A 45‑year‑old man was admitted to a hospital for dyspnea and chronic productive cough. Since childhood, he has had hyperkeratotic lymphatic malformation on the skin and bone cysts associated with left leg hypotrophy. At the age of 8 years he underwent subclavian flap aortoplasty due to aortic coarctation. At the age of 23 he was hospitalized for cardiac tamponade. Video‑assisted pericardioscopy was performed, resulting in drainage of 1000 ml of chylous fluid. Cytological analysis confirmed the presence of lymphocytes and numerous fat droplets. Thoracic computed tomography showed ground‑glass opacities with random distribution. Massive amounts of chylous sputum, with casts of the bronchial tree, were evacuated during bronchoscopy. Lymphoscintigraphy disclosed 2 contrast‑accumulating lesions in the upper mediastinum. The patient’s congenital defects are summarized in Figure 1A. A diagnosis of generalized lymphatic anomaly (GLA) with chylous pulmonary edema was established. The patient was treated with therapeutic bronchoscopies. Due to dyspnea at night and transient nocturnal desaturation, home oxygen therapy during sleep was introduced.
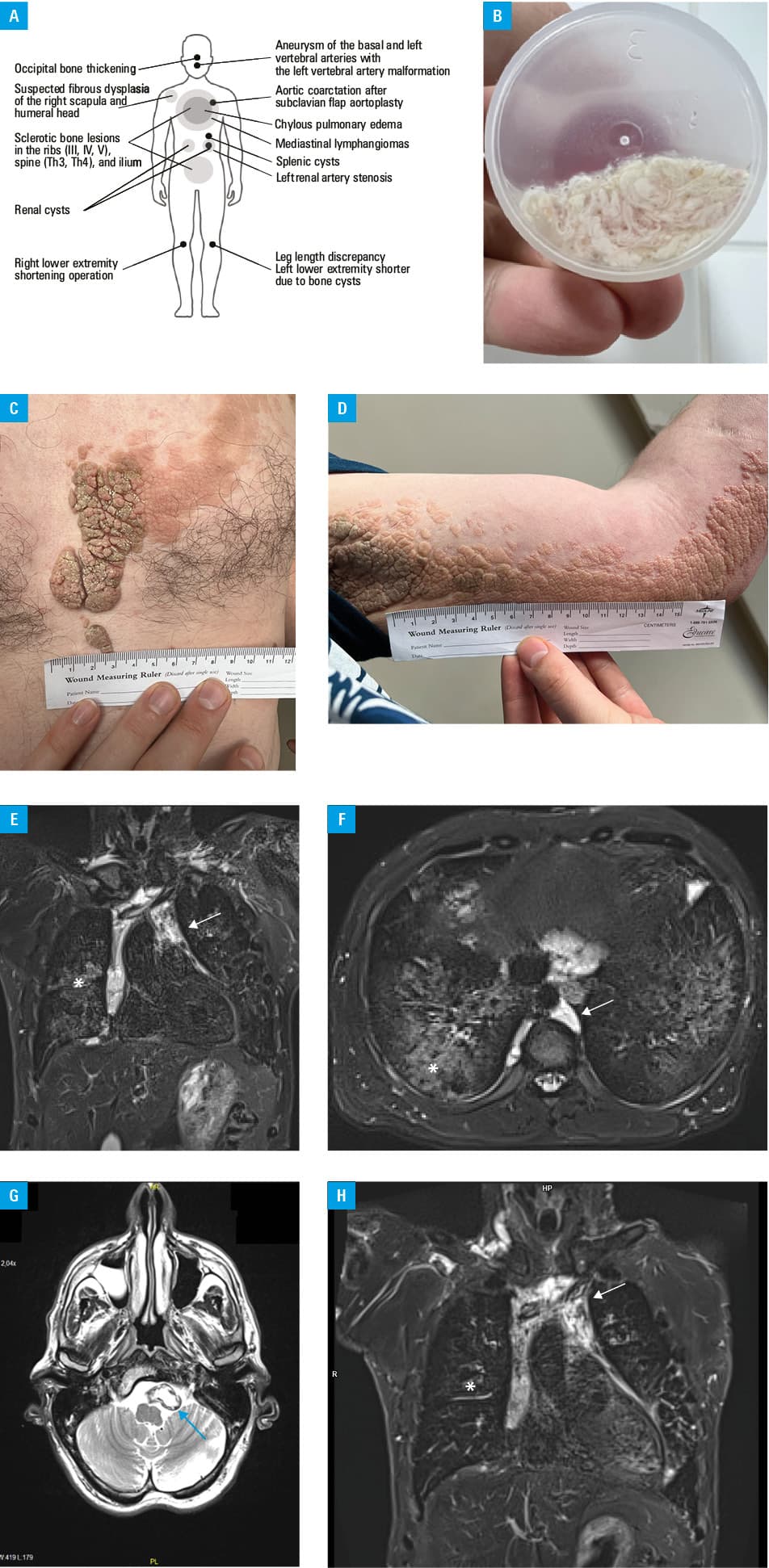
On the present admission, the patient complained of chronic productive cough with expectoration of chylous sputum. The sputum contained triglycerides (>1170 mg/dl; reference range [RR] <150 mg/dl) and cholesterol (66.6 mg/dl; RR <190 mg/dl; Figure 1B); serum levels of cholesterol and triglycerides were 191.5 mg/dl and 155.3 mg/dl, respectively. Examination showed 2 large lymphatic malformations on the skin (Figure 1C and 1D; Supplementary material, Figure S1A–S1C), an irregular bony structure over the occipital protuberance (Supplementary material, Figure S1D), and bilateral crackles at the lung bases. D‑dimer and fibrinogen levels were within normal ranges. Chylous pulmonary edema and 2 mediastinal lymphatic malformations, located anteriorly (13.19 cm × 7.19 cm) and posteriorly, were visualized on magnetic resonance imaging (MRI; Figure 1E and 1F). Spirometry results showed forced expiratory volume in 1 second at 94% of predicted volume (%pred) and forced vital capacity at 96%pred, while plethysmography confirmed total lung capacity at 99%pred and residual volume at 102%pred. Lung diffusion capacity was mildly impaired (73%pred; Z score, –1.91). Head MRI showed aneurysm of the basilar and left vertebral arteries, with left vertebral artery malformation (Figure 1G; Supplementary material, Figure S1E–S1H). Echocardiography results were unremarkable.
The diagnosis of GLA was confirmed. Treatment with sirolimus was initiated, leading to significant improvement in chylous sputum production, partial regression of chylous edema on MRI (Figure 1H; Supplementary material, Figure S1I and S1J), and normalization of saturation during sleep.
Complex lymphatic anomalies (CLAs) are rare multiorgan diseases with diverse, overlapping clinical findings that make an accurate diagnosis challenging. They are caused by pathological proliferation of lymphatic vessels associated with genetic abnormalities in the phosphoinositide 3‑kinase (PI3K) / mammalian target of rapamycin (mTOR) and rat sarcoma virus (RAS) / mitogen‑activated protein kinase (MAPK) signaling pathways. GLA is a type of CLA related to mutations in the latter pathway, and can involve various organs, such as the lungs, spleen, bones, mediastinum, and soft tissues. It can be associated with chylous collections in the pleura, pericardium, and peritoneum, mediastinal and retroperitoneal lymphangiomas, multiple cystic splenic lesions, gastrointestinal hemorrhage, multiple bone osteolysis, lymphedema, and skin involvement. The PIK3 / protein kinase B (Akt) / mTOR pathway plays a crucial role in the development of blood vessels and lymphatic tissues.1,2 Several studies reported responses to sirolimus inhibition, including improvements in radiological findings, functional impairment scores, and quality of life.3,4 Most patients experience side effects of treatment, predominantly mild.5
Our patient presented a unique set of congenital abnormalities, warranting only a provisional diagnosis of GLA. The effects of sirolimus on his vascular abnormalities indicate a positive response to such therapy in patients with CLA.
- Bouwman FCM, Verhoeven BH, Klein WM, et al. Congenital vascular malformations in children: from historical perspective to a multidisciplinary approach in the modern era – a comprehensive review. Children. 2024; 11: 567. | Crossref
- Kane G, Fernandez‑Pineda I. Targeted therapies for vascular malformations. Front Med. 2024; 11: 1446046. | Crossref
- Ozeki M, Fukao T. Generalized lymphatic anomaly and Gorham‑stout disease: overview and recent insights. Adv Wound Care (New Rochelle). 2019; 8: 230‑245. | Crossref
- Maruani A, Tavernier E, Boccara O, et al. Sirolimus (rapamycin) for slow‑flow malformations in children: the observational‑phase randomized clinical PERFORMUS trial. JAMA Dermatol. 2021; 11: 1289‑1298. | Crossref
- Dompmartin A, Baselga E, Boon LM, et al. The VASCERN‑VASCA Working Group diagnostic and management pathways for venous malformations. J Vasc Anom. 2023; 4: e064. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION