Placebo-adjusted effect of the initial estimated glomerular filtration rate decline following sodium-glucose cotransporter 2 inhibitor initiation: a systematic review and meta-analysis
Key words: chronic kidney disease, diabetes, estimated glomerular filtration rate dip, heart failure, sodium-glucose cotransporter 2 inhibitor

 CC BY 4.0
CC BY 4.0
Placebo-adjusted effect of the initial estimated glomerular filtration rate decline following sodium-glucose cotransporter 2 inhibitor initiation: a systematic review and meta-analysis
Introduction: Sodium‑glucose cotransporter 2 inhibitors (SGLT‑2is) are pivotal in managing heart failure, chronic kidney disease, and type 2 diabetes mellitus. While their beneficial impact is well established, the effects of the initial decline in estimated glomerular filtration rate (eGFR) at the start of SGLT‑2i therapy are poorly understood.
Objectives: The study aimed to assess the impact of the initial eGFR dip on prognosis in the abovementioned conditions.
Patients and methods: We systematically searched several databases to identify studies analyzing the effect of the initial eGFR dip following the initiation of an SGLT‑2i on selected outcomes. Randomized controlled trials (RCTs) were included, and a backward snowballing method was applied. The analysis was conducted according to the PRISMA guidelines and registered in PROSPERO (CRD42024527609).
Results: Out of 2422 papers screened, 14 passed the initial screening, and 5 were included in the quantitative analysis. The dip status was reported for all participants (n = 23 890), with the dip occurring in 13 575 patients (56.82%; 8245 [34.51%] in the intervention arm and 5330 [22.31%] in the placebo arm). In the patients allocated to receive SGLT2is, the initial eGFR dip, regardless of its magnitude, was not linked to an increased risk of adverse kidney outcomes, cardiovascular composite end point, cardiovascular mortality (hazard ratio [HR], 0.85; 95% CI, 0.65–1.11; P = 0.24), or all‑cause mortality (HR, 0.9; 95% CI, 0.7–1.15; P = 0.4). In contrast, in the placebo group, the dip was associated with a worse prognosis for the cardiovascular composite end point (HR, 1.35; 95% CI, 1.19–1.52; P <0.001). The use of an SGLT‐2i, as compared with placebo, was associated with a positive effect on the cardiovascular composite end point in the dip range of 0%–1.1% to 10%–11.8% (risk difference [RD], –0.04; 95% CI, –0.07 to –0.01; P = 0.006) and greater than 10%–11.8% (RD, –0.04; 95% CI, –0.06 to –0.02; P <0.001), but not if the dip exceeded 25%–30% (RD, –0.06; 95% CI, –0.13 to 0.02; P = 0.12).
Conclusions: Unlike in the placebo arms of RCTs, where an eGFR dip was associated with unfavorable outcomes, the early eGFR dip in the patients receiving SGLT‑2is was either neutral or beneficial. The SGLT‑2i–related eGFR dip appears to confer a particularly favorable effect in the population with heart failure with reduced ejection fraction. Mild SGLT‑2i–related eGFR dip (reduction by ≤11.8%) correlated with improved cardiovascular outcomes, while larger reductions did not negatively impact patient prognosis.
What's new?
This meta‑analysis is the first to systematically assess the clinical significance of the initial decline in estimated glomerular filtration rate (eGFR) following sodium‑glucose cotransporter 2 inhibitor (SGLT‑2i) initiation. Contrary to previous concerns, our findings suggest a trend toward this early decline being a benign and potentially favorable phenomenon, particularly in patients with heart failure with reduced ejection fraction. A mild eGFR dip (reduction by up to 11.8%) correlated with improved cardiovascular outcomes, while larger reductions did not negatively impact patient prognosis. These findings reassure clinicians regarding the implications of an eGFR dip in SGLT‑2i therapy and emphasize the importance of early monitoring for optimal patient management.

Introduction
Sodium‑glucose cotransporter 2 inhibitors (SGLT‑2is) have become crucial in the management of heart failure (HF), type 2 diabetes mellitus (T2DM), and chronic kidney disease (CKD), as outlined in the latest guidelines.1-4 This drug class has demonstrated a beneficial impact on prognosis across these patient populations, particularly regarding cardiovascular and kidney composite outcomes, as well as all‑cause mortality.5-9 A common yet not fully understood phenomenon associated with SGLT‑2is is the initial decline in estimated glomerular filtration rate (eGFR), which occurs in 28% to 45% of patients after the start of the therapy.10 Furthermore, evidence suggests that this initial eGFR dip (in the patients on SGLT‑2is, unlike in those receiving placebo) may not be associated with an increased risk of kidney injury, and might even predict a favorable outcome. Understanding the clinical significance and pathophysiological origins of this initial eGFR decline, along with its impact on patient prognosis, is essential for appropriate monitoring and management of treatment. Moreover, broader implementation of SGLT‑2i therapy may yield significant health benefits on the population level, as demonstrated in recent estimations for the Polish population, highlighting the potential of these agents to improve cardiovascular and renal outcomes on a larger scale.11 Due to the scarcity of compelling data in this area, we conducted a meta‑analysis to evaluate the impact of the initial eGFR dip on prognosis in each of the 3 abovementioned patient populations (HF, CKD, and T2DM).
Patients and methods
Eligibility criteria
The inclusion criteria for this systematic review and meta‑analysis comprised studies evaluating patients treated with SGLT‑2is, comparing outcomes between cohorts exhibiting an initial decline in eGFR and those without such a decline. Indications for initiating SGLT‑2i therapy included HF, CKD, and T2DM. Only randomized controlled studies (RCTs) were eligible for inclusion. The studies were required to assess at least 1 of the following predefined outcomes or a composite thereof: all‑cause mortality, cardiovascular mortality, all‑cause hospitalization, cardiovascular hospitalization, hospitalization for HF, emergency visits for HF, quality of life, and renal outcomes, such as sustained reduction in eGFR, a need for renal replacement therapy, or kidney transplant. Case reports, case series, animal studies, review articles, nonrandomized studies, and studies involving pediatric populations were excluded. The analysis was performed according to the PRISMA guidelines12 and registered in PROSPERO (CRD42024527609).
Search strategy and information sources
The following databases were systematically searched: Medline, Embase, Academic Search Ultimate, Health Source: Nursing / Academic Edition, Health Source: Consumer Edition, ERIC, Cochrane Library, and ClinicalTrials.gov. The search was performed on January 24, 2024, and employed key words are detailed in Supplementary material, Methods. Two investigators (WT and MG) independently reviewed the titles of the articles extracted from the databases. Any contentious issues were resolved through discussion. Following the initial title screening, a backward snowballing technique was applied, which involved analyzing the references of the retrieved articles and citing selected papers to identify additional relevant publications. Editorials identified as relevant were also included in the screening process.10,13
Data collection process
Data extraction was conducted by 2 independent reviewers (MF and OS). The extracted data included: year of publication, number of participants (only those in the SGLT‑2i arm were included), the proportion of male participants, mean age, indication for SGLT‑2i initiation, specific SGLT‑2i analyzed, study design (observational or RCT), definition of the dip (in percentage), timing of dip assessment, duration of follow‑up, and analyzed outcomes.
Risk of bias and certainty of evidence assessment
The Risk of Bias 2 (RoB 2) tools were utilized to assess the risk of bias in the included studies.14 Two investigators (KF and JP) conducted these assessments. A study was categorized as having a low risk of bias if it was evaluated as low‑risk across all domains. The quality of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework.15 The GradePRO GDT software (developed by McMaster University and Evidence Prime Inc., Hamilton, Canada) was employed to generate a summary of findings Table and assess the certainty of evidence.
Statistical analysis
A generic variance analysis with a random effects model was employed to pool the hazard ratios (HRs) obtained from different studies, while a fixed effect model was used to combine data from the same study. The pooled HR, along with its 95% CI, was calculated. Whenever available, adjusted HRs were prioritized over crude ratios. Due to the limited number of studies providing data, similar composite end points—such as renal or cardiovascular composites—were pooled, despite minor variations in their definitions across studies. A summary of differences in the composite end point definitions is provided in Table 1. The incidence of the dip in both the intervention and placebo arms was pooled using the risk difference (RD). Additionally, a pooled analysis of the effect of the dip was separately performed in the intervention and placebo arms (Supplementary material, Figure S1) based on the crude number of patients with events. A pooled analysis comparing the effect of dip vs nondip, using HRs in the intervention arm only, was also carried out. Furthermore, we analyzed the differences in outcomes between the intervention and placebo arms within the group experiencing the dip, based on the crude number of events and RD. Heterogeneity was evaluated using the I2 statistic, with values between 50% and 60% considered indicative of moderate or substantial heterogeneity, depending on overlapping 95% CIs and the P value in the χ2 test. An I2 greater than 60% was considered to indicate substantial heterogeneity. Subgroup analyses were conducted to evaluate the impact of different dip values. Additionally, we assessed the effect of the dip in specific HF populations, including the general HF population, HF with reduced ejection fraction (HFrEF), and HF with preserved EF (HFpEF), as these were the only diagnoses found in more than 1 study. Due to the limited number of studies, funnel plots were not constructed. Statistical analyses were performed using Review Manager, version 5.4.1 (The Cochrane Collaboration, London, United Kingdom). A P value below 0.05 was deemed significant.
Composite end point | DAPA‑CKD18 | DAPA‑HF17 | DELIVER16 | EMPEROR‑Reduced20 | EMPEROR‑Preserved19 |
Abbreviations: DAPA, dapagliflozin; eGFR, estimated glomerular filtration rate; ESKD, end‑stage kidney disease; HF, heart failure; HHF, hypertensive heart failure | |||||
Kidney composite end point | Sustained ≥50% decline in eGFR, onset of ESKD or renal death | Sustained ≥50% decline in eGFR, ESKD or renal death | ≥50% decline in eGFR relative to the month 1 value; ESKD or death due to kidney causes | Need for chronic dialysis or renal transplant or a sustained ≥40% decrease in eGFR or a sustained eGFR <15 ml/min/1.73 m2 (if the baseline eGFR was ≥30 ml/min/1.73 m2) or <10 ml/min/1.73 m2 (if the baseline eGFR was <30 ml/min/1.73 m2) | Time to the first occurrence of chronic dialysis; renal transplant; sustained eGFR reduction ≥40%; or sustained eGFR <15 ml/min/1.73 m2 (if the baseline eGFR ≥30 ml/min/1.73 m2) or <10 ml/min/1.73 m2 (if the baseline eGFR <30 ml/min/1.73 m2) |
Cardiovascular composite end point | Cardiovascular death or HHF | HHF or urgent visit for HF requiring intravenous therapy or cardiovascular death | Cardiovascular death or a worsening HF event (hospitalization or urgent visit) | Cardiovascular death or HHF | Cardiovascular death or HHF |
Ethics
Due to the design of this study (meta‑analysis), approval from an institutional review board or ethics committee, or consent from individual study participants, was not required. No new data were collected, and all data utilized were publicly available from previously published studies.
Results
Search process
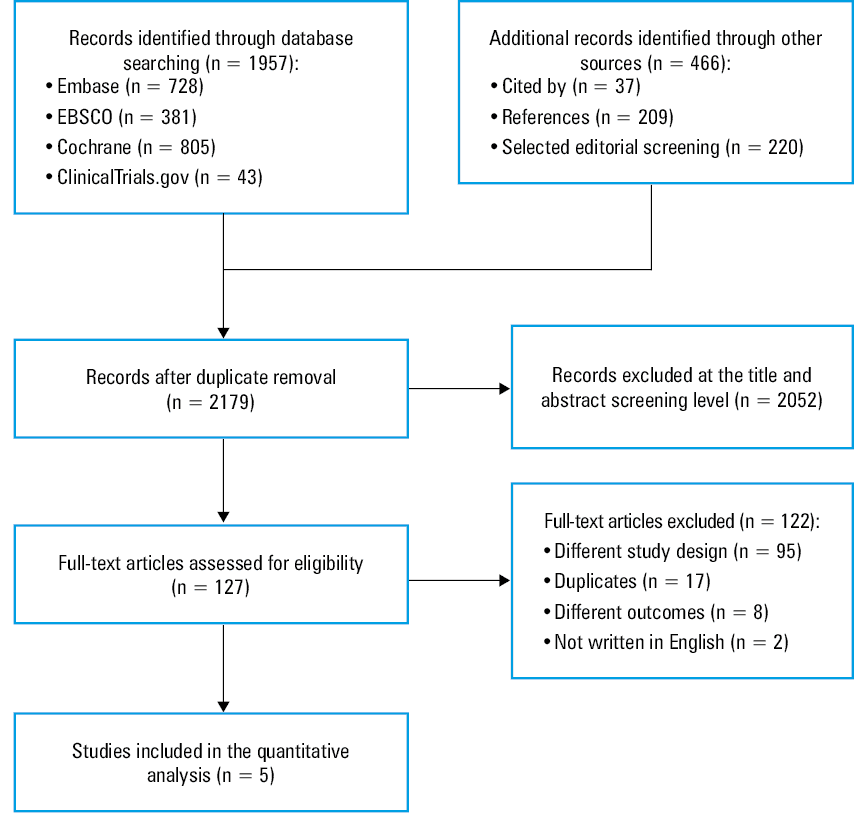
Initially, a total of 1957 studies were identified, with an additional 466 sourced through backward snowballing. The screening process flowchart is outlined in Figure 1. Ultimately, 14 studies met the inclusion criteria but only 5 were used in the quantitative analysis.16-20 Nine studies were excluded due to an absence of the desired outcome or data unavailability.21-28
Study characteristics
Characteristics of the included studies are presented in Table 2. The studies involved a total of 11 949 patients treated with SGLT‑2is. Of the 5 studies included, 4 focused on HF populations, and 1 addressed CKD. Dapagliflozin was investigated in 3 studies, while 2 examined empagliflozin. All studies were RCTs. The publication dates ranged from 2022 to 2024.
Author | Acronym | Year of publication | Study design | Sample size | Dip vs nondip, n (%) | Men, n, (%) | Mean age, y | Indication for SGLT‑2i initiation | Analyzed SGLT‑2i | Dip definition, % | Time point of dip assesment, mo | Duration of follow‑up, mo | Analyzed outcomes | Mean values of an acute dip (ml/min/1.73 m2) |
Abbreviations: ACM, all‑cause mortality; CKD, chronic kidney disease; CV, cardiovascular; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; RCT, randomized controlled trial; SGLT‑2i, sodium‑glucose cotransporter 2 inhibitor; others, see Table 1 | ||||||||||||||
Causland et al16 | DELIVER | 2024 | RCT | 2892 | 1144 (39.56) vs 1748 (60.44) | 1627 (56) | 72 | HFpEF, HFmrEF | Dapagliflozin | eGFR decline, >10%, >25% | 1 | 36 | Kidney composite, CV composite, ACM | SGLT‑2i, −4; placebo, −1 |
Jongs et al18 | DAPA‑CKD | 2022 | RCT | 2075 | 1627 (78.41) vs 448 (21.59) | 1391 (67) | 61.6 | CKD | Dapagliflozin | eGFR decline, 0%–10%; >10% | 0.5 | Median, 28 | Kidney composite, CV composite, ACM | SGLT‑2i, −4; placebo, −0.8 |
Zannad et al20 | EMPEROR‑Reduced | 2022 | RCT | 1782 | 1172 (65.77) vs 610 (34.23) | 1426 (76.54) | 67.2 | HFrEF | Empagliflozin | eGFR decline, ≤–11.4% (tertile 1), –11.4% to –1% (tertile 2), ≥0% (tertile 3) | 1 | Median, 16 | Kidney composite, CV composite, CV death, ACM | SGLT‑2i, −3.5; placebo, −1 |
Adamson et al17 | DAPA‑HF | 2022 | RCT | 2309 | 882 (38.2) vs 1427 (61.8) | 1761 (76) | 66.2 | HFrEF | Dapagliflozin | eGFR decline, >10%; ≤10% | 0.5 | Range, 4–24 | CV composite, CV death, ACM | SGLT‑2i, −4.2; placebo, −1.1 |
Rastogi et al19 | EMPEROR‑Preserved | 2024 | RCT | 2893 | 1928 (66.6) vs 965 (33.4) | 1609 (55.62) | 71.8 | HFpEF | Empagliflozin | eGFR decline, ≤–11.8% (tertile 1), –11.8% to –1.1% (tertile 2), ≥ –1.1% (tertile 3) | 1 | Median, 26.2 | CV composite, kidney composite, CV death, ACM | SGLT‑2i, −3.7; placebo, −0.5 |
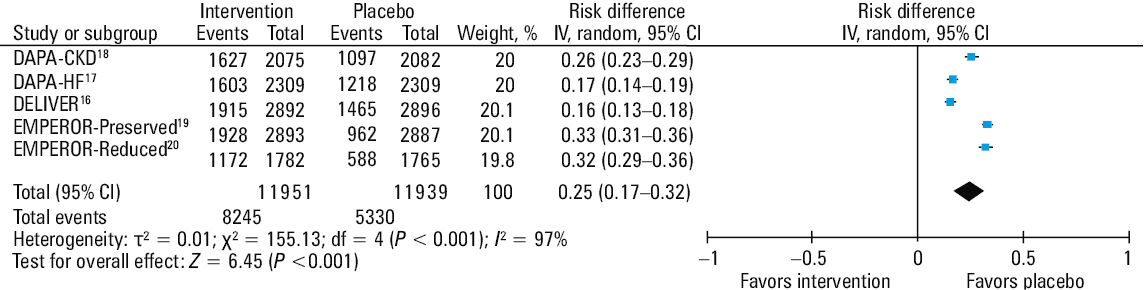
The average age of the participants was 68.3 years, and 7814 were men (65.38%). The dip status was reported for all 11 949 patients, with the dip occurring in 8245 individuals (68.99%). The definitions of the dip, the observed period during which the dip occurred, and the follow‑up duration varied slightly between the studies. The incidence of the dip was pooled, and the relative risk of the dip was found to be lower in the placebo arm, with an RD of 0.25 (95% CI, 0.17–0.32; Figure 2).
Abbreviations: df, degree of freedom; HF, heart failure, IV, inverse variance; others, see Tables 1 and 2
Outcomes
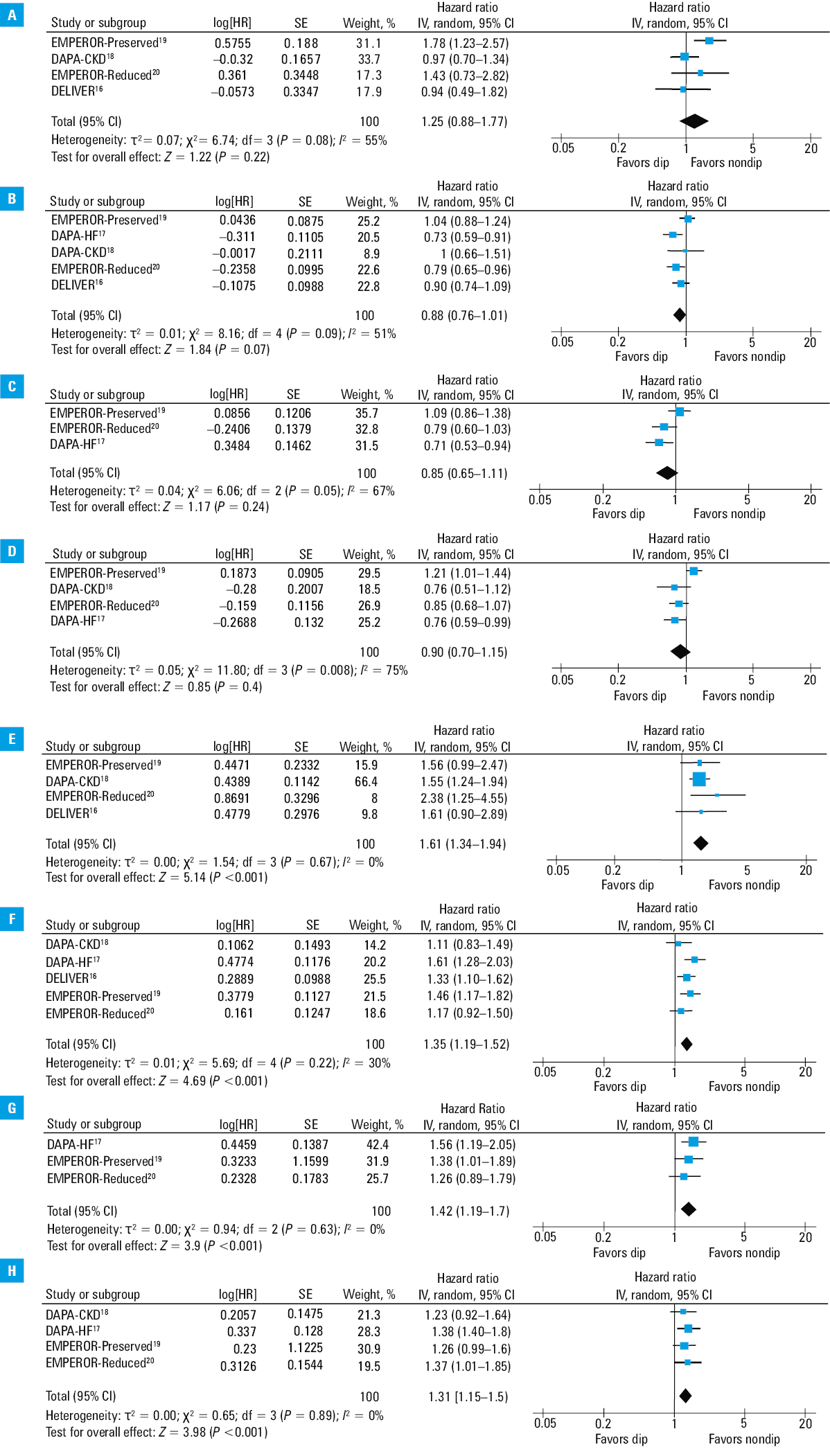
The 4 outcomes analyzed included cardiovascular composite, kidney composite, cardiovascular mortality, and all‑cause mortality, each examined in at least 2 studies. A summary of these outcomes is provided in Table 3. The forest plots depicting the analyzed outcomes are shown in Figure 3. The merged effect for the selected outcomes in individual studies, covering different dip ranges, and the results of subgroup analyses are detailed in Supplementary material, Figures S2–S5. Some studies did not report the exact number of patients with events. Consequently, these studies were excluded from our results report to avoid skewing the percentages but the HRs reported therein were pooled. Additionally, in some studies, the number of enrolled patients that was initially reported decreased when reporting the dip frequency and outcomes, likely due to patient loss to follow‑up, among other reasons.
