Thyroid hormone alterations in acute-on-chronic liver failure: a focus on liver transplantation and survival outcomes

 CC BY 4.0
CC BY 4.0
Thyroid hormone alterations in acute-on-chronic liver failure: a focus on liver transplantation and survival outcomes
Introduction
Acute‑on‑chronic liver failure (ACLF) is a severe clinical syndrome characterized by acute hepatic decompensation superimposed on chronic liver disease. It is frequently accompanied by extrahepatic organ failure and has a high short‑term mortality rate exceeding 50% in advanced cases.1-3 Despite considerable progress in understanding its pathophysiology, prognostic assessment and therapeutic strategies remain challenging, particularly where liver transplant (LT) is not possible.1,4 The interplay between systemic endocrine dysfunction and hepatic failure has garnered attention as a potential contributor to disease progression and a source of prognostic biomarkers.5,6
Thyroid hormones, particularly triiodothyronine (T3) and thyroxine (T4), play essential roles in regulating basal metabolic rate, cellular growth, and organ function, including hepatocytes.5,7,8 The liver, in turn, is central to thyroid hormone metabolism, regulating the conversion of T4 into its biologically active form, T3, and the elimination of thyroid hormones via conjugation and excretion.5,9 Dysfunctions in this bidirectional relationship can exacerbate both thyroid and hepatic pathophysiologies.5,10 In the context of ACLF, the dysregulation of thyroid hormone metabolism, often referred to as nonthyroidal illness syndrome (NTIS), is a common finding associated with poor outcomes in various liver diseases.10,11
Emerging evidence underscores the prognostic value of thyroid hormones in ACLF. Reduced levels of free T3 (fT3) and free T4 (fT4) correlate with disease severity and mortality in patients with liver failure.2,3,12 Furthermore, dynamic changes in thyroid hormone levels, particularly fT3, have demonstrated prognostic value in patients with hepatitis B virus–related ACLF.2,8 In contrast, the role of thyroid‑stimulating hormone (TSH) as a prognostic marker remains inconsistent, as some studies indicate its potential utility, while others report no such findings.6,8 These discrepancies highlight the need for further investigation into the prognostic implications of thyroid hormone profiles in ACLF patients.
This study aimed to evaluate the role of thyroid hormones, specifically fT3, fT4, and TSH, as biomarkers of disease severity and mortality in a cohort of ACLF patients, with a particular focus on differences between patients undergoing LT and those receiving standard medical care. By integrating thyroid function assessment into the prognostic evaluation of ACLF, we aimed to provide novel insights into its clinical utility and potential therapeutic implications.
Patients and methods
This retrospective observational study included patients diagnosed with ACLF based on the European Association for the Study of the Liver criteria.13 The patients were either treated at or referred from other centers to a tertiary LT referral center for LT evaluation between 2016 and 2024. Clinical and laboratory data were meticulously collected from patient records, encompassing demographic characteristics, liver disease severity scores, thyroid function tests, and survival outcomes. Initially, 99 patients were identified; however, 4 individuals with previously diagnosed thyroid disorders were excluded to avoid confounding effects on thyroid function assessment. Consequently, 95 patients were included in the final analysis, with 43 patients undergoing LT and 52 patients receiving standard of care (SoC) without transplantation. Patient flowchart is included in Supplementary material, Figure S1.
Venous blood samples were collected from all patients at the time of ACLF diagnosis or upon admission to the tertiary center. Thyroid function was evaluated through the measurements of fT3, fT4, and TSH levels. Liver function parameters, such as bilirubin, creatinine, international normalized ratio (INR), and partial pressure of oxygen (PaO2)/fraction of inspired oxygen (FiO2) ratios were also assessed. To quantify liver disease severity, we utilized the following established prognostic scores: the Model for End‑Stage Liver Disease (MELD), the MELD‑sodium (MELD‑Na), and the Chronic Liver Failure‑Consortium (CLIF‑C) ACLF. The survival and mortality observation period spanned from the time of diagnosis to the point of data collection. The median follow‑up time was 82 days (interquartile range [IQR], 16–1323.3) and the mean (SD) follow‑up duration was 721.1 (953.4 )days.
In collecting, analyzing, and reporting data, we adhered to the ethical standards of the Declaration of Helsinki. Due to the retrospective design of the study, the consent of a bioethics committee was not required. All patient data were anonymized prior to analysis to ensure confidentiality and integrity.
Statistical analysis
Statistical analyses were conducted to compare clinical and biochemical characteristics between the groups. Continuous variables were expressed as medians (IQRs) or means (SDs), depending on the distribution, and compared using the Mann–Whitney test for non‑normally distributed data. Categorical variables were presented as frequencies and percentages, with comparisons performed using the χ2 test or the Fisher exact test, as appropriate. A P value below 0.05 was considered significant.
Results
The study cohort consisted of 95 patients diagnosed with ACLF, at a median age of 52 years (IQR, 42–60). The patients were predominantly men, accounting for 71.6% of the cohort. The distribution of ACLF severity showed that 55.8% of the patients were classified as grade 1 or 2, while the remaining 44.2% were categorized as grade 3.
The median MELD score for the entire cohort was 31.1 (IQR, 26.7–37), and the MELD‑Na score was slightly higher, with a median of 34.8 (IQR, 26.4–46.6). The CLIF‑C ACLF score, reflecting the multiorgan failure burden, had a median value of 51.2 (IQR, 43.1–58.8), highlighting the critical clinical condition of the study population.
Thyroid function parameters demonstrated marked alterations. The median fT3 level was 2.4 pmol/ml (IQR, 1.98–3.08), and fT4 levels were reduced, with a median of 12.6 pmol/ml (IQR, 9.89–16.08). The median TSH level was 1.46 mIU/ml (IQR, 0.73–2.28), indicating NTIS, commonly observed in critical illness. The group characteristis are presented in Supplementary material, Table S1.
Survivors vs nonsurvivors
The cohort was stratified into 2 groups: survivors (n = 48; 50.5%) and nonsurvivors (n = 47; 49.5%). Differences were observed in thyroid hormone levels between the groups. The levels of fT3 were lower in the nonsurvivors (median, 2.13 pmol/ml; IQR, 1.12–5.58) than in the survivors (median, 2.56 pmol/ml; IQR, 1.39–5.04; P = 0.002). Similarly, fT4 levels were also lower in the nonsurvivors (median, 11.49 pmol/ml; IQR, 0–24.9), compared with the survivors (median, 14.68 pmol/ml; IQR, 1.28–22.63; P = 0.03). In contrast, TSH levels did not differ in the 2 groups (P = 0.97), with medians of 1.4 mIU/l (IQR, 0.03–20.7) and 1.54 mIU/l (IQR, 0.01–8.47) for the nonsurvivors and the survivors, respectively (Figure 1).
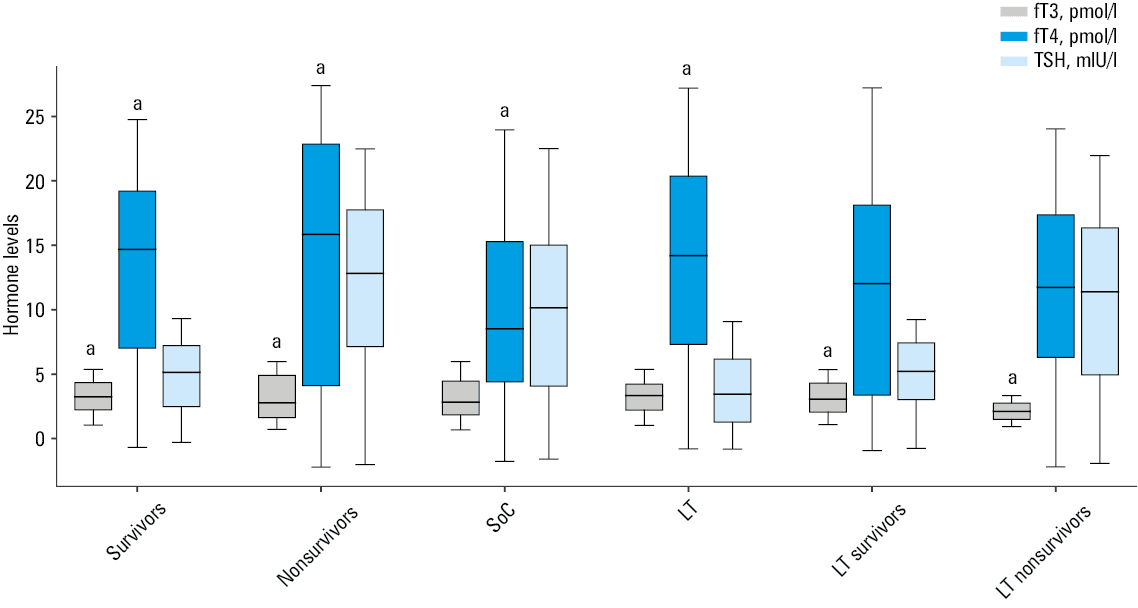
a P <0.05
Abbreviations: Ft3, free triiodothyronine; Ft4, free thyroxine; LT, liver transplant; SOc, standard of care; TSH, thyroid‑stimulating hormone
The parameters reflecting oxygenation and disease severity also showed differences. FiO2 was higher in the nonsurvivors (median, 0.21; IQR, 0.21–0.6) than in the survivors (median, 0.21; IQR, 0.21–0.4; P = 0.005). Although the median values were the same in both groups, the IQR was greater in the nonsurvivors, indicating a higher frequency of elevated FiO₂ values in this group.
Similarly, the PaO2/FiO2 ratio was lower in the nonsurvivors (median, 380.95; IQR, 107.5–576.19), compared with the survivors (median, 400.24; IQR, 162.5–704.76; P = 0.02). The CLIF‑C ACLF score was markedly higher in the nonsurvivors (median, 56.79; IQR, 33.81–78.15) than in the survivors (median, 47.22; IQR, 29.26–63.17; P <0.001; Supplementary material, Table S2).
In contrast, traditional markers of liver dysfunction, including the MELD score (P = 0.15), the MELD‑Na score (P = 0.14), and INR (P = 0.65) did not show differences between the groups. Similarly, albumin levels (P = 0.15) and platelet counts (P = 0.53) were not associated with survival (Supplementary material, Table S2).
Liver transplant vs standard of care
The analysis included 95 individuals with ACLF, divided into 2 groups: patients undergoing LT (n = 43; 45.3%) and those managed with SoC (n = 52; 54.7%).
Thyroid hormone levels showed notable differences between the groups. The levels of fT4 were higher in the LT group (median, 14.63 pmol/ml; IQR, 1.28–24.9) than in the SoC group (median, 11.95 pmol/ml; IQR, 0–22; P = 0.006). However, fT3 levels were comparable between the groups (P = 0.09) (Figure 1).
Differences were observed for several variables. The CLIF‑C ACLF score was markedly lower in the LT group (median, 47.84; IQR, 29.26–67.83), compared with the SoC group (median, 54.36; IQR, 33.81–78.15; P = 0.005). The FiO2 was lower in the LT group (median, 0.21; IQR, 0.21–0.4) than in the SoC group (median, 0.21; IQR, 0.21–0.6; P = 0.003). The greater IQR in the LT group suggests a higher frequency of elevated FiO₂ values. Furthermore, the PaO2/FiO2 ratio was markedly higher in the LT group (median, 400.24; IQR, 107.5–704.76), compared with the SoC group (median, 342.58; IQR, 107.5–576.19; P = 0.03) (Supplementary material, Table S3).
Notably, traditional markers of liver dysfunction, such as the MELD score (P = 0.89), the MELD‑Na score (P = 0.39), and INR (P = 0.21), did not differ between the groups. Age (P = 0.34), platelet counts (P = 0.18), and bilirubin levels (P = 0.92) were also comparable (Supplementary material, Table S3).
Survivors vs nonsurvivors after liver transplant
The analysis included 43 patients with ACLF who underwent LT. The cohort was divided into 2 groups: survivors (n = 34; 79.1%) and nonsurvivors (n = 9; 20.9%).
The levels of fT3 were lower in the nonsurvivors (median, 2.04 pmol/ml; IQR, 1.12–3.14) than inthe survivors (median, 2.57 pmol/ml; IQR, 1.39–5.04; P = 0.05). However, fT4 levels did not differ between the groups (P = 0.83). Additionally, TSH levels were comparable, with no notable differences observed (P = 0.59) (Figure 1).
Among biochemical parameters, bilirubin levels were higher in the nonsurvivors (median, 30.55 mg/dl; IQR, 6.23–41.66), compared with the survivors (median, 13.28 mg/dl; IQR, 2.58–41; P = 0.05). However, parameters such as the MELD score (P = 0.28) and the MELD‑Na score (P = 0.09) did not differ between the groups (Supplementary material, Table S4).
Oxygenation and respiratory variables, such as the PaO2/FiO2 ratio (P = 0.92) and FiO2 (P = 0.32), were not associated with post‑transplant mortality. Similarly, coagulation markers, including INR (P = 0.34), did not show differences (Supplementary material, Table S4).
Interestingly, while the CLIF‑C ACLF score reached higher values in the nonsurvivors (median, 51.59; IQR,42.9–67.83), compared with the survivors (median, 47.22; IQR, 29.26–63.17), this difference was not significant (P = 0.06) (Supplementary material, Table S4).
Discussion
The findings of this study provide noteworthy insights into the prognostic implications of thyroid function alterations in ACLF. The marked reduction in fT3 and fT4 levels, alongside preserved TSH levels, aligns with NTIS. NTIS is characterized by adaptive endocrine responses during critical illness, reflecting reduced peripheral conversion of T4 to T3 via deiodinases. The liver’s role in thyroid hormone metabolism, including the conversion of T4 to T3 and synthesis of thyroid‑binding globulin, provides an explanation of this phenomenon in ACLF patients.4,10 Similar patterns have been reported in both acute and chronic liver diseases, reinforcing the role of NTIS as a hallmark of systemic metabolic disorders in severe hepatic dysfunction.5,6
The differences in fT3 and fT4 levels between the survivors and nonsurvivors underscore their potential as prognostic biomarkers. The fact that the nonsurvivors had lower fT3 levels supports prior studies, demonstrating the correlation between fT3 reductions and poor outcomes in liver failure.3 12 Specifically, reduced fT3 levels have been linked to increased mortality in ACLF caused by hepatitis B virus infection, suggesting that fT3 could be a reliable predictor of the 30- and 90‑day survival.7,12 Interestingly, TSH levels were not associated with survival, which is consistent with findings that TSH alterations have less predictive value in critically ill patients.9
The study highlights differences in clinical and thyroid parameters between patients eligible for LT and those managed with SoC. Before transplant, patients in the LT group had higher fT4 levels and lower CLIF‑C ACLF scores, compared with the SoC group. This suggests that patients selected for transplant had less severe multiorgan failure and relatively preserved thyroid function, potentially reflecting a more favorable prognosis if LT was performed.3 Furthermore, improved oxygenation parameters (eg, higher PaO2/FiO2 ratio) in the LT group suggest better baseline systemic status, compared with the SoC patients. These observations underscore the importance of stratifying patients based on disease severity and thyroid parameters to optimize management strategies.7
The analysis of LT recipients showed that the nonsurvivors had lower fT3 levels than the survivors (median, 2.04 pmol/ml vs 2.57 pmol/ml; P = 0.05). This finding suggests that fT3 levels could serve as a reliable marker for predicting post‑transplant outcomes. While fT4 and TSH levels did not show differences, the relationship between fT3 and survival underlines the critical role of fT3 in metabolic and systemic recovery after transplant. Further studies comparing pre- and post‑LT fT3 levels could offer further insights into this subject. Furthermore, bilirubin levels were higher in the non‑survivors, indicating a potential interaction between unresolved liver dysfunction and endocrine status. The fact that oxygenation and coagulation parameters (eg, PaO2/FiO2 and INR) were comparable between the LT survivors and nonsurvivors (eg, PaO2/FiO2 and INR) further suggests that thyroid dysfunction represents a distinct prognostic pathway in post‑transplant outcomes. These results align with previous studies highlighting fT3 as a key prognostic factor in critical liver disease.8,12
Certain limitations of our study must be acknowledged. Although numerous clinical and laboratory parameters, including thyroid hormone levels, were meticulously collected from patient records, we did not perform a multivariable analysis to integrate them. Further analysis could provide deeper insights into the complex profile of ACLF patients.
Conclusions
The study underscores the importance of incorporating thyroid hormone assessment into ACLF management protocols. Regular monitoring of fT3 and fT4 levels could enhance risk stratification and guide treatment decisions, particularly in determining the need for LT. The association between fT3 levels and survival outcomes, both pre- and post‑transplant, suggests that fT3 monitoring could be integrated into existing scoring systems, such as CLIF‑C ACLF. Future prospective studies should validate these findings across larger cohorts and investigate the correlation between thyroid dysfunction and ACLF severity.
- Bernal W, Jalan R, Quaglia A, et al. Acute‑on‑chronic liver failure. Lancet. 2015; 386: 1576‑1587. | Crossref
- Arroyo V, Moreau R, Jalan R, et al. Acute‑on‑chronic liver failure: a new syndrome that will re‑classify cirrhosis. J Hepatol. 2015; 62: S131‑S143. | Crossref
- Chen JF, Weng WZ, Huang M, et al. The impact of serum thyroid‑stimulation hormone levels on the outcome of hepatitis B virus related acute‑on‑chronic liver failure: an observational study. BMC Gastroenterol. 2022; 22: 330. | Crossref
- Malik R, Hodgson H. The relationship between the thyroid gland and the liver. QJM. 2002; 95: 559‑569. | Crossref
- Marino L, Kim A, Ni B, et al. Thyroid hormone action and liver disease, a complex interplay. Hepatology. 2025; 81: 651‑669. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION