Massive recurrent ovarian cysts with oligomenorrhea as a clinical manifestation of pituitary gonadotropinoma

 CC BY 4.0
CC BY 4.0
Massive recurrent ovarian cysts with oligomenorrhea as a clinical manifestation of pituitary gonadotropinoma
A 33‑year‑old woman was admitted to an endocrinology department for a diagnostic evaluation of oligomenorrhea and recurrent, massive ovarian cysts. Prior to hospitalization, she had undergone diagnostic and therapeutic interventions at a gynecological outpatient clinic. For over 5 years, the patient had reported persistent lower abdominal pain and recurrent ovarian cysts, unsuccessfully managed with multiple ovarian cauterization procedures.
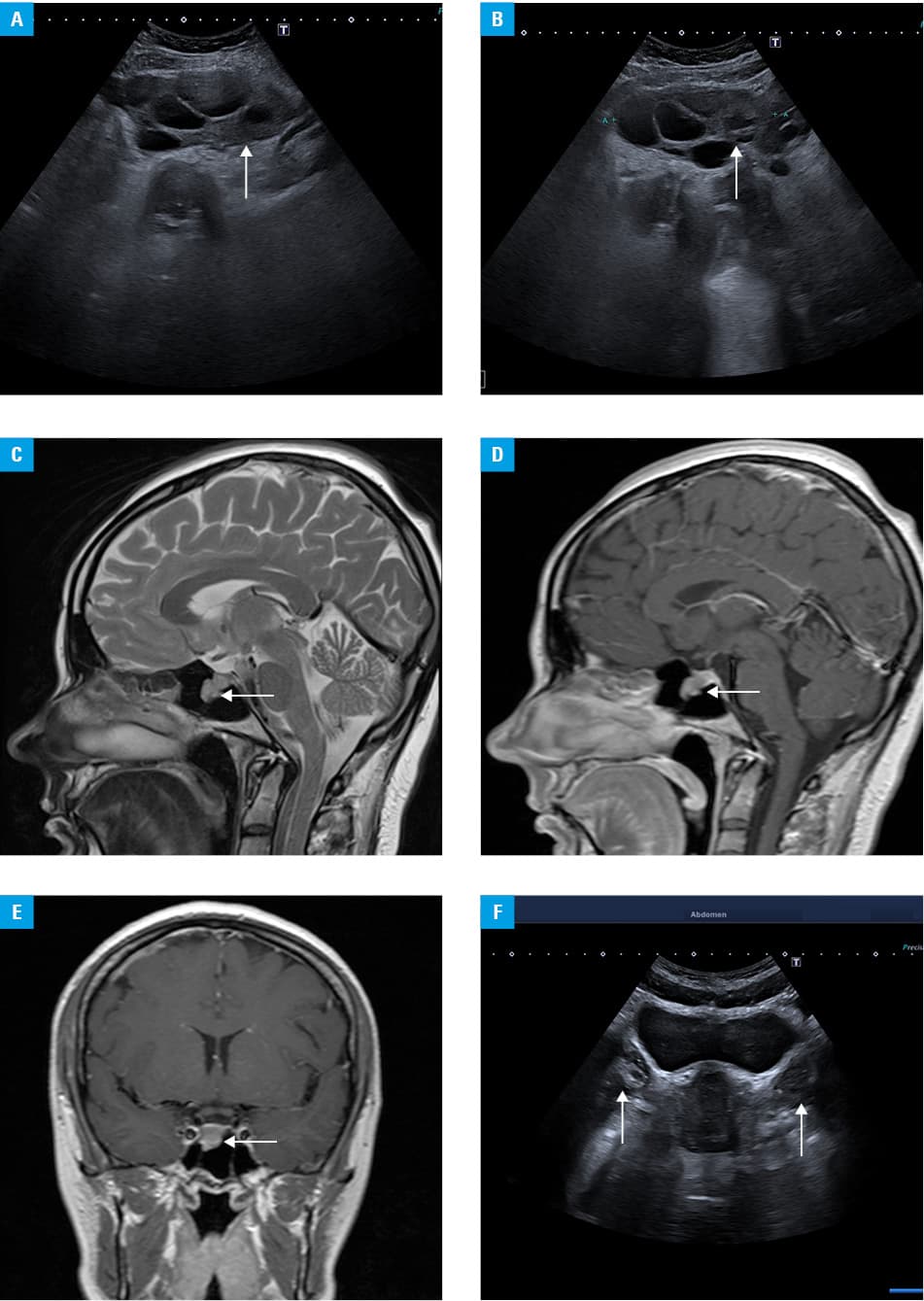
A consultation with a gynecologist‑endocrinologist was initiated due to a suspicion of a gonadotropin‑secreting tumor. During hospitalization, transabdominal ultrasonography (Figure 1A and 1B) showed multicystic ovaries. The dimensions of the right ovary were 88 mm × 49 mm × 100 mm, while the left ovary measured 80 mm × 49 mm × 59 mm. The uterus exhibited normal ultrasonographic appearance. Laboratory tests performed on day 30 of the menstrual cycle showed the following hormone levels: follicle‑stimulating hormone (FSH) of 13.89 IU/l (reference range [RR], 1–8 IU/l), luteinizing hormone (LH) of 0.1 IU/l (RR, 1–8 IU/l), estradiol of 3612.6 pmol/l (RR, 308–3561 pmol/l), and progesterone of 7.31 nmol/l (RR >31.8 nmol/l). Subsequently, a thyrotropin‑releasing hormone (TRH) stimulation test was conducted, with results summarized in Supplementary material, Table S1. Additional laboratory findings included an elevated α subunit (α-SU) level of 1.1 IU/l (RR, 0–0.7 IU/l), whereas the level of anti‑Müllerian hormone (AMH) was 5 pmol/l (RR, 5–54 pmol/l). Magnetic resonance imaging (MRI) of the pituitary gland demonstrated a focal lesion on the right side, measuring 4.8 mm × 8.1 mm (Figure 1C–1E). Subsequent abdominal MRI confirmed the presence of massive cystic lesions in both ovaries, but with no suspicion of neoplasm. Based on the clinical picture and laboratory results, pituitary gonadotropinoma was established as the initial diagnosis.
Subsequently, the patient underwent transsphenoidal surgery for the pituitary adenoma. Postoperative FSH levels declined sequentially from 3.16 IU/l to 1.59 IU/l and finally, to 1.02 IU/l; the LH level remained below 0.1 IU/l, and the estradiol concentration decreased to 1002.3 pmol/l. Histological examination confirmed pituitary adenoma (pituitary neuroendocrine tumor) with a Ki‑67 proliferation index of 3%. Immunohistochemical staining was negative for the growth hormone, prolactin, adrenocorticotropic hormone, thyroid‑stimulating hormone, and LH, while it was strongly positive for FSH and weakly positive for the α-SU.
During the follow‑up hospitalization 5 months after the surgery, imaging of the ovaries did not show any abnormalities (Figure 1F), and the patient’s regular menstrual cycle returned. On day 5 of the menstrual cycle, laboratory results showed the following hormone levels: estradiol of 298 pmol/l, LH of 7.25 IU/l, FSH of 9.35 IU/l, and the progesterone concentration of 0.96 nmol/l. The patient remained under endocrinological and gynecological surveillance for the next 6 months, with no evidence of pituitary insufficiency or recurrence of ovarian cysts.
Gonadotropinoma is a rare subtype of pituitary adenoma that typically exhibits minimal or no clinical symptoms in the general population.1,2 In most cases, the initial presentation is related to the tumor’s mass effect. However, in younger individuals, symptoms related to dysregulation of the hypothalamic‑pituitary‑gonadal axis may predominate. Diagnostic evaluation can be challenging, although α-SU and AMH measurements, as well as TRH stimulation testing provide valuable information.
The principal treatment is transsphenoidal surgical resection performed in specialized centers. In selected cases, particularly those with smaller tumors and mild clinical symptoms, conservative management involving observation or pharmacotherapy with somatostatin analogs may be considered.
- Rak B, Maksymowicz M, Grzywa TM, et al. Pituitary tumours ‑ a large retrospective single‑centre study of over 2300 cases. Experience of a tertiary reference centre. Endokrynol Pol. 2020; 71: 116‑125. | Crossref
- Asa SL, Mete O, Perry A, Osamura RY. Overview of the 2022 WHO classification of pituitary tumors. Endocr Pathol. 2022; 33: 6‑26. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION