A 77‑year‑old woman presented to a cardiology department with complaints of weakness and heart palpitations. Her medical history included arterial hypertension, hypercholesterolemia, psoriatic arthritis, osteoporosis, and hyperthyroidism at the euthyroid stage. On admission, she was hemodynamically stable. Laboratory tests showed no significant abnormalities. Posteroanterior chest X‑ray showed a mildly dilated cardiac silhouette, and her electrocardiogram demonstrated sinus rhythm without any abnormalities. Holter monitoring detected significant bradycardia with numerous episodes of sinus arrest up to 5 seconds, leading to a diagnosis of symptomatic sick sinus syndrome. Transthoracic echocardiography demonstrated preserved left ventricular ejection fraction and thickening of the interatrial septum (IAS) with an associated mass in the right atrium (Figure 1A). While lipomatous hypertrophy of the IAS (LHIAS) was suspected, other fat‑containing cardiac tumors could not be excluded. For better assessment of the IAS and adjacent structures, transesophageal echocardiography was performed. It demonstrated massive hypertrophy of the IAS measuring 28 mm in midesophageal bicaval view, with a characteristic dumbbell shape (Figure 1B and 1C). Cardiac magnetic resonance (CMR) imaging was used as the optimal modality for evaluating the complex architecture of the IAS. CMR better demonstrated the adipose nature of the mass. Cine CMR reveled an enlargement of the IAS with high signal intensity, similar to subcutaneous fat. The hyperintensity of the tissue was confirmed on T1- and T2‑weighted images, with T2‑weighted images with fat suppression showing hypointensity of the mass. Maximum T1 relaxation time of the mass measured on the T1 map images was 249 ms, confirming the lipomatous nature of the tissue (Figure 1D–1H). Based on these findings, LHIAS diagnosis was confirmed. After ruling out malignant cardiac lesions, a successful pacemaker implantation was performed, and the patient was discharged home in good general condition.
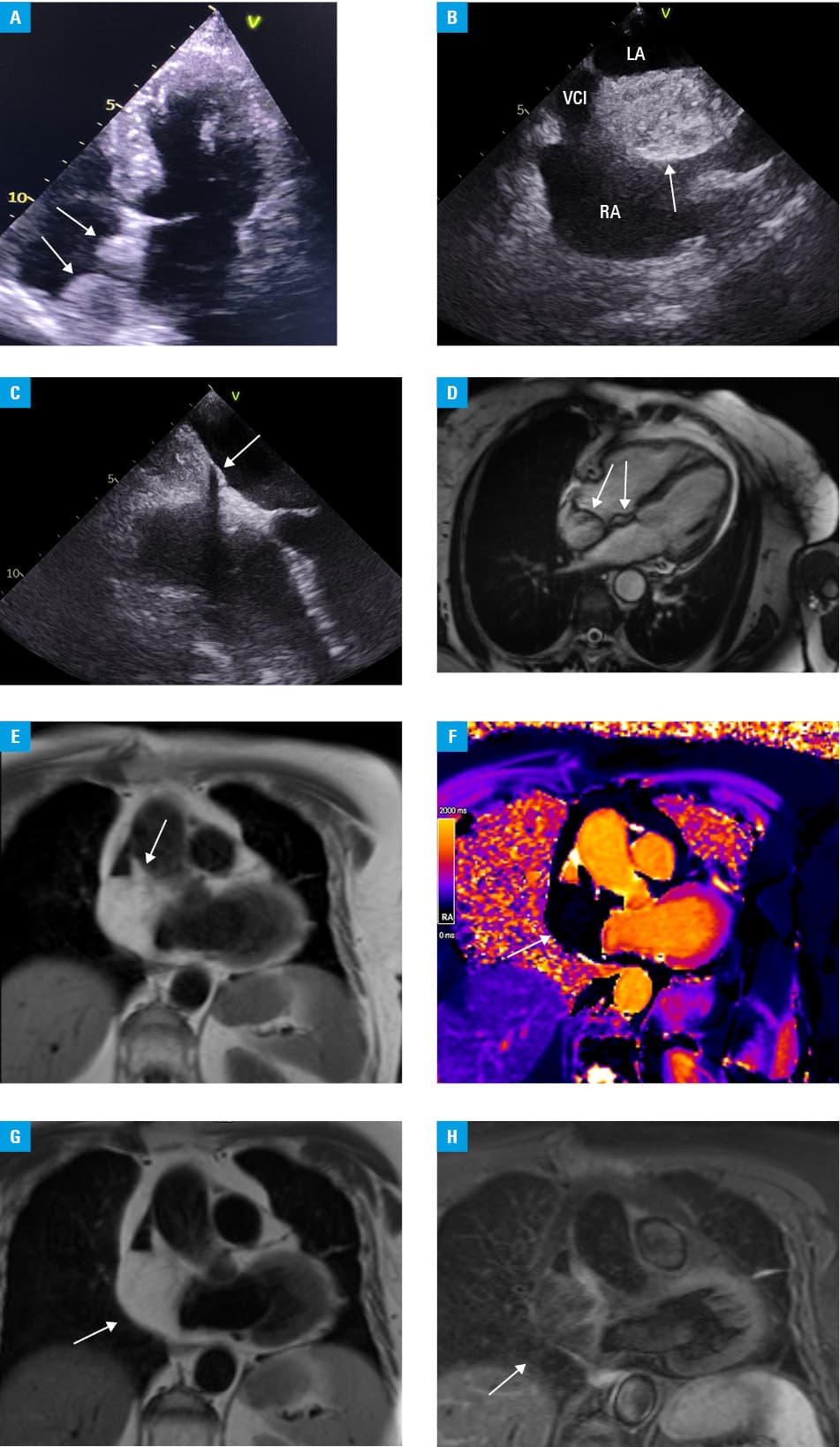
Abbreviations: LA, left atrium; RA, right atrium; VCI, vena cava inferior
A cardiac lesion detected on echocardiography may represent a normal anatomic structure, a benign tumor, or rarely, a malignancy. Therefore, precise lesion characterization is crucial for determining appropriate management. When echocardiography is inconclusive, computed tomography and CMR are often utilized for further evaluation.1 LHIAS is a benign, unencapsulated hyperplasia of lipocytes resembling brown fat in the fold of the septum secundum. It characteristically spares the fossa ovalis, which forms part of the septum primum, creating a typical barbell or dumbbell appearance.1 Although LHIAS is usually an incidental finding and it is asymptomatic, it may be associated with atrial arrhythmias.2 The main differential diagnosis is cardiac lipoma, which is distinguished by its encapsulation and sparse myocyte content. CMR remains the gold standard diagnostic tool.3 Additionally, the presence of metabolically active brown adipose tissue within LHIAS can demonstrate 18F‑fluorodeoxyglucose uptake on positron emission tomography, which can aid in establishing the correct diagnosis.4 Most patients with findings typical of LHIAS on advanced imaging without evidence of structural or arrhythmic complications can be managed conservatively. Surgical management is generally limited to cases in which LHIAS is complicated by serious arrhythmias, superior vena cava syndrome, right atrial obstruction, or hemodynamic derangements leading to congestive heart failure.5
- Tagliati C, Fogante M, Palmisano A, et al. Cardiac masses and pseudomasses: an overview about diagnostic imaging and clinical background. Medicina (Kaunas). 2023; 60: 70. | Crossref
- Yavar Z, Gilge JL, Patel PJ, et al. Lipomatous hypertrophy of the interatrial septum manifesting as third degree atrioventricular block. JACC Case Rep. 2020; 2: 2235‑2239. | Crossref
- Fussen S, De Boeck BWL, Zellweger MJ, et al. Cardiovascular magnetic resonance imaging for diagnosis and clinical management of suspected cardiac masses and tumours. Eur Heart J. 2011; 32: 1551‑1560. | Crossref
- Siminiak N, Rajewska‑Tabor J, Pyda M, et al. Changing appearance of lipomatous hypertrophy of the interatrial septum on positron emission tomography scan. Kardiol Pol. 2021; 79: 1032‑1033. | Crossref
- Zeebregts CJ, Hensens AG, Timmermans J, et al. Lipomatous hypertrophy of the interatrial septum: indication for surgery? Eur J Cardiothorac Surg. 1997; 11: 785‑787. | Crossref
ARTICLE INFORMATION