 (18.8) | 0.48 |
G2 | 90 (70.3) | 246 (72.4) | ||
G3 | 16 (12.5) | 30 (8.8) | ||
The Kaplan–Meier curve and the log‑rank test analyses showed that the 2 groups differing in their level of adherence to the ERAS protocol were similar in terms of 5‑year overall survival.
For the entire study population (n = 468), the 5‑year survival rate was 74.4%, and there was no substantial difference between the groups with low and high compliance with the ERAS protocol (72.5% vs 75.8%; P = 0.11). Next, the 2 separate subpopulations were investigated: with AJCC stage 1–2 and AJCC stage 3. In the AJCC stage 1–2 patients, the 5‑year survival in the group with ERAS adherence of at least 80% was higher than in the group where the adherence was below 80% (79.2% vs 72.3%; P = 0.03; Figure 2). Conversely, in the patients with high cancer stage (AJCC, 3), the compliance rate of the ERAS protocol had no effect on survival (70.3% vs 67.3%; P = 0.75).
The results included in Table 3 (univariable analysis) indicated that several factors were markedly associated with 5‑year mortality. Age below 65 years (HR, 0.42; 95% CI, 0.28–0.62; P <0.001), ASA scale 1–2 (HR, 0.44; 95% CI, 0.31–0.63; P <0.001), absence of cardiovascular disease (HR, 0.51; 95% CI, 0.35–0.73; P <0.001), absence of diabetes (HR, 0.52; 95% CI, 0.35–0.77; P = 0.001), and AJCC stage 1–2 (HR, 0.67; 95% CI, 0.46–0.98; P = 0.04) were predictors of reduced 5‑year mortality. The remaining parameters, such as sex, BMI, hypertension, pulmonary disease, renal disease, tumor location, neoadjuvant treatment, time of surgery, intraoperative blood loss, postoperative complications, and compliance with the ERAS protocol had no influence on mortality (Table 3).
Parameter | HR (95% CI) | P value |
Sex (female vs male) | 0.92 (0.63–1.32) | 0.63 |
Age (<65 vs ≥65 y) | 0.42 (0.28–0.62) | <0.001 |
BMI (<25 vs ≥25 kg/m²) | 0.84 (0.58–1.22) | 0.35 |
ASA scale (1–2 vs 3–4) | 0.44 (0.31–0.63) | <0.001 |
Cardiovascular disease (no vs yes) | 0.51 (0.35–0.73) | <0.001 |
Hypertension (no vs yes) | 0.84 (0.58–1.21) | 0.35 |
Diabetes (no vs yes) | 0.52 (0.35–0.77) | 0.001 |
Pulmonary disease (no vs yes) | 0.64 (0.37–1.08) | 0.1 |
Renal disease (no vs yes) | 0.67 (0.34–1.31) | 0.24 |
Tumor location (colon vs rectum) | 1.38 (0.93–2.04) | 0.11 |
AJCC stage (1–2 vs 3) | 0.67 (0.46–0.98) | 0.04 |
Neoadjuvant treatment (yes vs no) | 1.01 (0.67–1.52) | 0.96 |
Time of surgery (<200 vs ≥200 min) | 1.3 (0.9–1.87) | 0.16 |
Intraoperative blood loss (<200 vs ≥200 ml) | 0.83 (0.55–1.27) | 0.4 |
Postoperative complications (no vs yes) | 0.72 (0.48–1.08) | 0.11 |
Compliance with ERAS protocol (≥80% vs <80%) | 0.75 (0.51–1.12) | 0.16 |
After multivariable analysis, only age below 65 years (HR, 0.54; 95% CI, 0.35–0.82; P = 0.004) and AJCC stage 1–2 colorectal cancer (HR, 0.58; 95% CI, 0.42–0.93; P = 0.04) were found to be significant predictors of reduced 5‑year mortality (Table 4).
Discussion
Our study showed that high adherence to the ERAS protocol could have a beneficial effect on long‑term overall survival in patients with early‑stage colorectal cancer (AJCC, 1–2). A high degree of protocol implementation is an independent prognostic factor for a 5‑year survival in patients with stage 1–2 colorectal cancer. We also identified age below 65 years as an independent predictor of 5‑year overall survival. Notably, adherence to the ERAS protocol did not demonstrate substantial benefits for patients diagnosed with AJCC stage 3 colorectal cancer, indicating a differential effect across various disease stages. This suggests that the benefits of the ERAS protocol may be particularly pronounced in the early stages of colorectal cancer, where timely interventions and optimized perioperative care can profoundly influence prognosis.
We observed a significant but modest improvement in survival among the patients with high compliance to the ERAS protocol and stage 1–2 cancer according to the AJCC classification. It has to be emphasized that early stages of cancer usually have a good prognosis.22 No gain from strict compliance with the ERAS protocol was found for stage 3 cancer regarding 5‑year survival. In our previous study, we found high adherence to the ERAS protocol to be beneficial regarding mid‑term outcomes.18 Gustafsson et al16 presented evidence of an improvement in cancer‑specific 5‑year survival rates. However, it is worth noting that in their study, the compliance threshold for the ERAS protocol was set at 70%.16 On the contrary, Gomaa et al15 found an improvement in short‑term, but not long‑term outcomes in patients following and not following the ERAS protocol.15 Crettenand et al23 demonstrated improved survival in patients following the ERAS protocol after radical cystectomy due to urothelial cancer, although they compared only the patients treated before and after ERAS protocol introduction, with no compliance calculation. Rubinkiewicz et al24 found no benefit of high ERAS adherence in patients with gastric cancer, and the only risk factor for premature death was stage 3 cancer according to the AJCC classification. Tidadini et al25 showed that introduction of the ERAS protocol improved 3‑year survival in colorectal cancer. In another study, Tidadini et al26 reported benefits from the ERAS protocol compliance in the elderly, with a 30% reduction of death risk. This suggests that benefits leading to survival improvement are a sum of marginal gains from the ERAS protocol elements. What is worth mentioning, nowadays the elements of the ERAS protocol are widely used in everyday clinical practice, even if the full ERAS protocol is not introduced.27 Kehlet28,29 pointed out that the use of only basic core elements of the ERAS can still hugely improve the final outcomes. According to the same authors,29,30 preoperative patient information, epidural anesthesia in open surgery, avoidance of fluid overload and hypovolemia, and avoidance of a nasogastric tube with early oral feeding should facilitate early recovery within 2–4 days.
While no significant difference in the 5‑year survival rate was observed for AJCC stage 3 patients based on the ERAS compliance, this finding likely reflects a poor long‑term prognosis inherent to advanced colorectal cancer. Nonetheless, ERAS adherence may still confer significant perioperative benefits in this group, including reduced complications, shorter hospital stays, and faster recovery, which are not fully captured in the present analysis.
Our study, despite its valuable insights, has several limitations that need to be taken into consideration. Firstly, our reliance on data sourced from the National Personal Identification Number database for overall survival lacks granularity, as this database does not provide information on the cause of death, eliminating our ability to assess cancer‑specific survival. Furthermore, the variability in the number of elements comprising different versions of the ERAS protocol introduces a potential source of bias in terms of adherence assessment. To mitigate this, we decided to focus on evaluating compliance with the 13 staff‑dependent elements of the protocol, as outlined in our previous methodology.18 While this approach allowed us to standardize our assessment, it may not fully capture the intricacies and nuances of adherence to the ERAS protocol. Additionally, we analyzed patients with both colon and rectal cancer, while it is well known that the 5‑year survival rates differ between these groups. Furthermore, it is important to note that patients with lower adherence to the ERAS protocol were more likely to have received neoadjuvant therapy (27.4% vs 18%; P = 0.04), suggesting a higher burden of the disease in this group. This difference may have contributed to the observed survival differences and represents a potential confounding factor. While our multivariable analysis was adjusted for neoadjuvant therapy, residual confounding cannot be excluded. These limitations underscore the need for caution in interpreting our findings and highlight areas for further research and refinement in future studies.
Conclusions
High adherence to the ERAS protocol may influence long‑term outcomes in patients with stage 1–2 colorectal cancer, according to the AJCC classification. These results underline the importance of tailored perioperative care strategies based on the disease stage, with a focus on maximizing adherence to the ERAS protocol in patients with stage 1 and 2 colorectal cancer to potentially enhance their long‑term outcomes.
- Sharma R, Abbasi‑Kangevari M, Abd‑Rabu R, et al. Global, regional, and national burden of colorectal cancer and its risk factors, 1990‑2019: a systematic analysis for the Global Burden of Disease Study 2019. lancet Gastroenterol Hepatol. 2022; 7: 627‑647.
- Wysocki PT. A comprehensive review on posttreatment surveillance in colorectal patients. Pol Arch Intern Med. 2021; 131: 276‑287.
- Greco M, Capretti G, Beretta L, et al. Enhanced recovery program in colorectal surgery: a meta‑analysis of randomized controlled trials. World J Surg. 2014; 38: 1531‑1541. | Crossref
- Spanjersberg WR, van Sambeeck JDP, Bremers A, et al. Systematic review and meta‑analysis for laparoscopic versus open colon surgery with or without an ERAS programme. Surg Endosc. 2015; 29: 3443‑3453. | Crossref
- Zhang W, Wang F, Qi S, et al. An evaluation of the effectiveness and safety of the Enhanced Recovery After Surgery (ERAS) program for patients undergoing colorectal surgery: a meta‑analysis of randomized controlled trials. Wideochir Inne Tech Maloinwazyjne. 2023; 18: 565‑577. | Crossref
ARTICLE INFORMATION