Impact of exercise stress testing on plasma active factor VII–antithrombin levels in asymptomatic patients with aortic stenosis

 CC BY 4.0
CC BY 4.0
Impact of exercise stress testing on plasma active factor VII–antithrombin levels in asymptomatic patients with aortic stenosis
Introduction
Aortic stenosis (AS) is the most common valvular heart disease, with an estimated prevalence of 12.4% in the general population. Severe form of the disease affects 3.4% of individuals aged 75 years and older in developed countries.1 The pathophysiology of AS is complex, involving numerous interconnected mechanisms that are not yet fully elucidated.2 According to the latest European Society of Cardiology / European Atherosclerosis Society (ESC/EAS) guidelines for the management of valvular heart disease,3 exercise stress testing is recommended for asymptomatic patients to provide additional prognostic information. Stress echocardiography can further improve risk stratification and identify asymptomatic patients who are at a higher risk for cardiac events.3 Kolasa‑Trela et al4 showed that exercise stress testing in asymptomatic individuals with moderate‑to‑severe AS triggered prothrombotic changes, reflected by increased endogenous thrombin potential and prolonged clot lysis time associated with elevated levels of plasminogen activator inhibitor‑1, as well as a rise in the levels of interleukin (IL)-6, IL‑10, and growth factors.5 Similar observations were made in symptomatic severe AS patients, in whom coagulation activation was associated with inflammation, oxidative stress, and AS progression.6-9
Cardiomyocytes and fibroblasts consistently express high levels of tissue factor (TF), whereas TF is not detectable in skeletal muscles.10 Interestingly, it has been shown that TF is abundant within stenotic leaflets.6 TF, exposed upon endothelial damage, initiates the extrinsic coagulation pathway and is a high‑affinity receptor for active factor VII (FVIIa). The TF‑FVIIa complex activates factors IX and X, driving thrombin generation and fibrin formation. Antithrombin (AT) targets TF‑bound FVIIa to form FVIIa‑AT complexes.11 Of note, high FVIIa‑AT levels were shown to correlate with high TF mRNA levels12; therefore, FVIIa‑AT complexes have been proposed as a measure of TF exposure and an indirect marker of the TF‑FVIIa complex formation in vivo.13 To our best knowledge, there have been no reports on the effect of exercise on FVIIa‑AT complexes in humans. We aimed to investigate whether asymptomatic AS patients have higher FVIIa‑AT levels than well‑matched controls, and how exercise stress testing affects FVIIa‑AT complexes.
Patients and methods
Patients
We studied 31 consecutive asymptomatic patients with AS (mean [SD] age, 64.6 [11] years; 14 men [45.2%]) and 31 age-, sex-, and body mass index (BMI)-matched controls, who were selected from among the families of hospital personnel (Supplementary material, Table S1). All participants were enrolled between March 2011 and June 2012 at the St. John Paul II Hospital in Kraków, Poland. The study groups have been described in detail previously.4,5 In brief, asymptomatic patients with moderate‑to‑severe AS, free of significant atherosclerotic vascular disease, were enrolled based on the ESC/European Association for Cardio‑Thoracic Surgery guidelines for managing valvular heart disease.3 We excluded the participants with a history of myocardial infarction, stroke, atrial fibrillation, venous thromboembolism, dizziness, syncope, or any other significant valvular heart disease. Additional exclusion criteria comprised left ventricular ejection fraction (LVEF) below 50%, insulin‑dependent diabetes mellitus, severe renal or hepatic dysfunction, the use of nonsteroidal anti‑inflammatory drugs other than aspirin, and inability to perform exercise testing. Definitions of comorbidities were previously described.4,5 To assess atherosclerotic vascular disease, the intima‑media thickness of the right and left common carotid arteries was measured, as described before.4,5
The study was approved by the Ethics Committee (Krakow District Medical Chamber, Poland; 26/KBL/OIL/2011), and all participants gave written informed consent in compliance with the Declaration of Helsinki.
Exercise test
Symptom‑limited exercise stress echocardiography was conducted on a semi‑supine bicycle ergometer (Ergoline, Bitz, Germany) under continuous monitoring by an experienced cardiologist. Transthoracic echocardiography (Philips iE33, Andover, Massachusetts, United States) was used to evaluate parameters such as LVEF, peak transvalvular velocity (Vmax), and mean and maximal transvalvular pressure gradients (PGmean, PGmax) in both AS patients and controls. Starting at 25 W, the workload was increased by 25 W every 3 minutes, as detailed earlier.4,5 Blood pressure and electrocardiogram were monitored throughout the test, and exercise was stopped upon patient request, upon occurrence of symptoms such as chest pain, dyspnea, dizziness, fatigue, hypotension, or arrhythmia, or in the case of reaching the maximum heart rate. Echocardiography was conducted at rest and peak exercise.
Laboratory analysis
Fasting venous blood was collected from the antecubital vein of the AS patients and controls. Routine laboratory workup was performed at the hospital laboratory, including measurement of C‑reactive protein and fibrinogen levels. Blood samples for hemostatic variables, including FVIIa‑AT complexes, were collected before exercise, at peak exercise, as well as 1 hour and 24 hours postexercise. The samples were centrifuged at 2500 g for 20 minutes at 20 °C, and stored at −80 °C until analysis. Using the enzyme‑linked immunosorbent assay, we determined plasma FVIIa‑AT complexes (Diagnostica Stago, Asnières‑sur‑Seine, France) according to the manufacturer’s instruction. The reference range for FVIIa‑AT was between 75 and 220 pM. Thrombin endogenous potential was assessed in plasma samples using calibrated automated thrombography (Thrombinoscope BV, Maastricht, Netherlands), as described previously.4
Statistical analysis
Categorical variables were presented as counts and percentages, while continuous variables were expressed as mean and SD or median with interquartile range. Categorical variables were analyzed using the χ2 test with the Yates continuity correction or the 2‑tailed Fisher exact test. Normality was checked using the Shapiro–Wilk test. Differences between the AS and control groups were analyzed using the t test or the Mann–Whitney test, as appropriate. To compare dependent variables (before and after exercise), the t test for dependent samples was used for the normally distributed variables, while for the variables with a non‑normal distribution, the Wilcoxon signed‑rank test was used. To analyze differences across 4 time points during the exercise stress testing, the Friedman test with Dunn post hoc analysis were used, as the variables were non‑normally distributed. Associations between the variables were calculated using the Pearson or Spearman correlation coefficients, as appropriate. A P value below 0.05 was considered significant. All statistical analyses were performed using the Statistica software (version 13.3, Tibco Software, Palo Alto, California, United States).
Results
Baseline characteristics of the AS patients and controls are presented in Supplementary material, Table S1. No significant differences were observed between the groups with respect to demographic characteristics or risk factors. However, the AS patients more often used acetylsalicylic acid and had higher systolic blood pressure than the controls (P = 0.04 and P = 0.008, respectively; Supplementary material, Table S1). In terms of hemodynamic parameters, the AS patients demonstrated a 7.5‑fold higher PGmean, a 6.9‑fold higher PGmax, and a 1.7‑fold higher Vmax than the controls (all P <0.001; Supplementary material, Table S1). Following the exercise stress test, the controls exhibited a 7.1% increase in LVEF, while the AS patients showed a 10.6% increase, along with a 17.6% rise in PGmean and a 16.4% increase in PGmax (all P <0.001). In the control group, the exercise test duration was by 11.1% longer (P = 009), and the maximum workload was by 33.3% higher (P = 0.001) than in the AS patients. No differences were found between the groups in routine laboratory parameters (Supplementary material, Table S1).
At baseline, there was no difference in FVIIa‑AT levels between the AS patients and controls (Figure 1A). The patients with AS had by 25.1% higher FVIIa‑AT levels than the controls at peak exercise (P <0.001; Figure 1A). In both the AS and control participants, FVIIa‑AT complex levels reached the highest values 1 hour postexercise, but the AS patients had by 25.7% higher FVIIa‑AT levels than the controls at this time point (P <0.001; Figure 1A). No differences in FVIIa‑AT complex levels were found between the groups 24 hours postexercise (Figure 1A).
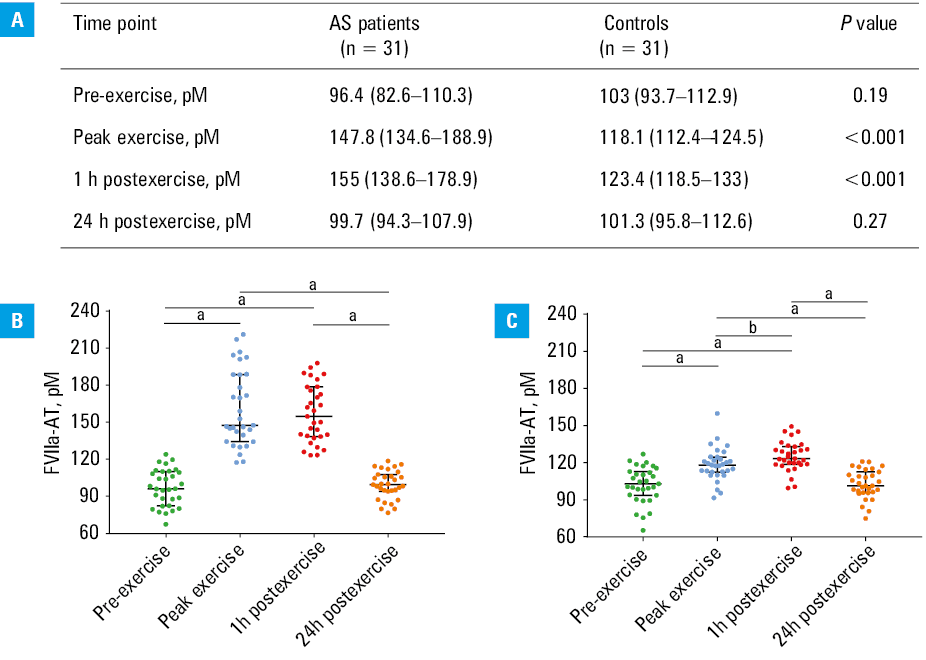
a P <0.001; b P <0.01
In the AS patients, the FVIIa‑AT complex levels increased at peak exercise relative to the baseline by 51.7%, and 1 hour after exercise by 61.6% (both P <0.001; Figure 1B), while 24 hours postexercise, they decreased by 32.7%, as compared with the values at peak exercise (P <0.001) and reached the pre‑exercise levels (Figure 1B). Similarly, in the control group, the FVIIa‑AT complex levels were by 15.8% higher at peak exrecise and by 22.7% higher at 1 hour after exercise, as compared with the baseline (both P <0.001; Figure 1C). Moreover, FVIIa‑AT levels were slightly higher (+6%) 1 hour after exercise as compared with the levels at peak exercise (P = 0.003), while 24 hours postexercise, they returned to baseline values (–13% as compared with peak exercise values; P <0.001; Figure 1C).
Peak thrombin levels were approximately by 23% higher in the AS patients during exercise and 1 hour postexercise, and by 46.8% higher 24 hours postexercise, as compared with the control individuals (all P <0.001; Supplementary material, Table S2).
FVIIa‑AT levels correlated with age only in the control group at all time points (baseline, R = 0.52; P = 0.003; peak exercise, R = 0.53; P = 0.002; 1 h postexercise, R = 0.56; P = 0.001; 24 h postexercise, R = 0.48; P = 0.006). No associations were observed between FVIIa‑AT levels and BMI, exercise variables, laboratory parameters (including peak thrombin), or echocardiographic measures of AS severity in either group at any time point.
Discussion
To the best of our knowledge, this is the first study to demonstrate that exercise stress testing induced an increase in plasma FVIIa‑AT levels in asymptomatic patients with moderate‑to‑severe AS and control individuals. Peak FVIIa‑AT levels were observed 1 hour postexercise, and were about 25% higher in the AS patients than in the controls, which indicates that enhanced TF exposure following the exercise stress test is more pronounced in AS. However, after 24 hours, TF exposure returned to the baseline values, without intergroup differences.
The mechanisms behind increased TF exposure induced by exercise in asymptomatic AS patients as compared with controls are unclear. Inflammatory markers or thrombin generation cannot explain this phenomenon. It might be speculated that increased oxidative stress during the exercise stress test, combined with hemodynamic disturbances associated with disease severity,7 may increase the exposure of TF in the vessels (despite an absence of clinically evident coronary or peripheral artery disease). We cannot exclude the role of stenotic valves as an additional source of TF potentiating TF exposure.
It has been previously reported by Weiss et al14 that running exercise does not enhance TF expression, as indicated by a lack of any effect on monocyte‑expressed TF and both protein and mRNA levels of TF in blood, as well as a lack of increase in FVII coagulant activity. In contrast to our findings, the authors concluded that physical activity does not trigger coagulation activation by the TF‑dependent pathway in young healthy volunteers.14 However, these discrepancies may be partially attributed to the younger age of the participants of the previous study,14 who were around 20 to 30 years old, while our control group consisted of individuals approximately 60 years old. On the other hand, that same study demonstrated an exercise‑induced increase in thrombin markers in plasma, that is, prothrombin fragment 1+2, thrombin‑AT complexes, and fibrinopeptide A, in endurance‑trained young men.14 Several mechanisms have been proposed for exercise‑induced coagulation activation, including a significant increase in shear stress and catecholamine release, which are crucial for platelet activation during exercise.15 In our study, control individuals displayed slightly higher FVIIa‑AT levels at peak exercise and 1 hour postexercise as compared with the baseline, while the AS patients showed a pronounced increase. In our opinion, the observed discrepancy may be related to different methodological approaches used to measure TF concentrations, with our study utilizing FVIIa‑AT complexes as an indirect measure of TF levels, while Weiss et al14 determined plasma levels and activity of TF and FVII separately. On the other hand, we postulate that the high shear stress inherent to AS, intensified by exercise testing, may partially explain the increased FVIIa‑AT levels observed in the AS patients, as compared with the controls, especially since the duration of exercise and maximum workload were significantly lower in the AS group. Although no correlation was identified at any time point between FVIIa‑AT levels and echocardiographic parameters of AS severity, we noted enhanced hemodynamic changes induced by exercise in the AS patients, as reflected by an increase in both transvalvular pressure gradients and LVEF, which aligns with previous studies.4,5 This observation suggests a contribution of other mechanisms, such as oxidative stress. Siudut et al7 demonstrated that severe AS patients had enhanced oxidative stress, as indicated by increased plasma protein carbonyl levels. It is known that oxidative stress, especially the generated free radicals, affects vascular endothelium and monocytes, which constitutively express TF.16 It may be speculated that in AS patients, due to continuous shear stress, cells are prone to activation, which may result in higher levels of TF, as reflected by increased levels of FVIIa‑AT complexes during exercise. This also accords with our earlier observations, showing that exercise stress testing in asymptomatic AS patients was associated with both enhanced blood coagulation and impaired fibrinolysis,4 which could be affected by exercise‑related oxidative stress.17 Considering the similarities between AS and atherosclerosis, it is worth noting the study by Paszek et al,18 demonstrating that in patients with advanced coronary artery disease, FVIIa‑AT levels correlated with the presence of activated FXI and TF, as well as with the levels of prothrombin fragment 1+2 and isoprostanes, markers specific to oxidative stress. Moreover, higher levels of FVIIa‑AT complexes assessed at baseline were linked to an increased risk of ischemic stroke and / or systemic thromboembolism over a follow‑up period of more than 8 years.18
It is tempting to speculate that recombinant tissue factor pathway inhibitor (TFPI), which has been tested in an experimental venous thrombosis model,19 could offer potential benefits for patients with elevated levels of the TF‑VIIa complex. However, recombinant TFPI is still under investigation, and its use is not yet widespread in clinical practice.
This study has several limitations that should be considered when interpreting its findings. First, the small sample size may limit the generalizability of the results. However, it is important to note that this research specifically focuses on a representative cohort of asymptomatic patients with moderate‑to‑severe AS who were capable of performing an exercise test. Second, the findings cannot be easily generalized to individuals with mild AS, as their physiological responses to exercise may differ. Third, assessing oxidative stress, measured as plasma protein carbonyl or isoprostane levels, could also provide valuable insights into the interaction between oxidative stress and coagulation during exercise testing in individuals with asymptomatic AS. Additionally, exercise testing was conducted using a bicycle ergometer, which may not fully replicate the physiological responses observed with other exercise modalities, suggesting that future studies employing alternative exercise protocols could offer additional insights. Finally, the timing of exercise plays a role, since it has been described that short‑duration, high‑intensity exercise increases plasma TF concentrations, particularly in the morning.20
In conclusion, our study showed that in asymptomatic patients with moderate‑to‑severe AS, FVIIa‑AT levels increased during exercise stress testing, as compared with controls, suggesting that hemodynamic disturbances associated with the disease severity may contribute to a prothrombotic state in these patients.
- Osnabrugge RL, Mylotte D, Head SJ, et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta‑analysis and modeling study. J Am Coll Cardiol. 2013; 62: 1002‑1012. | Crossref
- Yetkin E, Waltenberger J. Molecular and cellular mechanisms of aortic stenosis. Int J Cardiol. 2009; 135: 4‑13. | Crossref
- Vahanian A, Beyersdorf F, Praz F, et al; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022; 43: 561‑632. | Crossref
- Kolasa‑Trela R, Fil K, Wypasek E, Undas A. Exercise stress testing enhances blood coagulation and impairs fibrinolysis in asymptomatic aortic valve stenosis. J Cardiol. 2015; 65: 501‑507. | Crossref
- Kolasa‑Trela R, Konieczynska M, Bazanek M, Undas A. Specific changes in circulating cytokines and growth factors induced by exercise stress testing in asymptomatic aortic valve stenosis. PLoS One. 2017; 12: e0173787. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION