Single pathology, 2 clinical and therapeutic perspectives: popliteal aneurysm thrombosis as a rare cause of acute lower limb ischemia

 CC BY 4.0
CC BY 4.0
Single pathology, 2 clinical and therapeutic perspectives: popliteal aneurysm thrombosis as a rare cause of acute lower limb ischemia
Popliteal artery aneurysm (PAA) is defined as a segmental dilatation exceeding 50% of its normal diameter.1 Aneurysm thrombosis is a rare cause of acute lower limb ischemia (ALI)2 that can bring about serious health implications, including amputation or, when treated, reperfusion syndrome.3 Approximately 17%–46% of patients with PAA may develop severe ALI.4
Two men were admitted to an emergency department due to acute onset of lower limb pain. The first patient, aged 66, had a history of minor contusion of the popliteal area. The second, aged 58, reported mild‑to‑moderate dehydration due to recent food poisoning.
Patient 1
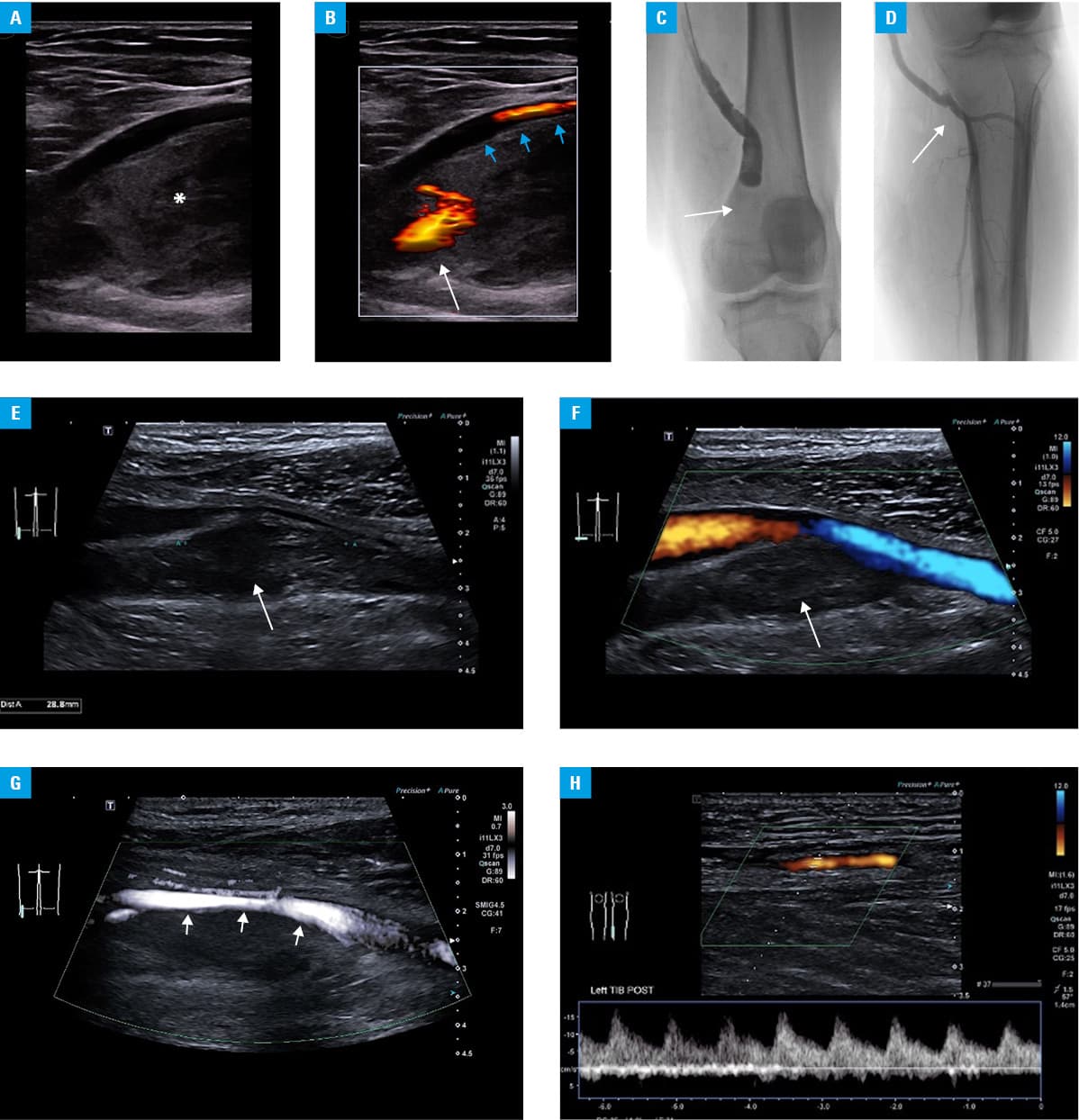
Clinical examination showed no pulse in the dorsal artery of the left foot with considerably prolonged capillary refill, severely compromised motor function, and paresthesia and rest pain. Doppler ultrasound showed 6 cm × 3 cm (length × diameter) PAA filled with heteroechoic masses that exhibited slight movement concurrent with the arterial pulsation in its proximal portion, consistent with acute thrombosis. No flow was detected in the below‑the‑knee arteries (class IIb in the Rutherford classification). The patient required immediate thrombolytic treatment, and he received a continuous infusion of alteplase delivered via an intra‑arterial catheter positioned within the thrombosed PAA. Additionally, an intra‑arterial infusion of heparin (500 IU/h) was administered distally to prevent below‑the‑knee thrombosis.
The next day, clinical improvement of the distal circulation was observed. Follow‑up angiography confirmed recanalization of the popliteal artery and below‑the‑knee arteries.
Femoropopliteal bypass surgery was performed on the same day to exclude PAA from the circulation (Figure 1A–1D). The patient developed symptoms of fascial compartment syndrome requiring urgent fasciotomy. By the following day, the distal pulse was restored and the skin temperature and function of the treated limb normalized.
Patient 2
The patient presented with symptoms of intermittent claudication occurring after walking short distances (50–100 m) for several days. The pulse on the dorsal pedal artery was absent, and the left foot was considerably colder. Motor function was slightly impaired, and sensation was limited to the distal part of the foot.
Ultrasound showed ectasia / aneurysm (13 mm in diameter) of the popliteal artery filled with heterogeneous thrombus, with no flow signals on Doppler or microvascular imaging. Low‑resistivity poststenotic flow patterns (peak systolic velocity, 5–15 cm/s) were observed in the distal two‑thirds of the posterior tibial and peroneal arteries. A monophasic (vein‑like) waveform was noted in the very distal anterior tibial artery, however, with no color‑coding (class IIa in the Rutherford classification).
Considering the subacute clinical manifestation, a decision was made to start conservative treatment with low‑molecular‑weight heparin (enoxaparin) and pentoxifylline. Popliteal and below‑the‑knee thrombectomy was performed on the following day, resulting in improved peripheral circulation. The second stage of the intervention (stent‑graft implantation) was scheduled in 3 weeks to exclude popliteal ectasia / aneurysm (Figure 1E–1H).
Popliteal artery aneurysms frequently remain asymptomatic. Trauma or dehydration may trigger the clotting cascade, resulting in aneurysmal thrombosis and ALI. While endovascular treatment has proven effective in restoring the arterial patency, selected cases still require open surgical intervention, such as thrombectomy or bypass to ensure optimal outcomes. In the case of ALI, it is essential to not only rely on diagnostic imaging, but also to take into consideration the Rutherford classification, that is, clinical factors, thorough physical examination, evaluation of motor function, possible dermatologic and trophic changes, nerve function evaluation, as well as flow evaluation to determine severity of the treatment. In our case, the thrombosed popliteal aneurysms were atypical cause of ALI.
- N’Dandu Z, Khaled K, Agbodji RA, et al. Endovascular treatment of complicated popliteal aneurysms using the novel “trap and fix” technique. JACC Case Rep. 2023; 24: 102029. | Crossref
- Natarajan B, Patel P, Mukherjee A. Acute lower limb ischemia – etiology, pathology, and management. Int J Angiol. 2020; 29: 168‑174. | Crossref
- Van DH, Boesmans E, Defraigne JO. Acute limb ischemia [in French]. Rev Med Liege. 2018; 73: 304‑311.
- Xiao X, Feng R, Wang M, et al. Comparisons of outcomes of open surgery versus endovascular intervention for thrombotic popliteal artery aneurysm with acute lower limb ischemia: a systematic review. BMC Surg. 2022; 22: 398. | Crossref
ARTICLE INFORMATION