Hybrid ablation with simultaneous right atrial appendage occlusion in a patient with supraventricular tachycardia and post-traumatic scar of the right atrium: an unusual histopathologic finding

 CC BY 4.0
CC BY 4.0
Hybrid ablation with simultaneous right atrial appendage occlusion in a patient with supraventricular tachycardia and post-traumatic scar of the right atrium: an unusual histopathologic finding
A 61‑year‑old man with a history of arterial hypertension and heart failure (ejection fraction, 50%) was previously diagnosed with atrial tachyarrhythmia originating from the anterior region of the right atrium (RA) and the right atrial appendage (RAA) ostium. At anamnesis, he reported to have experienced an injury to the right chest with rib contusion in an industrial accident a few months prior to the diagnosis. He underwent 2 radiofrequency catheter RAA ablations, both circularly‑shaped, at the base and tip of the RAA. Initially, the procedures were successful, with no inducibility of arrhythmia during the early follow‑up. However, during a subsequent electrophysiological study (EPS), a large scar area in the RA was identified as a potential substrate for recurrent atrial tachyarrhythmias or atypical atrial flutters. Despite combined antiarrhythmic therapy, the patient continued to experience severe symptoms, including rapid palpitations, presyncope, and exercise intolerance, which significantly impacted his quality of life. Additionally, he developed episodes of symptomatic sinus bradycardia, which represented the maximum tolerated effect of the combined therapy. After shared decision‑making, the patient was admitted to a cardiac surgery department for a hybrid thoracoscopic ablation under EPS guidance to address the persistent and disabling arrhythmias.
Numerous scars on the lateral wall of the RA and heavily calcified RAA were visualized on thoracoscopy. Ablation of the right pulmonary veins, crista terminalis, Waterstone groove, and ganglionated plexi was followed by cardiac mapping. The arrhythmogenic substrates in the wide scar area in the RAA and the anterior wall of the RA were identified (Figure 1A and 1B). Ablation around the RAA was followed by lines to the superior vena cava and RAA, as in the Maze IV procedure. Additional lines were performed after remapping. The isolation was confirmed. Due to suspicion of arrhythmogenic substrate (detection of a very late atrial signal >250 ms from the onset of the P wave in the RAA), the RAA was occluded with AtriClip Pro2 (40 mm; AtriCure Inc, Manson, Ohio, United States; Figure 1C). Epicardial pacing of the RAA confirmed the exit block. A biopsy at the tip of the RAA wall was taken. The examination showed cardiomyocytes with features of hypertrophy, extensive fibrosis, and a chronic inflammatory infiltrate (Figure 1D–1F). We suspected the association between the chest injury (isolated RA commotio cordis) and RA scarring; however, the cause of the inflammation could not be identified.
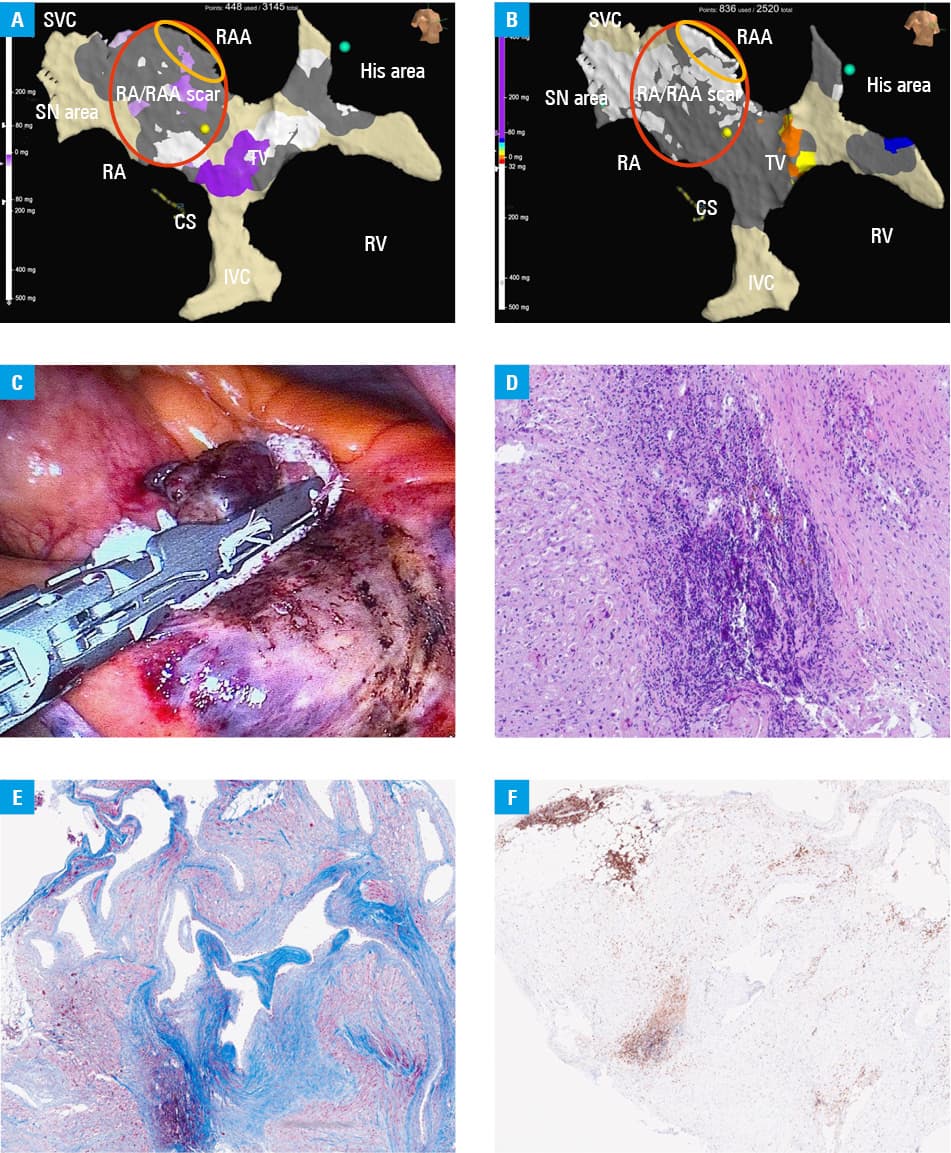
Abbreviations: CS, coronary sinus; IVC, inferior vena cava; RA, right atrium; RAA, right atrial appendage; RV, right ventricle; SN, sinuns node; SVC, superior vena cava; TV, tricuspid valve
No arrhythmia episodes were observed postoperatively. On the fourth day after the surgery, the patient was discharged in good general condition and referred for cardiac rehabilitation. At the 3‑month follow‑up, he maintained normal sinus rhythm and reported no symptoms.
This is the first‑in‑Poland case report on hybrid thoracoscopic ablation with cardiac mapping and simultaneous right atrial appendage occlusion (RAAO) in a patient with RA scar–induced supraventricular tachycardia. Simultaneous cardiac mapping helps identify electrical activity distribution, sinus node activity, and area of very delayed activation within the same chamber.1-4 In this case, the intraoperative macroscopic view of the RA/RAA and histopathologic findings coincided with the arrhythmia site and recurrences of atrial tachycardias or atypical scar‑related atrial flutters. EPS confirmed arrhythmia substrate in the scar region, suggesting that the inflammatory process could be proarrhythmic.5
RAAO is an uncommon procedure. In this case, however, it might be beneficial for the patient in terms of arrhythmia substrate isolation. Although dedicated to left atrial appendage occlusion, Atri Clip Pro2 was a feasible instrument for the procedure.
- Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020;41:655‑720.
- Maesen B, Luermans JGLM, Bidar E, et al. A hybrid approach to complex arrhythmias. Europace. 2021; 23: ii28‑ii33. | Crossref
- Shenasa M, Al‑Ahmad A. Historical perspectives on cardiac mapping and ablation. Card Electrophysiol Clin. 2019; 11: 405‑408. | Crossref
- Kumar S, Baldinger SH, Romero J, et al. Substrate‑based ablation versus ablation guided by activation and entrainment mapping for ventricular tachycardia: a systematic review and meta‑analysis. J Cardiovasc Electrophysiol. 2016; 27: 1437‑1447 | Crossref
- Lewek J, Kaczmarek K, Cygankiewicz I, et al. Inflammation and arrhythmias: potential mechanisms and clinical implications. Expert Rev Cardiovasc Ther. 2014; 12: 1077‑1085. | Crossref
ARTICLE INFORMATION