Breaking the weight loss paradox: from weight reduction to cardiovascular benefit in obesity treatment
Key words: cardiovascular risk reduction, glucagon-like peptide-1 receptor agonists, incretin-based therapies, metabolic syndrome, obesity pharmacotherapy

 CC BY 4.0
CC BY 4.0
Breaking the weight loss paradox: from weight reduction to cardiovascular benefit in obesity treatment
Obesity is a growing global epidemic and a major risk factor for cardiovascular disease. However, previous weight loss interventions have largely failed to demonstrate consistent cardiovascular benefits. While lifestyle modifications remain the cornerstone of obesity management, their long‑term efficacy is limited, and most individuals eventually regain the lost weight. Pharmacological approaches have historically been hindered by safety concerns and a lack of proven cardiovascular outcome benefits. Bariatric surgery remains the most effective intervention for long‑term weight management and metabolic improvement, with accumulating evidence supporting its role in reducing the incidence of cardiovascular events. However, its accessibility and eligibility criteria limit its widespread adoption. Recent advances in the use of glucagon‑like peptide‑1 receptor agonists and multireceptor agonists have transformed obesity treatment. Semaglutide became the first obesity pharmacotherapy to demonstrate a significant 20% reduction in the incidence of major adverse cardiovascular events in the SELECT trial, although its impact on secondary end points was neutral. More potent agents, such as tirzepatide and retatrutide, have achieved unprecedented weight loss (up to 24%), raising the possibility of greater cardiovascular benefits. Beyond weight loss, these drugs exert pleiotropic effects on inflammation, endothelial function, and atherosclerosis, which may contribute to their cardioprotective potential. As pharmacotherapy continues to evolve, personalized treatment approaches targeting metabolic dysfunction and cardiovascular health will be crucial in redefining obesity care. This review explores the current landscape of obesity pharmacotherapy, its cardiovascular implications, and the emerging role of next‑generation therapies in obesity management.
Introduction
According to the World Health Organization recommendations, obesity is considered a chronic disease and is also included in the International Classification of Diseases and Related Health Problems 11th Revision.1,2 Since 1975, global obesity rates have nearly tripled.3 In 2020, overweight and obesity (defined as a body mass index [BMI] ≥25 kg/m²) affected over 2.6 billion people (38% of the world’s population), with projections surpassing 4 billion (50%) by 2035.4 The most rapid increase is expected among children and adolescents, with rates doubling over the next 15 years. The economic burden of overweight and obesity is projected to exceed 4 trillion USD annually by 2035 (about 2.9% of the global gross domestic product).4 Obesity is a risk factor for nearly 200 diseases, including cardiovascular, neuropsychological, pulmonary, gastrointestinal, endocrine, oncologic, immune, and musculoskeletal disorders.5,6
Obesity and cardiovascular disease
Obesity combined with atherosclerotic cardiovascular disease (CVD) creates a high‑risk condition.1,7 It significantly increases the risk of hypertension, coronary artery disease, heart failure (HF), and stroke, contributing to higher overall mortality (Figure 1).2 A recent analysis of 12 systematic reviews, encompassing the results of 53 meta‑analyses (including over 501 cohort studies) and 12 Mendelian randomization studies, linked an increase in BMI to a higher risk of coronary artery disease, HF, atrial fibrillation (AF), stroke, hypertension, aortic valve stenosis, pulmonary embolism, and venous thromboembolism.8 Mendelian randomization analysis confirmed causal links between obesity and all these conditions except for stroke.8 A 5‑kg/m2 increase in BMI is associated with a relative increase in cardiovascular risk, ranging from 10% for stroke to 49% for hypertension.8 Interestingly, although obesity is strongly linked to cardiovascular risk factors, a Mendelian randomization analysis did not identify a causal relationship between obesity and all‑cause mortality.8 However, a separate meta‑analysis found higher overall mortality across all obesity grades except for grade 1 (BMI, 30–35 kg/m²), as compared with normal body weight (BMI, 18.5–25 kg/m²).9 While the association between obesity and CVD is well documented, its direct impact on all‑cause mortality remains unclear.8,9 Nonetheless, it is indisputable that obesity, even in the absence of other traditional risk factors, significantly contributes to CVD morbidity and increases the risk of severe complications (Figure 1).
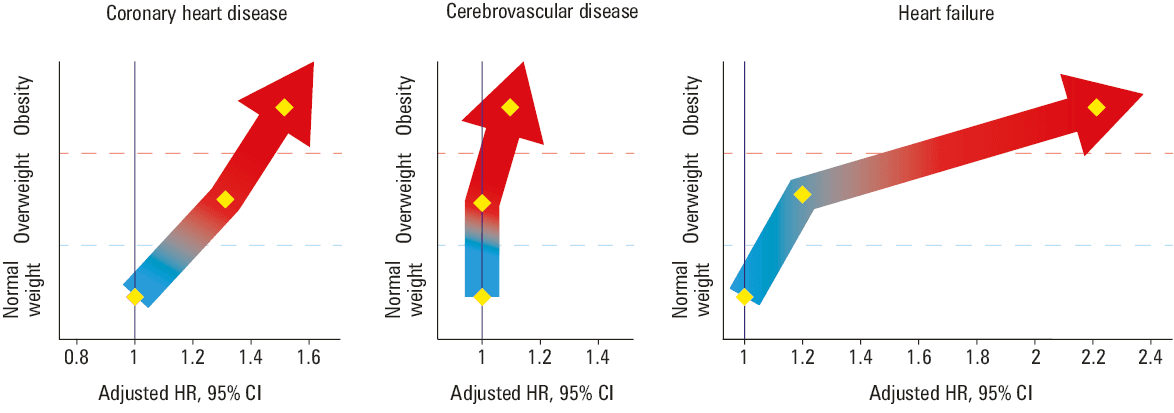
Abbreviations: HR, hazard ratio
According to the Global Burden of Disease Study, high BMI was associated with approximately 4 million deaths worldwide in 2015, with more than two‑thirds of these deaths attributed to CVD.7 Moreover, obesity exacerbates mortality rates in patients with pre‑existing CVD.7 The COVID‑19 pandemic further highlighted the risks associated with obesity, as individuals with higher BMI and pre‑existing CVD were disproportionately affected by severe and fatal outcomes of the disease.1 Given these findings, weight reduction should be a central component of cardiovascular risk management strategies. However, pharmacologic interventions for obesity have faced challenges, primarily due to the lack of robust evidence from cardiovascular outcome trials (CVOTs) demonstrating their efficacy in improving cardiovascular end points (Table 1).1,10
Trial | Intervention | Patients enrolled | Design | Event rate | HR | Discontinuation rate | Primary outcome | Results |
a Interim analysis after 50% of planned events
b Based on ClinicalTrials.gov (ClinicalTrials.gov identifier: NCT05556512)
| ||||||||
LOOK AHEAD21 | ILI | 5145 | Superiority | 1.83 events per 100 person‑years (ILI) vs 1.92 (control) | HR, 0.95 (95% CI, 0.83–1.09; P = 0.51) | Not specified | MACE | No significant reduction in CV events; terminated early for futility |
SCOUT23 | Sibutramine | 10 744 | Superiority | 11.4% (sibutramine) vs 10% (placebo) | HR, 1.16 (95% CI, 1.03–1.31; P = 0.02) | 30% | MACE + resuscitated cardiac arrest | Increased risk of nonfatal MI and stroke; led to market withdrawal |
CRESCENDO32 | Rimonabant | 18 695 | Superiority | 3.9% (rimonabant) vs 4% (placebo) | HR, 0.97 (95% CI, 0.84–1.12; P = 0.68) | 10% | MACE + CV hospitalization | No significant CV benefit; increased psychiatric adverse events; terminated early |
LIGHT32 | Naltrexone / bupropion | 8910 | Noninferiority | 2% (naltrexone / bupropion) vs 2.3% (placebo)a | HR, 0.88; adjusted 99.7% CI, 0.57–1.34a | 28.1% | MACE + angina hospitalization | Terminated due to data integrity concerns |
CONVENE38 | Naltrexone / bupropion | About 8800 | Noninferiority | ND | ND | ND | MACE | Terminated early |
CAMELLIA‑TIMI24 | Lorcaserin | 12 000 | Noninferiority | 2% (lorcaserin) vs 2.1% (placebo) | HR, 0.99 (95% CI, 0.85–1.14) | 5% | MACE + type 2 diabetes | Demonstrated noninferiority for CV safety; later withdrawn due to cancer risk concerns |
SELECT10 | Semaglutide 2.4 mg | 17 604 | Superiority | 6.5% (semaglutide) vs 8% (placebo) | HR, 0.8 (95% CI, 0.73–0.87; P <0.001) | 16.6% | MACE | Significant 20% reduction in MACEs, superior to placebo |
SURMOUNT‑MMOb | Tirzepatide 15 mg | 15 374 | Superiority | Ongoing | Ongoing | Ongoing | MACE | Ongoing study; results pending 2027b |
Adipose tissue dysfunction and systemic inflammation as key drivers of obesity‑related cardiovascular disease
Obesity‑related cardiovascular complications are caused by adipose tissue dysfunction, metabolic dysregulation, and systemic inflammation, collectively increasing cardiovascular morbidity and mortality (Figure 2).11 Excessive and dysfunctional adipose tissue, particularly visceral fat, triggers chronic low‑grade inflammation, characterized by increased secretion of proinflammatory cytokines (such as tumor necrosis factor [TNF] α and interleukin [IL]-6), oxidative stress mediators, and altered adipokine profiles (leptin, adiponectin, resistin, and visfatin).6 These factors promote endothelial dysfunction, insulin resistance, and abnormal lipid metabolism, ultimately leading to atherosclerosis, hypertension, and myocardial dysfunction.11 Dudek et al12 showed that severe obesity is associated with shorter telomeres, elevated IL‑6 levels, and advanced metabolic age, suggesting a direct link between adiposity, inflammation, and premature aging. Similarly, Pakiet et al13 found that obesity is associated with a proinflammatory oxylipin profile, which is mitigated by bariatric surgery, highlighting the role of chronic inflammation in obesity‑related cardiovascular risk and potential benefits of a surgical intervention.

Abbreviations: CRP, C‑reactive protein; IL, interleukin; MCP, monocyte chemoattractant protein; RAA; renin‑angiotensin‑aldosterone; TNF-α, tumor necrosis factor α
Dysfunctional adipose tissue, with impaired expandability and increased fibrosis, promotes ectopic lipid deposition in vital organs, such as the heart, liver, pancreas, and kidneys.14 Epicardial and pericardial fat causes local inflammation that contributes to myocardial fibrosis, left ventricular hypertrophy, and AF. Furthermore, perivascular adipose tissue dysfunction exacerbates vasoconstriction, arterial stiffness, and atherogenesis.14 The metabolic effects of obesity, including insulin resistance, dyslipidemia, and hyperglycemia further increase cardiovascular risk by enhancing oxidative stress, thrombogenesis, and endothelial dysfunction.11 Metabolic dysfunction–associated steatotic liver disease (MASLD) plays a significant role in obesity‑related complications.15 However, standard noninvasive diagnostic tools for nonalcoholic fatty liver disease require adjustments in individuals with severe obesity, highlighting the impact of obesity on metabolic and hepatic dysfunctions.15 Zieleniewska et al16 also demonstrated that abdominal obesity significantly increases the risk of glucose metabolism disorders, including prediabetes and type 2 diabetes (T2D), further emphasizing the strong association between obesity, metabolic syndrome, and CVD.
Systemic inflammation, evidenced by elevated levels of C‑reactive protein (CRP) and other inflammatory markers, is a key driver of obesity‑related CVD, correlating with increased atherosclerotic burden and cardiovascular events (Figure 2).11 Klejbuk and Strączkowski17 demonstrated that weight loss improves insulin sensitivity and increases the expression of NLRP12 (a negative nuclear factor κB regulator) in subcutaneous adipose tissue, suggesting a potential anti‑inflammatory effect. Strączkowski et al18 further showed that weight loss in obesity normalizes glucocorticoid‑related gene expression, enhances glucocorticoid signaling, and improves insulin sensitivity, highlighting the complex interplay between adipose tissue metabolism and inflammation. These findings demonstrate how adipose tissue dysfunction leads to metabolic derangements, systemic inflammation, and endothelial dysfunction, ultimately resulting in cardiovascular complications. Moreover, the interrelations between obesity, metabolic syndrome, and chronic kidney disease create a self‑perpetuating cycle of cardiorenal impairment, further exacerbating cardiovascular risk (Figure 2).11
In summary, obesity is a complex, multisystemic disease that accelerates cardiovascular pathology through metabolic dysregulation, inflammation, oxidative stress, and structural cardiac changes. Effective treatment requires targeted strategies addressing weight loss, adipose tissue function, and metabolic normalization to reduce the burden of obesity‑related CVDs.
