Misleading diagnosis of ST-segment elevation myocardial infarction in a patient receiving 5-fluorouracil

 CC BY 4.0
CC BY 4.0
Misleading diagnosis of ST-segment elevation myocardial infarction in a patient receiving 5-fluorouracil
A 65‑year‑old man with a history of surgically treated pancreatic ductal adenocarcinoma presented to a cardiology department with severe retrosternal chest pain lasting for 2 hours. The day before, he had received his first cycle of mFOLFIRINOX chemotherapy (5‑fluorouracil [5‑FU], leucovorin, irinotecan, and oxaliplatin) as adjuvant therapy, with an uneventful administration. Due to ST‑segment elevation in the leads V3–V6 and persistent symptoms, immediate coronary angiography was performed (Figure 1A). It showed significant stenosis of the mid‑left anterior descending artery (LAD) and borderline lesions in both the circumflex (Cx) and right coronary arteries (RCA). Following predilatation, a 4 mm × 20 mm everolimus‑eluting stent was successfully deployed at 16 atmospheres in the LAD and postdilated with a 4.5 mm × 15 mm noncompliant balloon catheter at 18–20 atmospheres, resulting in symptom resolution (Figure 1B). Echocardiography demonstrated reduced left ventricular ejection fraction of 40% with hypokinesis of the basal segments of the inferior, posterior, and lateral walls. The level of troponin I was marginally elevated at 0.147 ng/ml (reference range, 0.058 ng/ml). The patient was managed conservatively and discharged after 2 days.
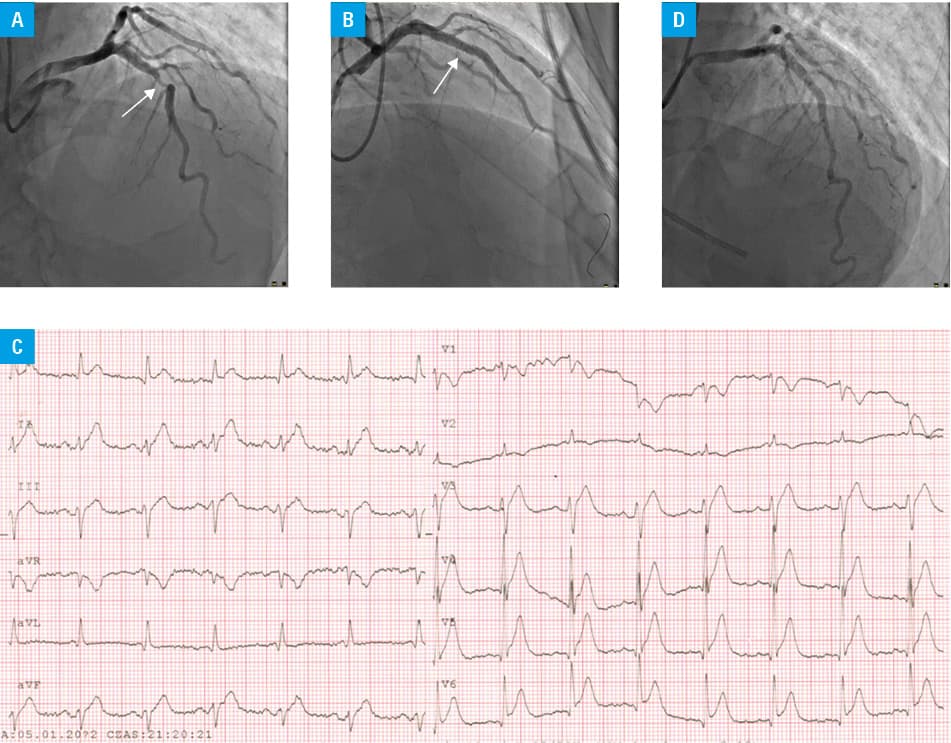
Four weeks later, emergency services transported the patient with suspected recurrent ST‑segment elevation. Electrocardiogram showed transient ST‑segment elevation in the leads V4–V6 (Figure 1C), although no new wall motion abnormalities were visualized on echocardiography. Antiplatelet medication compliance was confirmed. Notably, this episode occurred hours after completing the second chemotherapy cycle (80% dose of mFOLFIRINOX). Persistent chest pain prompted repeat coronary angiography, which demonstrated a patent LAD stent with complete distal flow (Figure 1D) and findings consistent with the previous study. Fractional flow reserve (FFR) and instantaneous wave‑free ratio (iFR) measurements excluded significant stenosis in the Cx and RCA. Despite abnormal values for the LAD (FFR, 0.62; iFR, 0.71) suggesting significant ischemia, no culprit lesions were identified on angiography or a pullback iFR. The clinical presentation was attributed to chemotherapy‑induced coronary vasospasm and / or microvascular dysfunction, with symptoms resolving after nitroglycerin administration. Peak troponin I level reached 0.141 ng/ml. Anemia due to bone marrow suppression and acute kidney injury were excluded. Treatment with isosorbide mononitrate and diltiazem was initiated, with no subsequent symptom recurrence. Following interdisciplinary consultation between cardiology and oncology specialists, outpatient rechallenge with 5‑FU–based therapy was planned.
Our case demonstrates the cardiovascular risks associated with 5‑FU–based chemotherapy regimens, particularly highlighting how coronary vasospasm can mimic acute coronary syndrome.1-4 The clear temporal relationship between chemotherapy administration and cardiac events strongly indicates 5‑FU–induced cardiotoxicity, an established but frequently underrecognized complication. This cardiotoxicity has multiple underlying mechanisms, including endothelial damage, coronary vasospasm, oxidative stress, and thrombogenic effects, with clinical manifestations ranging from subtle electrocardiography changes to acute coronary syndrome, cardiogenic shock, and sudden cardiac death.2,3 While significant LAD stenosis guided our initial decision on coronary intervention, the subsequent vasospastic episodes revealed a more complex pathophysiology.2,3 Notably, the discrepancy between FFR/iFR measurements and angiographic findings during follow‑up underscores the intricate coronary physiology associated with chemotherapy‑induced vascular dysfunction.5 This complication can occur independently of underlying coronary artery disease, emphasizing the need for interventional cardiologists to maintain high awareness of chemotherapy‑related cardiotoxicity.1-3 Success in managing such cases critically relies on strict cardiologist‑oncologist collaboration.
- Klotzka A, Iwańczyk S, Ropacka‑Lesiak M, et al. Anthracycline‑induced microcirculation disorders: AIM PILOT Study. Kardiol Pol. 2023; 81: 766‑768. | Crossref
- Aleksova A, Gagno G, Pierri A, et al. What the cardiologist needs to consider in the management of oncologic patients with STEMI‑like syndrome: a case report and literature review. Pharmaceuticals (Basel). 2021; 14: 563. | Crossref
- Padegimas A, Carver JR. How to diagnose and manage patients with fluoropyrimidine‑induced chest pain: a single center approach. JACC CardioOncol. 2020; 2: 650‑654. | Crossref
- Balaji N, Dixit P, Adams AM, et al. ST‑segment elevation myocardial infarction caused by 5‑fluorouracil‑related cardiotoxicity. Cureus. 2024; 16: e52864. | Crossref
- Figura E, Zaremba M, Rogula S, et al. Coronary slow flow and microvascular spasm as an underrecognized cause of chest pain. Adv Interv Cardiol. 2023; 19: 289‑291. | Crossref
ARTICLE INFORMATION