Author | Acronym | CV composite | Kidney composite | CV mortality | All‑cause mortality |
Data are presented as hazard ratios (95% CIs).
| |||||
Causland et al16 | DELIVER | 0.9 (0.74–1.09) | 0.94 (0.49–1.92) | NR | NR |
Jongs et al18 | DAPA‑CKD | 1.00 (0.66–1.51) | 0.97 (0.7–1.34) | NR | 0.76 (0.51–1.21) |
Zannad et al20 | EMPEROR‑Reduced | 0.79 (0.65–0.96) | 1.43 (0.73–2.82) | 0.79 (0.6–1.03) | 0.85 (0.68–1.07) |
Adamson et al17 | DAPA‑HF | 0.73 (0.59–0.91) | NR | 0.71 (0.53–0.94) | 0.76 (0.59–0.99) |
Rastogi et al19 | EMPEROR‑Preserved | 1.04 (0.88–1.24) | 1.78 (1.23–2.57) | 1.09 (0.86–1.38) | 1.21 (1.01–1.44) |
Cardiovascular composite end point
The occurrence of the cardiovascular composite end point was assessed in 5 studies, comprising 23 763 patients (11 911 in the SGLT‑2i arm and 11 852 in the placebo arm). The number of events for this outcome was reported in 4 of the 5 studies, involving 9145 patients (9602 in the SGLT‑2i arm and 9543 in the placebo arm). Among these patients, the dip status was reported for 9192 patients (5849 in the SGLT‑2i arm and 3342 in the placebo arm). In the SGLT‑2i arm, the cardiovascular composite end point occurred in 684 patients (11.7%) in the dip group and 556 patients (14.8%) in the nondip group. While the definition of the cardiovascular composite end point varied slightly among the studies (Table 1), it consistently included cardiovascular mortality and HF hospitalization or HF events (defined as HF hospitalization or urgent visit).
The eGFR dip was not associated with an adverse impact on the cardiovascular composite end point (HR, 0.88; 95% CI, 0.76–1.01; P = 0.07). In contrast, in the placebo group, the dip was linked to a worse prognosis (HR, 1.35; 95% CI, 1.19–1.52; P <0.001). Significant heterogeneity was noted among the studies (I2 = 51%; P = 0.09). In the intervention arm, the dip did not affect the cardiovascular composite end point (RD, –0.01; 95% CI, –0.04 to 0.01; P = 0.32), whereas in the placebo arm, it was associated with worse prognosis (RD, 0.02; 95% CI, 0–0.05; P = 0.02).
Subgroup analysis showed that in the general HF population (irrespective of EF) and in the patients with HFpEF, the effect of the eGFR dip remained nonsignificant (HR, 0.87; 95% CI, 0.74–1.01; P = 0.07 and HR, 0.98; 95% CI, 0.84–1.13; P = 0.74, respectively), while in the HFrEF population, it was associated with improved outcomes (HR, 0.76; 95% CI, 0.66–0.88; P <0.001). In contrast, in the placebo group, the dip was consistently associated with worse prognosis across all subgroups: HF (HR, 1.39; 95% CI, 1.23–1.57; P <0.001), HFrEF (HR, 1.38; 95% CI, 1.01–1.88; P = 0.04), and HFpEF (HR, 1.39; 95% CI, 1.2–1.61; P <0.001). With respect to the effect of the dip magnitude, a moderate dip (0% to 10%–11.8%) showed a significant positive effect (HR, 0.83; 95% CI, 0.69–0.99; P = 0.04), whereas a greater dip (>10%–11.8%) did not have a significant effect on the cardiovascular composite end point (P = 0.28; Supplementary material, Figure S6).
The use of a SGLT‑2i, as compared with placebo, was associated with a positive effect on the cardiovascular composite end point in the dip range of 0%–1.1% to 10%–11.8% (RD, –0.04; 95% CI, –0.07 to –0.01; P = 0.006) and greater than 10%–11.8% (RD, –0.04; 95% CI, –0.06 to –0.02; P <0.001), but not if the dip in eGFR exceeded 25%–30% (RD, –0.06; 95% CI, –0.13 to 0.02; P = 0.12; Supplementary material, Figure S7).
Kidney composite end point
The kidney composite end point was evaluated in 4 studies, encompassing 19 064 patients (9551 in the intervention arm and 9513 in the placebo arm). Dip occurrence was reported for 9145 patients (5815 in the SGLT‑2i arm vs 3330 in the placebo arm). In the SGLT‑2i arm, the kidney composite end point occurred in 221 patients (3.8%) in the dip group and 85 patients (2.3%) in the nondip group. Although the definitions varied slightly, they consistently included a combination of doubling of serum creatinine levels, end‑stage kidney disease, a decline in eGFR greater than or equal to 50%, or kidney‑related mortality (Table 1). The eGFR dip had a neutral effect on the kidney composite outcome (HR, 1.25; 95% CI, 0.88–1.77; P = 0.22). In contrast, in the placebo group, the dip was associated with worse prognosis (HR, 1.61; 95% CI, 1.34–1.94; P <0.001). Significant heterogeneity was observed (I2 = 55%; P = 0.08).
In the intervention arm, the dip had no significant effect on the kidney composite outcome (RD, 0; 95% CI, 0–0.01; P = 0.22), while in the placebo arm, it was associated with worse prognosis (RD, 0.02; 95% CI, 0.00–0.04; P = 0.02). The dip was linked to worse kidney prognosis in the general HF population (HR, 1.45; 95% CI, 1.01–2.09; P = 0.04) but this association was not observed in the HFpEF subgroup (HR, 1.38; 95% CI, 0.75–2.53; P = 0.3). In contrast, in the placebo group, the dip was strongly associated with worse prognosis in both the general HF population (HR, 1.74; 95% CI, 1.27–2.39; P <0.001) and the HFpEF subgroup (HR, 1.58; 95% CI, 1.1–2.27; P = 0.01). The effect of the dip on kidney outcomes remained nonsignificant across the entire range of dip magnitudes (Supplementary material, Figure S6). Furthermore, in the dip group, the effect of SGLT‑2i use vs placebo on kidney outcomes remained nonsignificant, regardless of the dip magnitude (Supplementary material, Figure S7).
All‑cause mortality
Overall mortality was analyzed in 4 studies involving 18 102 patients (9059 in the SGLT‑2i arm and 9043 in the placebo arm). The number of events for this outcome was reported in 3 of the 4 studies, involving 13 484 patients (6750 in the SGLT‑2i arm and 6734 in the placebo arm). Among these patients, the dip status was recorded for 7354 individuals (4727 in the SGLT‑2i arm and 2647 in the placebo arm). In the SGLT‑2i arm, death occurred in 479 patients (10.1%) in the dip group, as compared with 233 patients (11.5%) in the nondip group. The eGFR dip was not associated with an increased risk of death, regardless of the underlying cause (HR, 0.9; 95% CI, 0.7–1.15; P = 0.4). In contrast, in the placebo group, a significant association was observed between the eGFR dip and worse prognosis (HR, 1.31; 95% CI, 1.15–1.5; P <0.001). Significant heterogeneity was observed (I2 = 75%, P = 0.008). The dip did not significantly influence outcomes in either the intervention (RD, –0.01, 95% CI, –0.03 to 0.02; P = 0.64) or the placebo group (RD, 0.02; 95% CI, 0.00–0.03; P = 0.07).
In the intervention arm, the eGFR dip was associated with a reduction in all‑cause mortality (ACM) in the HFrEF population (HR, 0.81; 95% CI, 0.69–0.96; P = 0.02) but not in the general HF population (HR, 0.93; 95% CI, 0.7–1.24; P = 0.64). In contrast, in the placebo arm, the eGFR dip was consistently associated with worse prognosis across all assessed subgroups: HF (HR, 1.33; 95% CI, 1.15–1.55; P <0.001) and HFrEF (HR, 1.39; 95% CI, 1.14–1.68; P <0.001; Supplementary material, Figure S8).The effect of the dip in the intervention arm remained nonsignificant, regardless of its magnitude (Supplementary material, Figure S6).
SGLT‑2i use, as compared with placebo, was positively associated with a reduction in ACM for patients with a dip magnitude greater than 10%–11.8% (RD, –0.02; 95% CI, –0.04 to 0; P = 0.03) but not for those with a dip in the range of 0%–10%–11.8% (RD, –0.01; 95% CI, –0.04 to 0.02; P = 0.37).
Cardiovascular mortality
Cardiovascular mortality was assessed in 3 studies involving 13 945 patients (6984 in the SGLT‑2i arm and 6961 in the placebo arm). The number of events for this outcome was reported in 2 out of the 3 studies, involving 9327 patients (4675 in the SGLT‑2i arm and 4652 in the placebo arm). Among these patients, the dip status was documented for 4650 participants, including 3100 in the SGLT‑2i arm and 1550 in the placebo arm. In the SGLT‑2i arm, cardiovascular death occurred in 231 patients (7.5%) in the dip group and 136 patients (8.6%) in the nondip group. In the intervention arm, the dip was not associated with an increased risk of cardiovascular death (HR, 0.85; 95% CI, 0.65–1.11; P = 0.24), with significant heterogeneity observed (I2 = 67%; P = 0.05). In contrast, in the placebo group, a clear association was observed between the dip occurrence and worse prognosis (HR, 1.42; 95% CI, 1.19–1.7; P <0.001).The dip did not significantly affect outcomes in either the intervention (RD, –0.01; 95% CI, –0.04 to 0.02; P = 0.38) or the placebo group (RD, 0.02; 95% CI, 0–0.04; P = 0.13).
In the intervention arm, the dip was significantly associated with better prognosis in the HFrEF population (HR, 0.75; 95% CI, 0.61–0.91; P = 0.004) but not in the general HF population (HR, 0.85; 95% CI, 0.65–1.11; P = 0.24). In contrast, in the placebo group, the dip was associated with worse prognosis in both subgroups: HF (HR, 1.42; 95% CI, 1.19–1.7; P <0.001) and HFrEF (HR, 1.44; 95% CI, 1.16–1.79; P <0.001). The effect of the dip remained nonsignificant regardless of its magnitude (Supplementary material, Figure S6). Additionally, there was no association between the SGLT‑2i effect and placebo across the entire range of dip magnitudes (Supplementary material, Figure S7).
Risk of bias and certainty of evidence
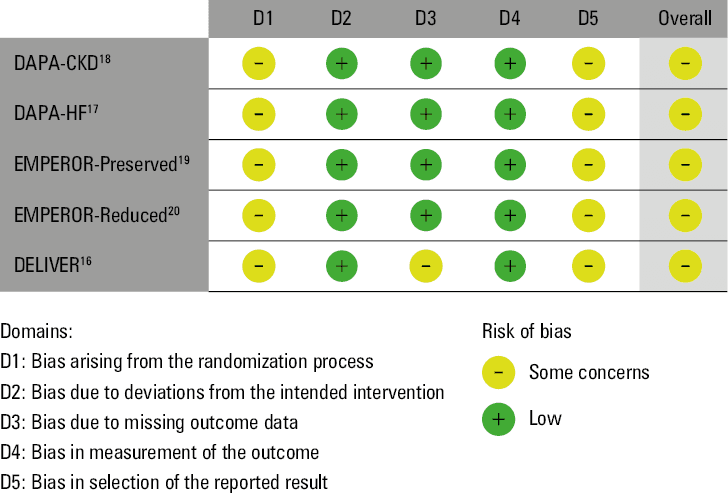
The outcomes of the risk of bias evaluation are presented in Figure 4. Overall, the risk of bias was categorized as indicating some concerns, while the quality of evidence ranged from very low to low‑to‑moderate, contingent upon the specific outcome (Table 4). Due to the fact that absolute event numbers were not reported in some studies, it was not possible to calculate the anticipated absolute risk.
End point | Patients / included studies, n | Quality of evidence | HR (95% CI) |
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the placebo group and the relative effect of the intervention (and its 95% CI).
a The degree of variability between studies may represent moderate heterogeneity, but CIs overlap and statistical test for heterogeneity is >0.05.
b Differences in population type translate into different baseline risks (eg, some studies evaluated HF patients only, while 1 study evaluated adults with CKD and albuminuria). Different time points for assessing the eGFR dip.
c The total number of events does not meet the optimal size; however, the group size is large.
d The total number of events meets the optimal size of 400, by the rule of thumb, to meet the threshold. The 95% CI indicates no effect and does not indicate appreciable benefit or harm.
e The degree of variability between studies represents substantial heterogeneity, CIs partially overlap, and the statistical test for heterogeneity is ≥0.05.
f All studies evaluated patients with HF only.
g The total number of events does not meet the optimal information size.
h Wide CI; the 95% CI indicates no effect and appreciable benefit.
Abbreviations: HR, hazard ratio; others, see Table 2 | |||
Kidney composite | 9551 / 4 RCTs | Lowa,b,c | 1.25 (0.88–1.77) |
CV composite | 11 910 / 5 RCTs | Moderatea,b,d | 0.88 (0.76–1.01) |
CV mortality | 6983 / 3 RCTs | Very lowe,f,g | 0.85 (0.65–1.11) |
ACM | 9058 / 4 RCTs | Very lowb,e,h | 0.9 (0.7–1.15) |
Discussion
Our meta‑analysis, which included only RCTs, summarized the evidence on the impact of the initial eGFR decline following SGLT‑2i initiation. Our findings suggest that the initial eGFR dip is safe and may even be beneficial for cardiovascular outcomes. To the best of our knowledge, this is the first meta‑analysis to demonstrate the association between eGFR decline after SGLT‑2i initiation and patient prognosis.
Although the dip following SGLT‑2i initiation remained nonsignificant across all analyzed outcomes in the primary analysis, some important distinctions are worth further elaboration. The quantitative analysis of the cardiovascular composite end point did not reach statistical significance; however, the numerical effect was positive. This effect was significant in the SGLT‑2i group for the patients experiencing a mild eGFR dip in the range of 0%–11.8% vs the baseline eGFR. A significant reduction in cardiovascular composite end point, cardiovascular mortality, and ACM was also observed in the HFrEF subgroup (Supplementary material, Figure S8).
A particularly intriguing observation pertains to the difference in the dip effect across the treatment arms in the analyzed studies, specifically between the SGLT‑2i and placebo arms. Although nonsignificant, a nearly symmetrical pooled effect was evident in the forest plots for various outcomes, comparing the intervention and placebo groups. In the SGLT‑2i group, the dip effect was numerically favorable or neutral, while in the placebo group, it was associated with worse outcomes. Notably, for the cardiovascular composite end point, where the beneficial effect of the dip in the SGLT‑2i arm appeared to be the most pronounced, a dip in the placebo arm was strongly linked to worse outcomes.
