Echocardiographic features and therapeutic dilemmas in a patient with clinically significant multivalvular disease and left atrial appendage thrombus

 CC BY 4.0
CC BY 4.0
Echocardiographic features and therapeutic dilemmas in a patient with clinically significant multivalvular disease and left atrial appendage thrombus
A 71‑year‑old woman on long‑term treatment with rivaroxaban, with obesity and a history of hypertension, pulmonary embolism, valvular disease, and atrial fibrillation (AF) was admitted for arrhythmia ablation. She complained of progressive exertional dyspnea, weakness, and dizziness. Transthoracic echocardiography showed moderate mitral stenosis (MS; mean gradient [MG], 6 mm Hg; mitral valve area / body surface area [MVA/BSA], 0.7 cm/m2), an enlarged left atrium (LA; Figure 1A), and moderate aortic stenosis (AS) with a low gradient (peak gradient [PG], 16 mm Hg; atrial valve area [AVA]/BSA, 0.65 cm/m2; Figure 1B) due to insufficient filling of the left ventricle (LV). The LV ejection fraction was 55%.
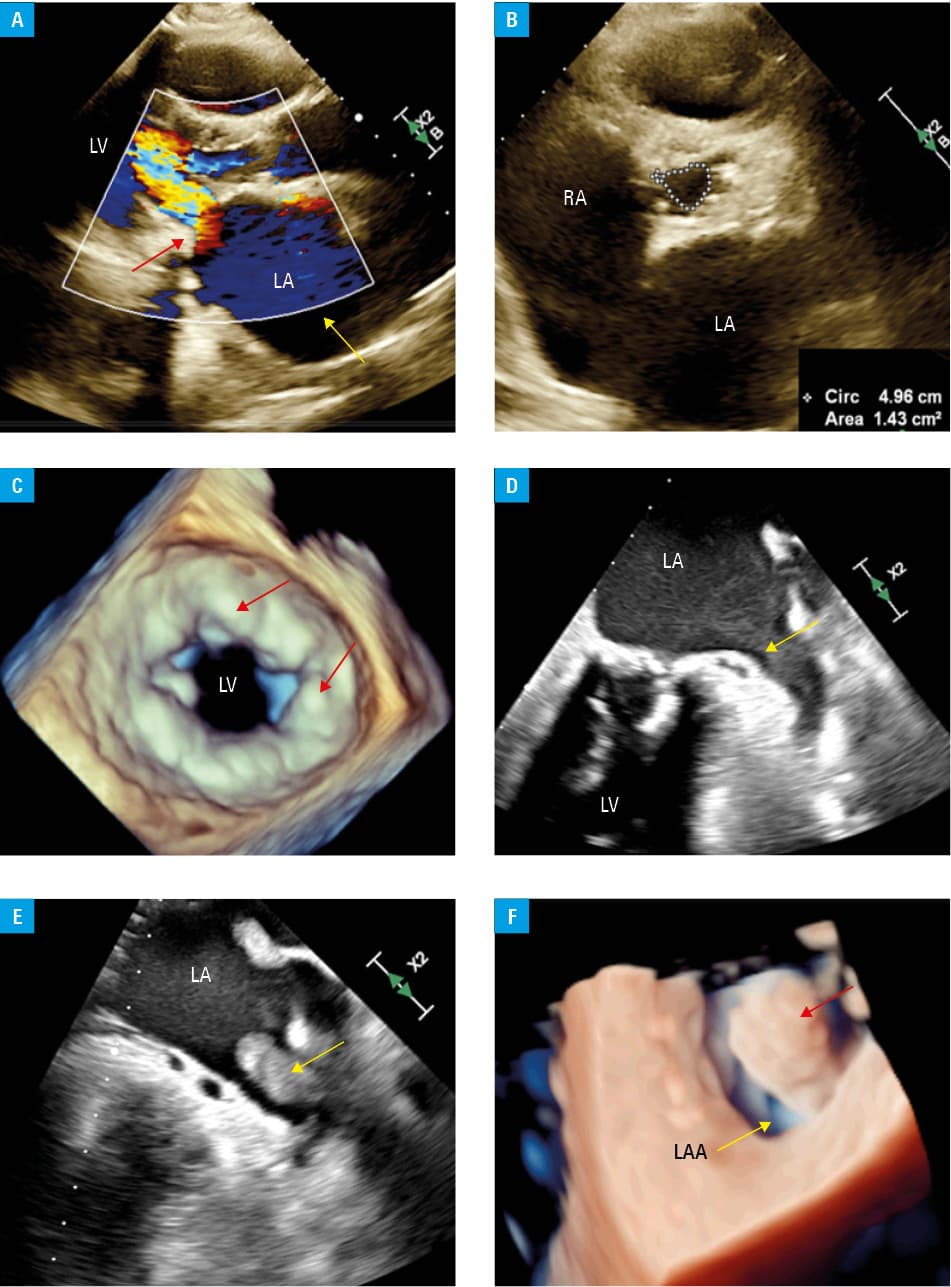
Abbreviations: LA, left atrium; LAA, left atrial appendage; LV, left ventricle; RA, right atrium
Transesophageal echocardiography (TEE) showed massive calcifications of the mitral annulus (Figure 1C) and dense spontaneous echo‑contrast in the left atrial appendage (LAA; Figure 1D). Due to a low emptying velocity (20 cm/s) and a high risk of a thrombus formation at the LAA bottom, ablation was postponed and rivaroxaban was replaced with warfarin. Therapeutic international normalized ratio values were achieved.
Unfortunately, after 3 months, preablation TEE showed a fully formed, more echogenic LAA thrombus, measuring 25 mm × 9.5 mm (Figure 1E and 1F), which indicated ineffective anticoagulation. Warfarin dosage was modified and cardiac surgery consultation was planned. Shortly after discharge, the patient experienced an ischemic stroke, but, fortunately, did not sustain any significant neurologic deficits. Cardiothoracic surgeons assessed her perioperative risk as higher than 10%. The patient is still awaiting the final decision.
In patients with multivalvular left heart disease, both diagnostic and therapeutic problems may arise. The first issue is an increased risk of underestimating the degree of valve defects and the resulting symptoms, which can be misleading.1 Each valve defect should be assessed individually and the interactions between them should always be considered.1
This case confirms that when AS and MS coexist, we observe a reduction in cardiac output greater than in isolated AS, as well as lower‑than‑expected MS and AS gradients.2 Despite these reduced values, the defects remain clinically significant.
The second problem is the consequence of significant MS, including AF, and the associated high risk of thrombus formation. It is worth noting that the presence of LAA thrombus in AF patients, even those on chronic anticoagulation, is possible.3 TEE is clearly the best diagnostic tool for assessing the LAA and excluding or confirming thrombus formation.3,4
In our patient, anticoagulation was initiated due to pulmonary embolism (related to obesity, without other causes of hypercoagulability) and continued after AF was detected. Then, rivaroxaban therapy was changed to warfarin, as recommended for moderate MS cases,4 but follow‑up TEE showed a large thrombus in the LAA. According to data from the LATTEE registry (Left Atrial Thrombus on Transesophageal Echocardiography)3, the risk of LAA thrombus formation is higher in AF patients on vitamin K antagonist therapy than direct oral anticoagulants (DOACs).3 Interestingly, Kim et al5 presented an analysis with promising results for the use of DOACs in patients with MS and AF, but these findings need confirmation in randomized trials.
Since AF ablation was impossible, the patient was referred to a cardiac surgery department for valve surgery preparation. However, this also poses a dilemma because of the high estimated perioperative risk, and the decision has not yet been made.
Our case highlights the importance of correct echocardiography interpretation and difficulties in preventing stroke in the left heart multivalvular disease.
- Vahanian A, Beyersdorf F, Praz F, et al; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022; 43: 561‑632. | Crossref
- Berti S, Bonanni M, D’agostino A, et al. Treatment of multiple valve disease: surgery, structural intervention, or both? Eur Heart J Suppl. 2023; 25 (Suppl B): B21‑B24. | Crossref
- Kapłon‑Cieślicka A, Gawałko M, Budnik M, et al. Left atrial thrombus in atrial fibrillation / flutter patients in relation to anticoagulation strategy: LATTEE registry. J Clin Med. 2022; 11: 2705.
- Van Gelder IC, Rienstra M, Bunting KV, et al; ESC Scientific Document Group. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio‑Thoracic Surgery (EACTS). Eur Heart J. 2024; 45: 3314‑3414.
- Kim JY, Kim SH, Myong JP, et al. Outcomes of direct oral anticoagulants in patients with mitral stenosis. J Am Coll Cardiol. 2019; 73: 1123‑1131. | Crossref
ARTICLE INFORMATION