Hepatocellular carcinoma in a young patient with hypoplastic left heart syndrome with Fontan circulation

 CC BY 4.0
CC BY 4.0
Hepatocellular carcinoma in a young patient with hypoplastic left heart syndrome with Fontan circulation
The Fontan procedure remains the treatment of choice for patients with a functionally single ventricle heart. It results in improved patient survival, but over time leads to multiorgan complications, including Fontan‑associated liver disease (FALD), affecting all Fontan patients.1 Severe liver damage seems to be the main substrate for the risk of hepatocellular carcinoma (HCC), which affects only 1%–2% of Fontan patients, but is associated with a grim 1‑year survival rate of only 50%.2-4 However, according to Kim et al,3 there is no simple relationship between the age at Fontan surgery or the time since the Fontan operation and the development of HCC. Moreover, it has been shown that “seriously ill” individuals (including those with deoxygenation (oxygen saturation <90%), heart failure, and lymphatic disorders, as well as those who have undergone additional cardiac surgery) may be at the highest risk of developing HCC.3
We present a case of rapid HCC progression in a 19‑year‑old man with hypoplastic left heart syndrome (Figure 1A–1E) and failing Fontan circulation, where adverse factors and limitations of diagnostic methods further contributed to the unfavorable outcome. So far, the patient has undergone several procedures, including a 3‑stage palliation: the Norwood, the hemi‑Fontan, and the Fontan procedures with fenestration and balloon angioplasty. This was followed by stent implantation in the left pulmonary artery, percutaneous embolization of the innominate vein, both internal thoracic arteries, and external thoracic artery, and pacemaker implantation for sick sinus syndrome. He was also diagnosed with elevated pulmonary pressure, protein‑losing enteropathy, chronic leukopenia, hypoproteinemia, severe mixed immunodeficiency syndrome (DiGeorge syndrome and immunodeficiency secondary to enteropathy) requiring subcutaneous immunoglobulin substitution, moderate restrictive ventilation disorders, peptic ulcer disease with a single episode of gastrointestinal bleeding, esophageal varices, chronic occlusion of the right and left subclavian veins and the left internal jugular vein, chronic and massive lymphedema of the right lower extremity as a result of deep vein thrombosis, and lymphangitis (Figure 1B).
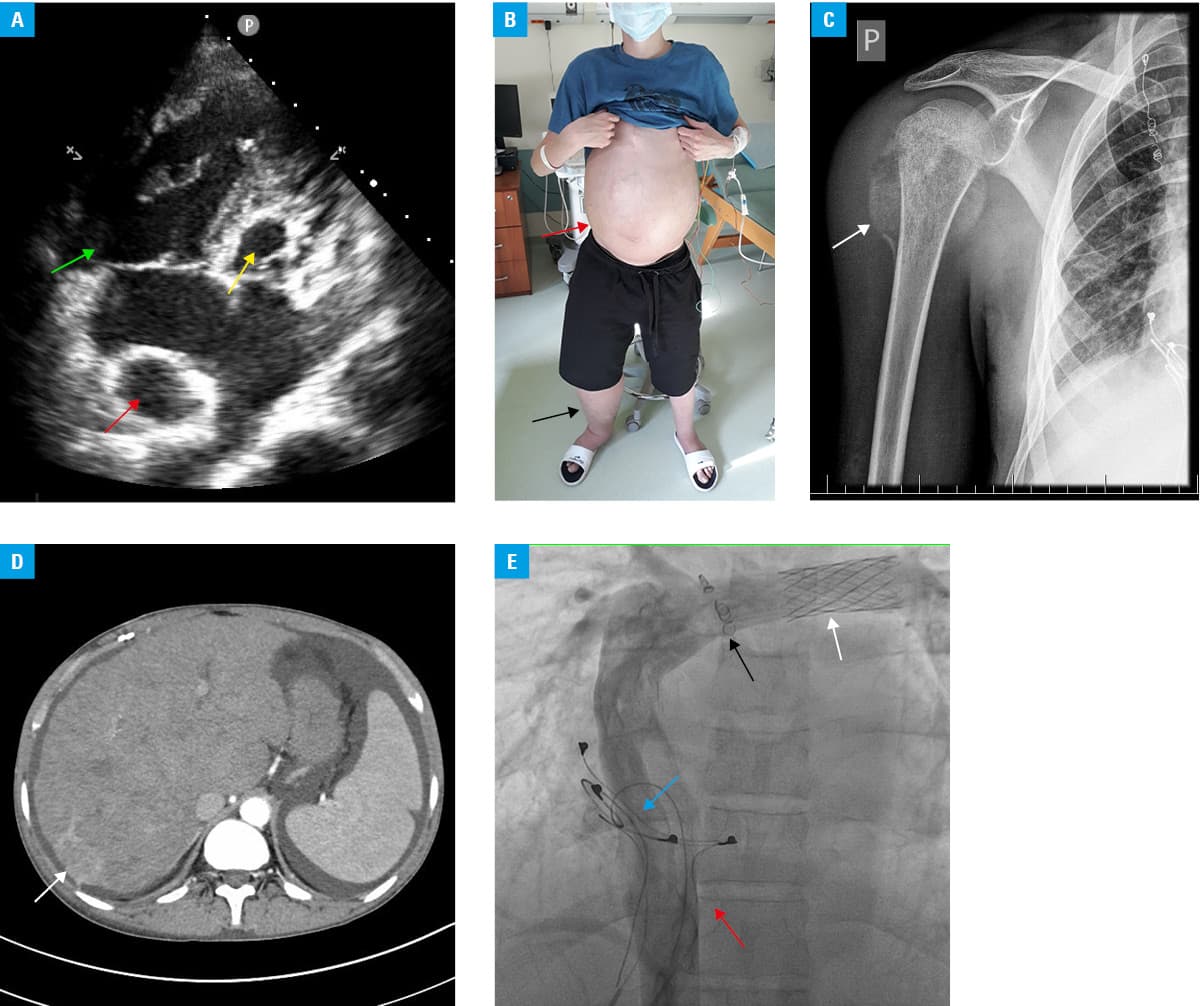
At first evaluation in our center in 2020, the patient was in the New York Heart Association (NYHA) functional class II, without physical signs of circulation failure, and had a resting oxygen saturation of 90%. Echocardiography showed good contractility of the systemic ventricle and no significant atrioventricular valve regurgitation. Laboratory tests showed an increased α-fetoprotein (AFP) level of up to 426 ng/ml (baseline value <7 ng/ml), normal levels of standard liver enzymes, and normal bilirubin fractions. Abdominal ultrasonography with sonoelastography performed by a highly experienced physician showed moderately enlarged liver with stiffness assessed as F3 on the METAVIR scale, without visible focal lesions or peritoneal effusion. Viral hepatitis B and C were excluded.
Urgent follow‑up hospitalization was planned; however, due to the COVID‑19 pandemic and associated restrictions, it was delayed by 6 months. Further diagnostics became possible when the patient contracted COVID‑19, which was accompanied by the worsening of exertional dyspnea to NYHA class III and ascites. Laboratory tests showed an elevated D‑dimer level of 2951 μg/l and a significant increase in AFP level to 5940 ng/ml (baseline value <7 ng/ml), but still normal levels of standard liver enzymes and bilirubin. The patient was diagnosed with pulmonary embolism based on ventilation / perfusion scintigraphy. Abdominal ultrasound showed progression in liver stiffness to class F3 / F4 and severe ascites, but still no focal lesions in the liver. Due to the presence of a pacemaker incompatible with proMRI (Vitatron Holding B.V., Maastricht, The Netherlands), computed tomography (CT) was performed, showing a subcapsular focal lesion in liver segment VII measuring 25 mm × 37 mm × 23 mm, with imaging characteristics typical of HCC. Within a few weeks, the patient noticed a painful tumor of the right humeral head (Figure 1C), which was subsequently partially removed, and histopathology confirmed metastatic cells of HCC.
Multiple consultations in expert centers resulted in the patient’s disqualification from both curative (including heart and liver transplant) and local cancer treatment. He died at the age of 20, within a year of being diagnosed with HCC.
Although most guidelines recommend ultrasound every 6 months as the primary method of screening and monitoring HCC, unfortunately, in our case, it proved ineffective. In turn, an increased AFP concentration may confirm that the simultaneous use of these 2 methods is the right strategy in standard observation (ultrasonography and AFP level check every 6–12 months).1-5 However, when uncertainties arise or additional factors (failing Fontan and other highlighted by Kim et al3) affect an individual’s risk of HCC, we believe that utilizing supplementary methods, including advanced imaging studies (magnetic resonance imaging or / and CT), is essential.3 Unfortunately, the COVID‑19 pandemic and the rapid progression of the disease further reduced both the patient’s and our chances in this challenging battle against HCC.
- Baumgartner H, de Backer J, Babu‑Narayan SV, et al. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J. 2021; 42: 563‑645. | Crossref
- Possner M, Gordon‑Walker T, Egbe AC, et al. Hepatocellular carcinoma and the Fontan circulation: Clinical presentation and outcomes. Int J Cardiol. 2021; 322: 142‑148. | Crossref
- Kim YY, Lluri G, Haeffele C, et al. Hepatocellular carcinoma in survivors after Fontan operation: a case‑control study. Eur Heart J. 2024; 45: 1477‑1480. | Crossref
- Apitz C, Helbing WA, Kaulitz R, et al. Long‑term management of Fontan patients: The importance of a multidisciplinary approach. Front Pediatr. 2022; 10: 886208. | Crossref
- Smaś-Suska M, Skubera M, Wilkosz T, et al. Noninvasive assessment of liver status in adult patients after the Fontan procedure. Pol Arch Intern Med. 2019; 129: 181‑188. | Crossref
ARTICLE INFORMATION