The diverticular inflammation and complication assessment classification: ready to use, easy to use, must be used
1,2

 CC BY 4.0
CC BY 4.0
The diverticular inflammation and complication assessment classification: ready to use, easy to use, must be used
Although diverticulosis is the most frequent anatomical alteration detected on colonoscopy,1 its endoscopic classification has been absent for many years. Despite a large number of examinations quite frequently revealing not only diverticulosis but also signs of endoscopic inflammation without any clinical suspicion of acute diverticulitis,2,3 the first endoscopic classification of diverticular disease (DD), called Diverticular Inflammation and Complication Assessment (DICA), was presented only in 2015.4 This classification overcame the flaws of previous definitions describing too vaguely the colon with diverticulosis on colonoscopy, leading to the development of an easy‑to‑use 3‑step score (DICA 1, DICA 2, and DICA 3).4
In a long process of national5 and international6 validation, 2 international studies, 1 retrospective7 and 1 prospective,8 confirmed a significant predictive value of this classification in terms of acute diverticulitis occurrence / recurrence and a risk of surgery within up to 3 years.
This classification is also significantly associated with the severity of symptoms (in particular the severity of abdominal pain, diarrhea, and constipation),9 with the value of erythrocyte sedimentation rate, and the levels of C‑reactive protein4 and fecal calprotectin.10 In other words, the severity of some clinical and laboratory findings is linked to the higher risk of finding a more severe DICA degree on colonoscopy.
In this issue of Polish Archives of Internal Medicine, Pietrzak et al11 report on the results of a 12‑month prospective study performed in asymptomatic patients with diverticulosis. The authors did not find any role of the DICA score in predicting the occurrence of diverticulitis in this cohort of patients, questioning therefore its actual usefulness, at least in asymptomatic individuals. Of course, these disappointing results may confound the reader, because they seem to reduce the role of the DICA classification. However, the key to explain the results reported by Pietrzak et al11 is the type of patients enrolled. Only asymptomatic patients were investigated in that study, and we know that such patients are mainly classified into the DICA 1 group (simple diverticulosis without any endoscopic signs of current or past diverticular inflammation), and that such a mild DICA score is not a risk factor for diverticulitis or surgery.8 Of course, signs of inflammation may be also detected in asymptomatic patients, but this occurs in about 0.8%–3% of individuals with asymptomatic diverticulosis.2,3 This may therefore explain the lower prevalence of DICA 2 and DICA 3 in the population studied by Pietrzak et al.11 Moreover, we know that asymptomatic diverticulosis does not translate into changes in the gut microbiota,12 and does not produce significant signs of inflammation on microscopy.13 Finally, we know that the risk of diverticulitis in asymptomatic diverticulosis is very low, reaching the rate of 4% at 10 years.14 Thus, the short follow‑up duration (12 months) may also explain the low rate of diverticulitis in the study by Pietrzak et al.11 Putting these data together, and as already highlighted by the authors,11 their disappointing results can be clearly and convincingly explained.
However, this study opens an interesting question in real life: if I detect colonic diverticulosis during a screening colonoscopy in an asymptomatic patient who shows no signs of diverticular inflammation (namely a DICA 1 patient), how to advise them on their diverticulosis and potential risk of diverticulitis in the future?
To try to answer this question, we need to remember that DICA is a dynamic classification that may be influenced by treatment. For example, we know that rifaximin or mesalazine, 2 main medications for DD, may impact mucosal inflammation.1 This may be responsible for a surprisingly low DICA score in patients undergoing colonoscopy after an episode of acute diverticulitis.15 Thus, the DICA score may show its real efficacy in predicting the course of the disease only in patients at the first diagnosis of diverticulosis or DD.
Moreover, patient age at diagnosis and the type of symptoms (mainly abdominal pain) have been identified as risk factors for further diverticular complications in individuals classified with the DICA score.8 To further improve the score, we developed a new one called Combined Overview on Diverticular Assessment (CODA) including endoscopic and clinical features.8 This score combines the DICA score, age at diagnosis, and severity of abdominal pain, yielding 3 different subscores (CODA A, CODA B, and CODA C), and showing a significant relationship between the severity of CODA score and the risk of diverticulitis and surgery.8 Further, this score is enhanced by incorporating the fecal calprotectin levels. The combination of CODA score (ie, DICA score + age at diagnosis + severity of abdominal pain) and fecal calprotectin levels equal to or above 90 µg/g may define a short‑term risk of diverticulitis.10
The last question is how DICA classification may help physicians choose the right therapy addressing the symptoms and severity of the score? According to a retrospective study on DICA classification,7 only DICA 2 patients benefited from a treatment aimed at preventing the occurrence of diverticulitis, and mesalazine‑based therapies were the most effective in this setting. In other words, in DICA 1 patients, if symptomatic, we just need to treat the symptoms and further surveillance is not necessary, as the risk of complications is very low. In DICA 3 patients we also just treat the symptoms, but the patients need strict surveillance, especially if fecal calprotectin levels are equal to or higher than 90 µg/g, as the risk of complications is high and the therapies may be insufficient to prevent them.10 Further prospective studies are welcome in this setting. In the meanwhile, Figure 1 shows a flow chart suggesting the possible short‑term risk stratification of patients in whom colonic diverticulosis was detected on endoscopy and diagnosed for the first time.
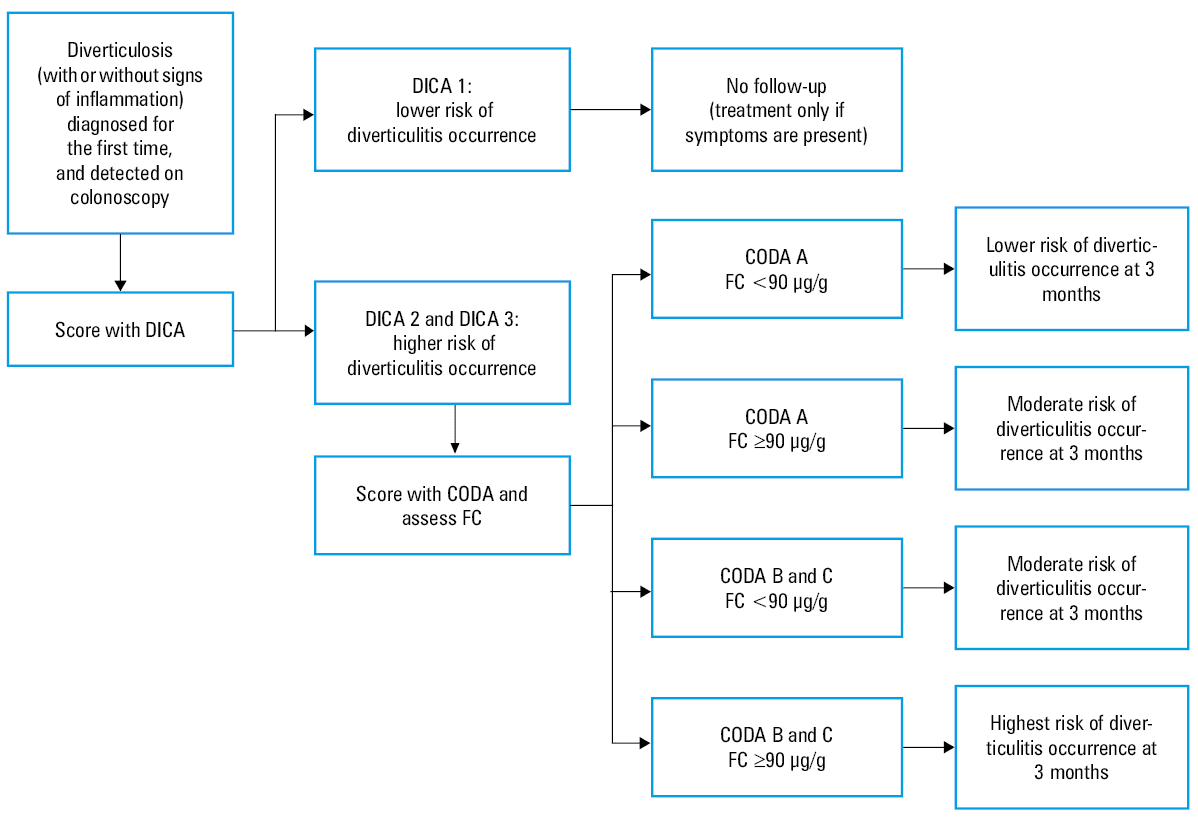
Abbreviations: CODA, Combined Overview on Diverticular Assessment; DICA, Diverticular Inflammation and Complication Assessment; FC, fecal calprotectin
- Tursi A, Scarpignato C, Strate LL, et al. Colonic diverticular disease. Nat Rev Dis Primers 2020; 6: 20. | Crossref
- Ghorai S, Ulbright TM, Rex DK. Endoscopic findings of diverticular inflammation in colonoscopy patients without clinical acute diverticulitis: prevalence and endoscopic spectrum. Am J Gastroenterol 2003; 98: 802‑806. | Crossref
- Tursi A, Elisei W, Giorgetti GM et al. Inflammatory manifestations at colonoscopy in patients with colonic diverticular disease. Aliment Pharmacol Ther. 2011; 33: 358‑365. | Crossref
- Tursi A, Brandimarte G, Di Mario F et al. Development and validation of an endoscopic classification of diverticular disease of the colon: the DICA classification. Dig Dis. 2015; 33: 68‑76. | Crossref
- Tursi A, Brandimarte G, di Mario F, et al; DICA Italian Group. The “DICA” endoscopic classification for diverticular disease of the colon shows a significant interobserver agreement among community endoscopists. J Gastrointestin Liver Dis. 2019; 28: 23‑27. | Crossref
ARTICLE INFORMATION