Lifestyle interventions for obesity and cardiovascular risk: efficacy, limitations, and long‑term outcomes
Comprehensive obesity management requires a systematic assessment of adherence to a healthy lifestyle (increased physical activity, dietary compliance, and weight management) and existing cardiovascular risk factors. Current European Society of Cardiology (ESC) guidelines on CVD prevention recommend weight reduction in patients with overweight or obesity to lower blood pressure and mitigate the risk of T2D (class IA recommendation).19 Caloric restriction is the primary approach to weight loss, while physical activity is crucial for maintaining weight reduction and preventing weight regain.19 A plant‑based, hypocaloric Mediterranean diet is endorsed as an effective intervention to reduce both weight and the incidence of cardiovascular events, showing more sustained benefits than low‑carbohydrate diets, restrictive food plans (eg, vegetables and fruits), or time‑restricted eating.19,20 Successful long‑term outcomes are largely dependent on dietary quality, particularly replacing saturated fats with unsaturated fats and increasing fiber intake.19,20 The complex interplay between alcohol consumption, obesity, and cardiovascular complications was recently highlighted by Surma and Gajos.20 Excessive alcohol intake, even in individuals following the Mediterranean diet, significantly contributes to global morbidity and mortality, worsening obesity‑related cardiovascular complications, such as hypertension, coronary artery disease, and AF.20 This is evidenced by a 72% increase in the prevalence of combined heavy drinking and obesity among United States adults from 1999 to 2020.20
While behavioral and pharmacologic weight loss interventions improve cardiovascular risk factors, such as blood pressure and glycemic control in patients with obesity, no interventional study has shown that nonsurgical weight loss reduces the incidence of major adverse cardiovascular events (MACEs; Figure 3).21-25 A large, prospective, randomized LOOK AHEAD (Action for Health in Diabetes) trial in 5145 patients with T2D and overweight or obesity reported significant weight loss (8.6% vs 0.7% at 1 year) with intensive dietary intervention vs routine management. However, it ultimately failed to show any reduction in MACEs (including cardiovascular death) after nearly 10 years of follow‑up, resulting in the study termination (Table 1, Figure 3).21 A post hoc analysis revealed that only the participants who achieved more than 10% weight loss in the first year experienced a significant 21% reduction in cardiovascular events (hazard ratio [HR], 0.79; 95% CI, 0.64–0.98), as compared with those with stable weight or weight gain, suggesting that the cardiovascular benefits of lifestyle intervention may be limited to those achieving substantial weight loss.26 However, recent data from the LOOK AHEAD trial demonstrated weight regain in nearly all individuals who intentionally lost weight.27 Moreover, individuals with a greater genetic predisposition for abdominal adiposity experienced a greater increase in waist circumference after weight loss.
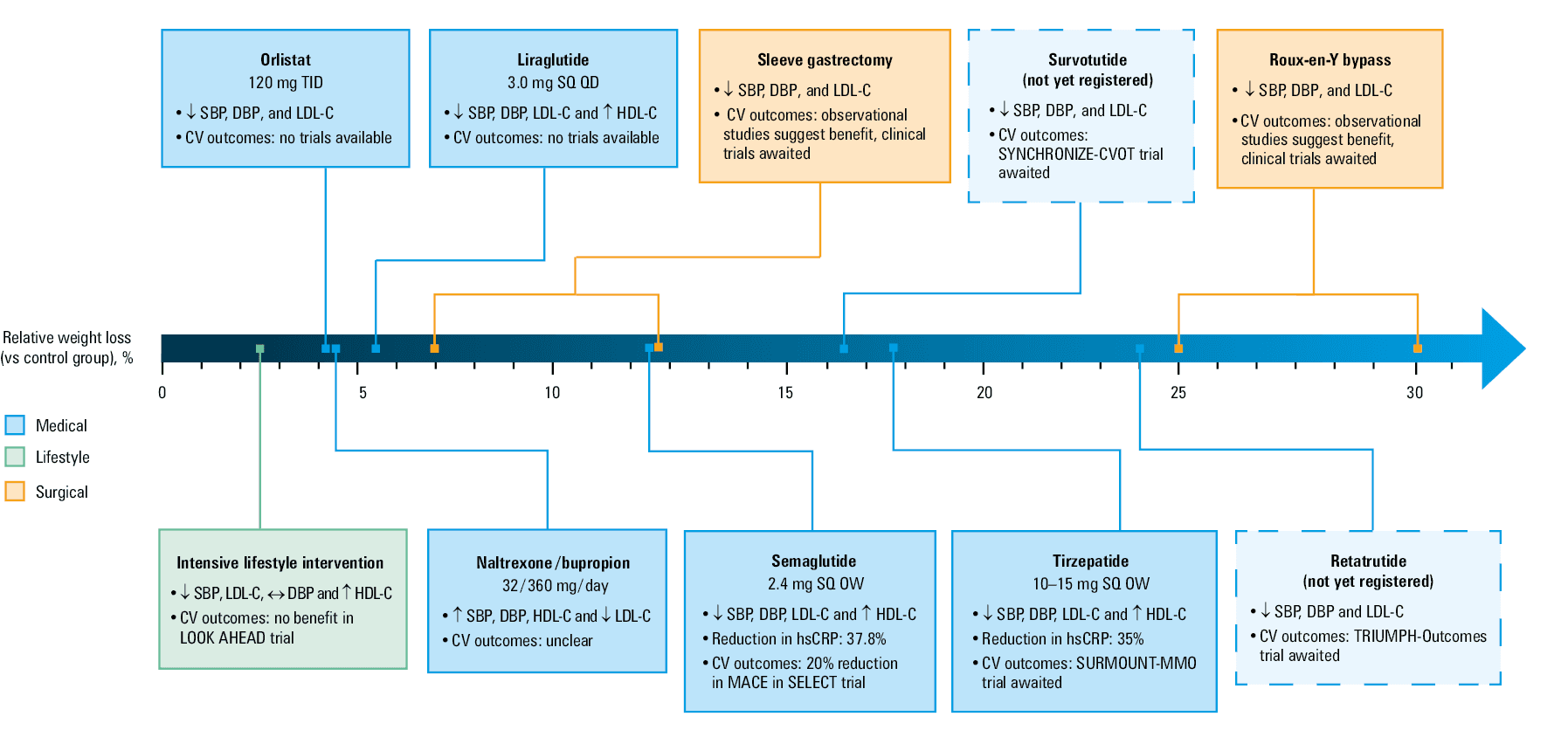
Abbreviations: CV, cardiovascular; CVOT, cardiovascular outcomes trial; DBP, diastolic blood pressure; HDL‑C, high‑density lipoprotein cholesterol; hsCRP, high‑sensitivity C‑reactive protein; LDL‑C, low‑density lipoprotein cholesterol; MACE, major adverse cardiovascular event (cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke); OD, once daily; OW, once a week; SBP, systolic blood pressure; SQ, subcutaneous; TID, three times a day
Polemiti et al28 showed that weight reduction (as compared with stable weight) was associated with a lower risk of microvascular complications (nephropathy, neuropathy, and retinopathy) in patients with T2D. However, the relationship between BMI and macrovascular complications remains unclear. A large‑scale observational study (n = 138 567) using electronic health records found that weight loss in individuals with obesity was associated with a lower risk of coronary heart disease but not stroke or overall CVD.29 This suggests that weight loss may selectively benefit coronary health rather than reduce overall cardiovascular risk, highlighting the complex relationship between weight management and CVD prevention.29
In summary, lifestyle interventions, including caloric restriction and physical activity, remain the foundation of obesity management. However, despite improvements in cardiovascular risk factors, studies such as LOOK AHEAD and large‑scale observational analyses suggest that lifestyle interventions alone do not significantly reduce the incidence of MACEs, and most individuals eventually regain lost weight, particularly those with a genetic predisposition to abdominal adiposity.
Obesity pharmacotherapy: a legacy of failures and unmet expectations
In response to increasing demand and the limited effectiveness of lifestyle interventions, various pharmacotherapies have been investigated for obesity treatment since the 1940s. Until recently, the number of approved drugs remained limited, with many withdrawn shortly after introduction due to significant adverse events (AEs; Table 1).30
Desoxyephedrine (methamphetamine) was the first drug approved for short‑term obesity treatment (<3 months) in 1947, followed by phenmetrazine and phentermine. Phentermine, a methylated amphetamine derivative, stimulates catecholamine neurotransmitters peripherally and increases central dopamine and norepinephrine levels, suppressing appetite. However, due to significant AEs and addiction potential, these agents were withdrawn and are no longer used for obesity treatment.30
In the 1990s, new pharmacologic agents and their combinations emerged.30 The fenfluramine‑phentermine combination, along with dexfenfluramine (an isomer of fenfluramine) and sibutramine, were approved for long‑term obesity treatment.30,31 However, regulatory concerns arose after dexfenfluramine was linked to neurotoxicity in animal studies, while epidemiologic data suggested an increased risk of primary pulmonary hypertension and valvular heart disease with long‑term use.31 Importantly, the randomized prospective double‑blind SCOUT study (Sibutramine Cardiovascular Outcomes Trial) found that sibutramine increased the risk of nonfatal myocardial infarction (MI) and stroke in overweight and obese patients with pre‑existing CVD. However, no increase in cardiovascular or all‑cause mortality was documented (Table 1).23
In the 2000s, rimonabant, a cannabinoid‑1 receptor antagonist, was introduced as an antiobesity agent. However, the CRESCENDO trial (Comprehensive Rimonabant Evaluation Study of Cardiovascular Endpoints and Outcomes), a large‑scale CVOT in 18 695 patients, was terminated prematurely due to an unacceptable incidence of serious neuropsychiatric AEs, including depression and suicide (Table 1).32
In 2018, the CAMELIA‑TIMI 61 (Cardiovascular and Metabolic Effects of Lorcaserin in Overweight and Obese Patients–Thrombolysis in Myocardial Infarction 61) trial evaluated lorcaserin, a centrally acting selective serotonin 5HT‑2C receptor agonist targeting the hypothalamus, in a high‑cardiovascular‑risk population (atherosclerotic CVD or multiple cardiovascular risk factors) with overweight or obesity.24 Compared with placebo, lorcaserin facilitated sustained weight loss but had no impact on MACE incidence.24 However, subsequent analyses revealed a potential association between lorcaserin use and an increased risk of cancer (one additional cancer case per 470 patients treated annually). In February 2020, the United States Food and Drug Administration (FDA) requested the voluntary withdrawal of lorcaserin from the market due to these concerns (Table 1).33
Orlistat, introduced in 1998, remains the longest used approved treatment for obesity. It is a long‑acting gastrointestinal lipase inhibitor that reduces fat absorption and caloric intake by inhibiting hydrolysis of dietary triglycerides.34 At the recommended dose, it reduces fat absorption by approximately 30%. It is indicated for patients with a BMI of 28 kg/m² or higher in combination with a hypocaloric diet.34
The ORliCARDIA (Orlistat and Cardiovascular Risk Profile in Patients with Metabolic Syndrome and Type 2 Diabetes) study demonstrated that orlistat reduced weight, waist circumference, and cardiovascular risk factors, including fasting glucose, glycated hemoglobin (HbA1c), systolic blood pressure, low‑density lipoprotein cholesterol, and the Homeostasis Model Assessment of Insulin Resistance index.35 In a recent meta‑analysis of observational studies, orlistat use was linked to a lower incidence of MACEs, including newly diagnosed HF, renal failure, and mortality.36 However, there are no CVOTs specifically for orlistat, and patients with CVD were excluded from major clinical trials (Figure 3).25
Another approved treatment for obesity is a naltrexone / bupropion combination, which consists of 2 centrally acting agents: naltrexone, an opioid receptor antagonist approved for alcohol dependence, and bupropion, a selective norepinephrine and dopamine reuptake inhibitor indicated for major depressive episodes and nicotine addiction. Their combination exerts anorectic effects via sustained activation of anorexigenic hypothalamic neurons.19 According to the product characteristics, naltrexone‑bupropion is recommended as an adjunct to behavioral modifications, including a reduced‑calorie diet and increased physical activity, for adults with a BMI of 27 kg/m² or higher and at least 1 obesity‑related condition, such as hypercholesterolemia, T2D, or well‑controlled hypertension.37 Three phase 3 trials reported modest weight reductions after 56 weeks of treatment, as compared with placebo: 5.4% vs 1.3%, 8.1% vs 4.9%, and 3.7% vs 1.7%. Completion rates in the treatment arm ranged from 53% to 55%, reflecting significant dropout, likely due to AEs. In a fourth phase 3 trial (28‑week follow‑up), only 65.6% of patients receiving active treatment completed the study (vs 67.3% in the placebo group), with weight reductions of 5.7% (vs 1.9% in the placebo group).1,37 The most common AEs—nausea, vomiting, constipation, headaches, dizziness, and insomnia—frequently led to treatment discontinuation.1,37
In 2011, the LIGHT (Cardiovascular Outcomes Study of Naltrexone SR/Bupropion SR in Overweight and Obese Subjects With Cardiovascular Risk Factors; ClinicalTrials.gov identifier: NCT01601704) trial was initiated to assess MACE incidence in response to FDA concerns about potential cardiovascular effects, particularly blood pressure elevation (Figure 3).38 However, the trial was prematurely terminated.38 Interim analyses at 25% and 50% of planned end points found no significant increase in MACE incidence among overweight and obese patients with elevated cardiovascular risk.38,39 Nevertheless, the study’s noninferiority design could only exclude a 1.4‑fold increased risk. In 2015, the CONVENE trial (Naltrexone / Bupropion Cardiovascular Outcomes Study; ClinicalTrials.gov identifier: NCT02638129) was initiated to evaluate the cardiovascular safety of the naltrexone / bupropion combination in obese patients with CVD. However, the study was discontinued early in 2016 (Table 1).Thus, the cardiovascular safety of naltrexone‑bupropion remains uncertain, necessitating further research in well‑powered clinical trials (Table 1).38,39
Regulatory concerns following the LIGHT trial reflect a broader shift in obesity pharmacotherapy, with the FDA and European Medicines Agency now requiring comprehensive CVOTs before approval.25 While orlistat and naltrexone‑bupropion remain available, their clinical utility is limited by poor adherence, frequent AEs, and historically low insurance reimbursement. The inclusion of obesity management in cardiovascular prevention guidelines by the American Heart Association and ESC further underscores its role in long‑term risk reduction, necessitating continued evaluation of pharmacologic strategies beyond weight loss.19,25,40
Glucagon‑like peptide‑1 receptor agonists in obesity and cardiovascular disease: a breakthrough or just another step?
Liraglutide
Liraglutide, a glucagon‑like peptide‑1 receptor agonist (GLP‑1RA) originally developed for T2D management, is now approved for obesity treatment (Figure 4). It is indicated as an adjunct to diet and physical activity in adults and children aged 10 years or older, either alone or with oral antidiabetic agents and / or insulin.19
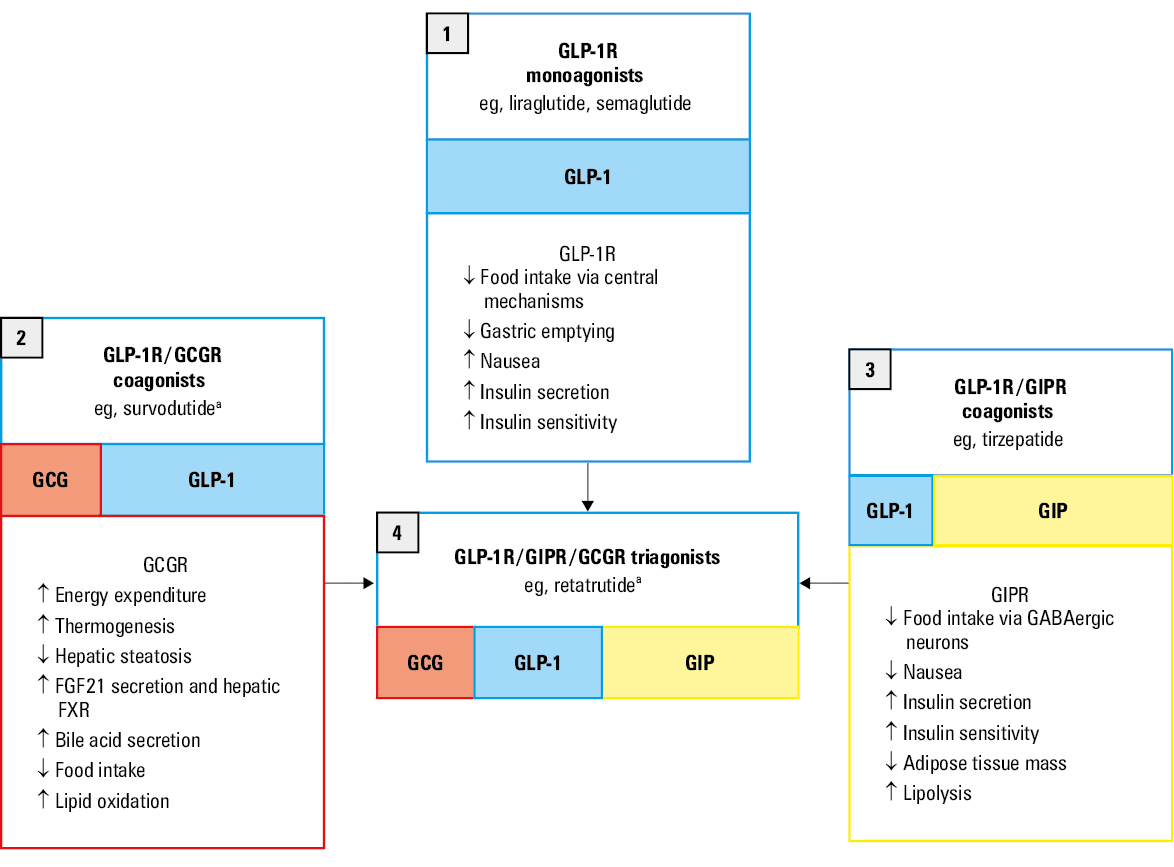
Abbreviations: FGF, fibroblast growth factor; FXR, farnesoid X receptor; GABA, gamma‑aminobutyric acid; GCGR, glucagon receptor; GIP, glucose‑dependent insulinotropic polypeptide; GIPR, glucose‑dependent insulinotropic polypeptide receptor; GLP‑1, glucagon‑like peptide‑1, GLP‑1R, glucagon‑like peptide‑1 receptor
The LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) trial assessed cardiovascular safety of liraglutide in patients with T2D, most of whom were obese.41 When added to standard therapy, liraglutide reduced MACE incidence (cardiovascular death, nonfatal MI, or nonfatal stroke), as compared with placebo.41 The SCALE (Satiety and Clinical Adiposity—Liraglutide Evidence) trial evaluated the effects of 3‑mg liraglutide (a higher dose than that for diabetes treatment) in nondiabetic patients with a BMI of 30 kg/m² or higher or of 27 kg/m² or higher with untreated dyslipidemia or hypertension. After 56 weeks, weight loss exceeding 5% was achieved in 63.2% of the liraglutide‑treated patients vs 27.1% in the placebo group, while a weight loss of 10% or greater was observed in 33.1% and 10.6%, respectively.42 Liraglutide also reduced systolic blood pressure (by about 2–5 mm Hg) and triglyceride levels, suggesting cardiovascular benefits beyond body weight reduction (Figure 3).42 Both trials showed significant reductions in HbA1c and fasting glucose levels with liraglutide treatment. Severe hypoglycemia was rare (1.3% vs 1% in SCALE; 2.4% vs 3.3% in LEADER), while transient gastrointestinal AEs (nausea, vomiting, diarrhea) occurred in 9%–21% of cases.41,42
Although the LEADER trial demonstrated cardiovascular benefits of liraglutide in T2D, its impact on MACEs in nondiabetic individuals remains uncertain. While a dedicated CVOT for liraglutide in nondiabetic patients with obesity is lacking, findings from the SCALE trial suggest potential cardiometabolic benefits beyond weight reduction.
Semaglutide
Semaglutide, a GLP‑1RA, has demonstrated significant efficacy in weight reduction and cardiovascular risk mitigation in individuals with T2D, most of whom were obese (Figure 4).43 The SUSTAIN and PIONEER trials evaluated its subcutaneous and oral formulations, respectively, in patients with T2D and increased cardiovascular risk.43,44 In SUSTAIN 6 (Trial to Evaluate Cardiovascular and Other Long‑term Outcomes with Semaglutide in Subjects with Type 2 Diabetes), weekly subcutaneous semaglutide (1 mg) led to a mean weight loss of 2.9 kg and a 26% reduction in MACEs, as compared with placebo.43 Similarly, PIONEER 6 (A Trial Investigating the Cardiovascular Safety of Oral Semaglutide in Subjects with Type 2 Diabetes) reported a 3.4‑kg weight reduction and a nonsignificant 21% decrease in MACEs with daily oral semaglutide.44
The STEP (Semaglutide Treatment Effect in People with Obesity) trials examined the effect of semaglutide on weight management in nondiabetic individuals with obesity.45 STEP 1 demonstrated that semaglutide at a weekly dose of 2.4 mg, which is higher than the dose used for diabetes treatment, led to a 12.4% placebo‑adjusted weight loss over 68 weeks (Figure 3).46 In contrast, STEP 2, which included individuals with T2D, showed a 6.2% placebo‑adjusted reduction, highlighting the reduced weight loss efficacy in this population. Beyond weight loss, the STEP trials demonstrated broad cardiometabolic benefits, including reductions in waist circumference (about 14 cm), systolic (about 6 mm Hg) and diastolic (about 2.9 mm Hg) blood pressure, and the levels of low‑density lipoprotein cholesterol (about 7%), triglycerides (about 20%), and CRP (about 40%; Figure 3).45
The recent SELECT trial (Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes) represents a significant advancement in the field.10 This study evaluated the efficacy of once‑weekly subcutaneous semaglutide (2.4 mg) vs placebo in reducing MACEs among 17 604 overweight or obese patients with pre‑existing CVD but without diabetes. Conducted across 804 clinical sites in 41 countries, the trial demonstrated a 20% reduction in the composite cardiovascular end point—comprising cardiovascular death, nonfatal MI, and nonfatal stroke—over a mean follow‑up of approximately 40 months (HR, 0.8; 95% CI, 0.72–0.9; P <0.001; Table 1). Notably, the early divergence in cardiovascular outcomes between the semaglutide and placebo groups, occurring before significant weight loss, suggests a direct effect on cardiovascular risk reduction. However, due to the lack of a significant reduction in cardiovascular death (P = 0.065) and the hierarchical testing approach, superiority testing was not conducted for the remaining confirmatory secondary end points, thereby limiting its overall impact. The absence of superiority in these additional measures was somewhat unexpected, particularly given that prior semaglutide cardiovascular trials in diabetes had demonstrated broader benefits across multiple outcomes. Nonetheless, the HRs for HF composite events (HR, 0.82; 95% CI, 0.71–0.96) and all‑cause mortality (HR, 0.81; 95% CI, 0.71–0.93) indicate a potential clinical benefit, though these findings remain hypothesis‑generating.10 Moreover, the average weight reduction of 8.5% in the SELECT trial was modest in comparison with the previous STEP trials and emerging therapies utilizing newer multireceptor agonists (Table 1).10
Recent analyses of metabolic outcomes from the SELECT trial further highlight its significance. As many as 66.4% of its participants met the criteria for prediabetes (HbA1c ≥5.7%), and semaglutide reduced the relative risk of developing diabetes by 73%. This represents a paradigm shift in prediabetes management, which has traditionally relied on lifestyle modifications and metformin.47 Moreover, the cardiovascular benefits appeared independent of baseline HbA1c levels or glycemic changes, highlighting pleiotropic effects in addition to glucose control.48 Therefore, the SELECT trial is the first to establish obesity as a pharmacologically modifiable risk factor for CVD, reinforcing the role of GLP‑1RAs in cardiovascular prevention beyond diabetes management.
Advancement of glucagon‑like peptide‑1 receptor–based multireceptor drugs as emerging obesity therapies for cardiovascular risk reduction
While GLP‑1RAs have revolutionized obesity treatment, their weight loss effects are modest (typically 5%–15%), and cardiovascular benefits are largely mediated by weight reduction and improved glycemic control, although direct cardiovascular effects have also been observed.49
Multireceptor agonists represent a major advancement in obesity pharmacotherapy. By targeting multiple metabolic pathways—such as GLP‑1, glucose‑dependent insulinotropic polypeptide receptor (GIPR), and glucagon receptor (GCGR)—these agents enhance weight loss efficacy, often achieving reductions of 20%–30%, comparable to bariatric surgery (Figures 3 and 4).49 Moreover, GLP‑1R/GIPR coagonists and GLP‑1R/GIPR/GCGR triagonists show promise for improved tolerability, as compared with GLP‑1RAs alone (Figure 4).49 Although both classes share gastrointestinal side effects, including nausea and vomiting, some multireceptor drugs, particularly those incorporating GIPR activation, may attenuate these AEs. The use of multireceptor pharmacology has the potential to drive a paradigm shift in obesity and CVD management, moving beyond monotherapies toward a comprehensive approach to metabolic modulation.
Tirzepatide
Tirzepatide, a dual GIP/GLP‑1RA, demonstrated superior weight loss and metabolic benefits in comparison with placebo and GLP‑1RAs in patients with obesity in the SURMOUNT trials (A Study of Tirzepatide [LY3298176] in Participants with Obesity or Overweight) (Figures 3 and 4).50 In SURMOUNT‑1, a 15‑mg dose of tirzepatide achieved a 22.5% mean body weight reduction (–17.8% vs placebo),51 while SURMOUNT‑2 (which included patients with T2D) showed a substantial weight reduction of about 15% (Figure 3).52 Beyond weight loss, tirzepatide improved atherogenic lipid profiles, lowered blood pressure, enhanced insulin sensitivity, and reduced inflammatory markers (high‑sensitivity CRP [hsCRP]).51,52 The superiority of tirzepatide over semaglutide for weight loss in adults with obesity was confirmed in the SURMOUNT‑5 trial and a real‑world study.53,54 SURMOUNT‑5 showed a 47% greater weight loss with tirzepatide vs semaglutide (a mean difference of 6.5%) over 72 weeks,54 and a 12‑month real‑world study reported a 15.3% average weight loss with tirzepatide vs 8.3% with semaglutide, with a 3.24‑fold greater likelihood of achieving a weight loss of 15% or higher.53
Recent real‑world data on tirzepatide have also provided promising results for its cardiovascular benefits. In a large‑scale cohort study51 (n = 140 308), tirzepatide treatment was associated with a lower risk of MACEs (adjusted HR [AHR], 0.8; 95% CI, 0.71–0.91), all‑cause mortality (AHR, 0.58; 95% CI, 0.45–0.75), and kidney events (AHR, 0.52; 95% CI, 0.37–0.73), as compared with GLP‑1Ras.51 The ongoing SURMOUNT‑MMO trial (A Study of Tirzepatide [LY3298176] on the Reduction on Morbidity and Mortality in Adults with Obesity) is evaluating the safety and efficacy of tirzepatide vs dulaglutide in 12 500 patients with T2D and atherosclerotic CVD (Table 1; ClinicalTrials.gov identifier: NCT05556512).
Recent data highlight an emerging role for tirzepatide in patients with HF. The SUMMIT trial (Study of Tirzepatide in Participants with Heart Failure with Preserved Ejection Fraction and Obesity) assessed tirzepatide in 731 patients with HF with preserved ejection fraction (HFpEF) and obesity (BMI ≥30 kg/m2; left ventricular EF ≥50%) over more than 52 weeks. The primary end point—a composite of death from cardiovascular causes or worsening HF—occurred in 9.9% of the tirzepatide group vs 15.3% of the placebo group (HR, 0.62; P = 0.026). The effectiveness of tirzepatide was mainly due to reduction of worsening HF events (HR, 0.54; P <0.05), while cardiovascular mortality rates were similar between groups. Tirzepatide also improved patient‑reported health status (Kansas City Cardiomyopathy Questionnaire Clinical Summary Score, +19.5 vs +12.7; P <0.001), supporting its role in reducing HFpEF‑related morbidity.55 New data from the SUMMIT trial show that tirzepatide improved hemodynamic, inflammatory, and renal markers in HFpEF and obesity. At 52 weeks, it lowered systolic blood pressure (−5 mm Hg; P <0.001), blood volume (−0.58 l; P <0.001), and CRP level (−37.2%; P <0.001). These changes were associated with improvements in estimated glomerular filtration rate, reduction in albuminuria, and lower levels of myocardial injury markers (troponin T, N‑terminal pro–B‑type natriuretic peptide). These findings reinforce tirzepatide’s role in reducing cardiovascular and kidney damage and HFpEF morbidity.56
Clinical trials suggest that tirzepatide is better tolerated than GLP‑1R monoagonists. A recent systematic review of phase 3 clinical trials and an unadjusted analysis found that tirzepatide 10 and 15 mg had fewer gastrointestinal side effects than semaglutide 2.4 mg, except for diarrhea, supporting its superior tolerability profile.57 Gastric inhibitory polypeptide receptor agonism appears to enhance tolerability of multireceptor drugs by mitigating nausea associated with GLP‑1R activation.49
Safety considerations of glucagon‑like peptide‑1 receptor agonists
Systematic reviews of phase 3 clinical trials highlight potential serious adverse effects of GLP‑1RAs beyond gastrointestinal issues.57 GLP‑1RAs have been linked to a higher risk of acute pancreatitis, though the absolute incidence remains low, and some trials report pancreatic enzyme elevations of unclear significance.57 Preclinical rodent studies associate GLP‑1RAs with thyroid C‑cell hyperplasia and medullary thyroid carcinoma (MTC) risk, though human data remain inconclusive; caution is advised in those with a family history of MTC or multiple endocrine neoplasia type 2.50,57 Semaglutide has been associated with worsening diabetic retinopathy (DR) in SUSTAIN‑6 trial, likely due to rapid glucose reduction,57 and emerging evidence suggests a possible link to nonarteritic anterior ischemic optic neuropathy.50 These risks warrant careful monitoring in individuals with a history of pancreatitis, thyroid malignancy risk, or advanced DR.
Other multireceptor drugs obesity trials
In addition to tirzepatide, several other promising multireceptor agonists are in phase 3 clinical trials for obesity (Figure 3).50 Survodutide, a GLP‑1/GCGR coagonist, has shown significant weight reduction and metabolic benefits (Figure 4).49,50 Another promising agent, maridebart cafraglutide (MariTide), is a dual‑acting therapy combining a GLP‑1RA with a GIP receptor (GIPR) antagonist.50 Administered once monthly, it has demonstrated prolonged effects, with weight loss sustained for up to 150 days after the last dose in clinical studies.58 Retatrutide, a GLP‑1/GIP/GCGR triagonist, has shown unprecedented weight loss of up to 24.2% in a phase 2 trial, with additional benefits in lipid metabolism and glycemic control (Figure 4).49,50
CagriSema, a fixed‑dose combination of cagrilintide (a long‑acting amylin analogue) and semaglutide, has demonstrated superior weight loss efficacy in comparison with other GLP‑1Ras.50 A recent meta‑analysis identified it as the most effective treatment for weight reduction in T2D, with an average loss of 14.03 kg.59 The REDEFINE 1 trial (A Research Study to See How Well CagriSema Helps People with Excess Body Weight Lose Weight) further supported its potential in obesity management, showing a 22.7% weight loss over 68 weeks, outperforming semaglutide (16.1%) and cagrilintide (11.8%), though slightly below Novo Nordisk’s 25% target.60 In REDEFINE 2, assessing CagriSema in T2D, weight loss reached 13.7% (treatment policy estimand) and 15.7% (trial product estimand) vs 3.4% and 3.1% with placebo.61 While confirming superiority over placebo, these results are less pronounced than in the REDEFINE 1, previous expectations, and emerging multireceptor agonist trials.
Cardiovascular benefits of glucagon‑like peptide‑1 receptor agonists: metabolic, antiatherogenic, and anti‑inflammatory effects
The cardiovascular benefits of GLP‑1RAs are multifactorial, encompassing weight reduction, glycemic improvements, and cardiovascular risk modulation. Additionally, semaglutide may exert direct effects on cardiomyocytes, vascular structures, and platelet function while mitigating inflammation and visceral or ectopic fat deposition.62
Weight loss involves complex metabolic adaptations. While a cumulative deficit of 3500 kcal is traditionally estimated to cause 0.45 kg of weight loss, this model does not fully account for body composition changes or compensatory declines in energy expenditure, which promote weight regain.63 GLP‑1RAs play a key role in overcoming these barriers. Secreted by L‑cells in the small intestine, GLP‑1 enhances glucose‑dependent insulin secretion, inhibits hepatic glucose production, delays gastric emptying, and regulates appetite, facilitating sustained weight reduction.63,64
The cardiovascular benefits of GLP‑1RAs extend beyond weight loss and glycemic control, providing direct cardiovascular protection. They improve endothelial function by enhancing nitric oxide bioavailability, activating endothelial nitric oxide synthase, and attenuating angiotensin II signaling, thereby reducing oxidative stress and vascular dysfunction.62 Additionally, GLP‑1RAs improve atherosclerotic plaque stability, suppress monocyte‑macrophage adhesion, and downregulate proinflammatory cytokines (TNF-α, IL‑6, IL‑1β), contributing to anti‑inflammatory and antiatherosclerotic effects.62
In cardiomyocytes, GLP‑1R activation enhances myocardial contractility and cell survival by counteracting reactive oxygen species and mitochondrial dysfunction induced by inflammatory stimuli.62 Furthermore, GLP‑1RAs reduce cardiac hypertrophy through 5'AMP‑activated protein kinase / mammalian target of rapamycin signaling and modulate the renin‑angiotensin‑aldosterone system, contributing to blood pressure reductions observed in clinical trials.62 Notably, emerging evidence highlights that GLP‑1RAs reduce epicardial fat thickness by up to 20%–30%, a key factor in metabolic and CVD progression.62
These findings underscore that GLP‑1RAs provide cardiovascular benefits beyond metabolic improvements, including direct vascular protection and anti‑inflammatory effects. This broad range of actions reinforces their role in obesity and cardiometabolic disease management.
Emerging incretin‑based therapies for metabolic dysfunction–associated steatotic liver disease and cardiovascular risk reduction
Recent trials highlight the potential of GLP‑1RAs and multireceptor incretin therapies in treating MASLD, while also addressing cardiovascular risk.50 A recent Novo Nordisk press release reported positive topline results from part 1 of the phase 3 ESSENCE trial (Research Study on whether Semaglutide Works in People with Non‑alcoholic Steatohepatitis; unpublished work). Weekly semaglutide (2.4 mg) was superior to placebo in resolving MASLD without worsening fibrosis and improving fibrosis without worsening MASLD.65
Several phase 2 trials have also demonstrated promising efficacy. The SYNERGY‑NASH trial (A Study of Tirzepatide [LY3298176] in Participants with Nonalcoholic Steatohepatitis) showed that tirzepatide (a GLP‑1/GIPR coagonist) led to metabolic dysfunction–associated steatohepatitis (MASH) resolution in up to 62% of patients and fibrosis improvement in over a half.66 Similarly, the phase 2b trial of survodutide demonstrated significant reductions in liver fat content and histological improvement of MASH.67 Other dual agonists, such as cotadutide and efinopegdutide, have also shown metabolic and hepatic benefits in early‑stage trials.65 Moreover, studies link GLP‑1RAs with reduced cravings for specific foods and alcohol, likely via dopaminergic pathways.50 This may support their role in managing MASLD by regulating appetite and addictive behaviors.
Given the strong association between MASH and CVD, these findings suggest that incretin‑based therapies could improve both liver and cardiovascular outcomes. However, further phase 3 trials are needed to confirm their long‑term impact.67
Obesity treatment and cardiovascular risk reduction in obstructive sleep apnea
Obstructive sleep apnea (OSA) is prevalent and strongly linked to obesity and increased cardiovascular risk. The recent SURMOUNT‑OSA trial (Obstructive Sleep Apnea Master Protocol GPIF: a Study of Tirzepatide [LY3298176] in Participants with Obstructive Sleep Apnea) demonstrated that tirzepatide significantly reduced the apnea–hypopnea index, body weight, systemic inflammation (hsCRP), and systolic blood pressure in individuals with moderate‑to‑severe OSA and obesity.68 These findings suggest that pharmacologic weight reduction with incretin‑based therapies may improve both respiratory function and cardiovascular risk factors, in addition to the benefits provided by conventional mechanical treatments. Therefore, in December 2024, the FDA approved tirzepatide as the first medication for moderate‑to‑severe OSA in adults with obesity.
Bariatric surgery
Although this paper focuses on pharmacotherapy, bariatric surgery remains crucial for obesity and cardiovascular risk management. Retrospective analyses show that metabolic surgery in patients with T2D reduced MACE incidence by 39%, with procedures including Roux‑en‑Y gastric bypass (63%), sleeve gastrectomy (32%), adjustable gastric banding (5%), and biliopancreatic diversion with duodenal switch (0.04%).69,70 A recent meta‑analysis involving 174 772 participants found that bariatric surgery reduced all‑cause mortality by 59% in obese adults with T2D and by 30% in those without diabetes, extending life expectancy by 9.3 and 5.1 years, respectively.71 In addition to weight loss, Bylica et al72 reported that laparoscopic sleeve gastrectomy improved erythrocyte fatty acid composition, correlating with reduced inflammation and lower cardiovascular risk. Similarly, Cecha et al73 found that bariatric surgery enhanced myocardial work parameters, including global constructive work, EF, and strain, suggesting positive cardiac remodeling.
However, recent attempts to emulate randomized trials using observational data among the United States veterans found no clear reduction in 7‑year cardiovascular risk after bariatric surgery, with risk differences of −0.9% and −1.4%, depending on study design.74 Despite significant BMI and HbA1c reductions, these findings highlight the need for large randomized controlled trials.
Conclusions
Obesity is a modifiable risk factor for CVD, and its management should be integrated into comprehensive cardiometabolic care. While bariatric surgery remains the most effective long‑term intervention, its cardiovascular benefits require further confirmation in randomized trials. The emergence of GLP‑1RAs and multireceptor incretin‑based therapies marks a significant advancement, with semaglutide providing the first evidence of reductions in cardiovascular events in individuals with obesity. Multireceptor agonists—such as tirzepatide and potentially survodutide or retatrutide— demonstrate even greater efficacy in terms of weight loss and metabolic improvement, thereby broadening the therapeutic options. The development of obesity therapies that not only promote weight loss but also positively impact cardiovascular outcomes continues to be a key area of research.
- Płaczkiewicz‑Jankowska E, Czupryniak L, Gajos G, et al. Management of obesity in the times of climate change and COVID‑19: an interdisciplinary expert consensus report. Pol Arch Intern Med. 2022; 132: 16216. | Crossref
- Collaborators GRF. Global burden of 87 risk factors in 204 countries and territories, 1990‑2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020; 396: 1223‑1249.
- Marques A, Peralta M, Naia A, et al. Prevalence of adult overweight and obesity in 20 European countries, 2014. Eur J Public Health. 2018; 28: 295‑300. | Crossref
- Federation WO. World Obesity Atlas. 2023; https://data.worldobesity.org/publications/?cat=19. Accessed February 1, 2025.
- Lange A, Lange N, Jagiełło K, et al. Impact of socioeconomic factors and obesity on visual impairment among older adults in Poland. Pol Arch Intern Med. 2024; 134: 16857. | Crossref
ARTICLE INFORMATION