Moreover, in an isolated analysis of patients who experienced a dip, SGLT‑2is vs placebo generally demonstrated a trend toward a favorable effect of the drug regardless of the dip magnitude; however, these effects did not achieve statistical significance.
On the other hand, among the patients on placebo, the eGFR dip appeared to be associated with worse renal outcomes. In the placebo group, this effect was significant, whereas in the intervention group, only a numerical trend was observed. Additionally, the detrimental effect seemed to be more pronounced for dips greater than 10%–11.8%, as compared with dips within the range of 0% to 10%–11.8%. These data show that the eGFR dip following SGLT‑2i initiation is associated with opposing trajectories in cardiovascular vs renal prognosis. The cause of this divergence remains unclear at this time.
The underlying mechanisms of the eGFR dip and its possible favorable effect remain unclear; however, several hypotheses have been proposed. The initial eGFR dip may simply identify the patients who adhere to treatment recommendations. Proposed mechanisms include changes in tubuloglomerular feedback, where SGLT‑2i reduces sodium and glucose reabsorption in the proximal tubule, leading to increased sodium delivery to the macula densa and consequent constriction of the afferent renal arteriole, thus reducing eGFR. This is a process opposite to that observed in the early stage of T2DM, where dilation of the afferent arteriole leads to an increase in eGFR.29 This feedback mechanism appears to diminish over time. Additionally, a decrease in 8‑isoprostane, a marker of oxidative stress, has been observed following flozin initiation.13,30 Conversely, some evidence suggests that improved renal hemodynamics may be due to postglomerular vasodilation mediated by the adenosine receptor activation, rather than preglomerular vasoconstriction.31 SGLT‑2is have also been shown to reduce the levels of renal injury biomarkers, such as albuminuria, kidney injury molecule 1, interleukin 6, tumor necrosis factor receptor (TNFR)-1, and TNFR‑2, with each 10% reduction in TNFR associated with a lower risk of kidney outcomes.32,33 Additionally, SGLT‑2is have demonstrated anti‑inflammatory and antifibrotic properties, thereby mitigating unfavorable remodeling of tubular cells.34 Flozins are also associated with increased excretion of uric acid, a recognized cardiovascular disease risk factor, and enhanced reabsorption of phosphate and magnesium, which helps prevent arrhythmias. Furthermore, SGLT‑2i–induced localized hypoxia in tubular cells stimulates erythropoietin secretion, leading to an elevated hemoglobin concentration. The reduced workload of proximal tubular cells further contributes to a decreased risk of acute kidney injury.35-37 Moreover, the initiation of an SGLT‑2i is associated with augmentation of diuresis and effective decongestion; this could potentially lead to a decrease in plasma volume and hemoconcentration.38,39 Further mechanistic studies are necessary to fully understand this phenomenon and its prognostic implications.40
A particularly interesting phenomenon is the occurrence of the eGFR dip even in the placebo group (Figure 2). Several explanations have been proposed for this observation. One of them is the natural progression of CKD, which aligns with our findings demonstrating that the initial dip in this group was consistently associated with worse prognosis across all assessed outcomes. Another contributing factor may be the impact of concomitant pharmacotherapy, such as angiotensin‑converting enzyme inhibitors or angiotensin II receptor blockers, which can induce a transient decrease in eGFR at the initiation of therapy. It is plausible that at the time of trial enrolment, treatment optimization beyond SGLT‑2is was implemented in both the intervention and placebo groups.
Understanding that the initial eGFR dip post–SGLT‑2i initiation is safe and potentially beneficial has significant clinical implications. Specifically, an eGFR reduction of approximately 10% should not deter physicians from continuing SGLT‑2i therapy. Conversely, a more pronounced decrease in eGFR—likely exceeding 30%—should not be presumed to be related to SGLT‑2i use; instead, it should prompt an investigation into alternative causes of acute kidney injury.41
Our study has several limitations that need to be considered. Firstly, pooling composite outcomes with different compositions may have impacted the results. The HRs used in our analysis were adjusted for various factors that could influence the findings. The results of the quantitative analysis for individual outcomes may originate from isolated populations; for example, data on cardiovascular mortality were derived exclusively from studies involving HF populations. Consequently, these findings cannot be fully generalized across all 3 populations: HF, CKD, and T2DM. Lastly, the study involved different SGLT‑2is, which introduces uncertainty regarding generalizability of the results to all drugs within this class.
In conclusion, unlike in the placebo arms of the included RCTs, where an eGFR dip was associated with unfavorable outcomes, the early eGFR dip in the patients receiving SGLT‑2is was either neutral or beneficial. The dip appears to confer a particularly favorable effect in the population of patients with HFrEF.
- Roddick AJ, Wonnacott A, Webb D, et al. UK Kidney Association Clinical Practice Guideline: sodium‑glucose co‑transporter‑2 (SGLT‑2) inhibition in adults with kidney disease 2023 UPDATE. BMC Nephrol. 2023; 24: 310. | Crossref
- Navaneethan SD, Zoungas S, Caramori ML, et al. Diabetes management in chronic kidney disease: synopsis of the KDIGO 2022 clinical practice guideline update. Ann Intern Med. 2023; 176: 381‑387. | Crossref
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42: 3599‑3726.
- McDonagh TA, Metra M, Adamo M, et al. 2023 Focused update of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2023; 44: 3627‑3639. | Crossref
- Heerspink HJL, Stefánsson B V, Correa‑Rotter R, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020; 383: 1436‑1446. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION