“Double diabetes?” Diagnostic and therapeutic challenges in a patient with established type 1 diabetes mellitus, developing features of type 2 diabetes mellitus

 CC BY 4.0
CC BY 4.0
“Double diabetes?” Diagnostic and therapeutic challenges in a patient with established type 1 diabetes mellitus, developing features of type 2 diabetes mellitus
Diabetes mellitus encompasses metabolic disorders characterized by elevated blood glucose due to issues with insulin production and function. In type 1 diabetes mellitus (T1DM), autoimmune destruction of pancreatic β-cells is the primary cause, while in type 2 DM (T2DM), the condition arises from a progressive decline in insulin secretion and resistance.1-3
This report presents a case of a 32‑year‑old man diagnosed with T1DM at the age of 12, who, 17 years later, was also diagnosed with T2DM. In 2005, the patient was referred to a hospital with symptoms of lethargy, vomiting, fatigue, polyuria, polydipsia, and elevated fasting blood glucose (serum glucose >600 mg/dl; reference range, 59–100 mg/dl). A diagnosis of T1DM was confirmed based on the presence of autoantibodies, and the treatment with subcutaneous aspart insulin (Novorapid) at a dosage of 20 IU/ml before meals and subcutaneous isophane insulin (Insulatard) at a dosage of 30–40 IU/ml at night was started. Despite the administration of high doses of insulin, diabetes was not controlled well, and body mass index (BMI) remained high at 40.22 kg/m².
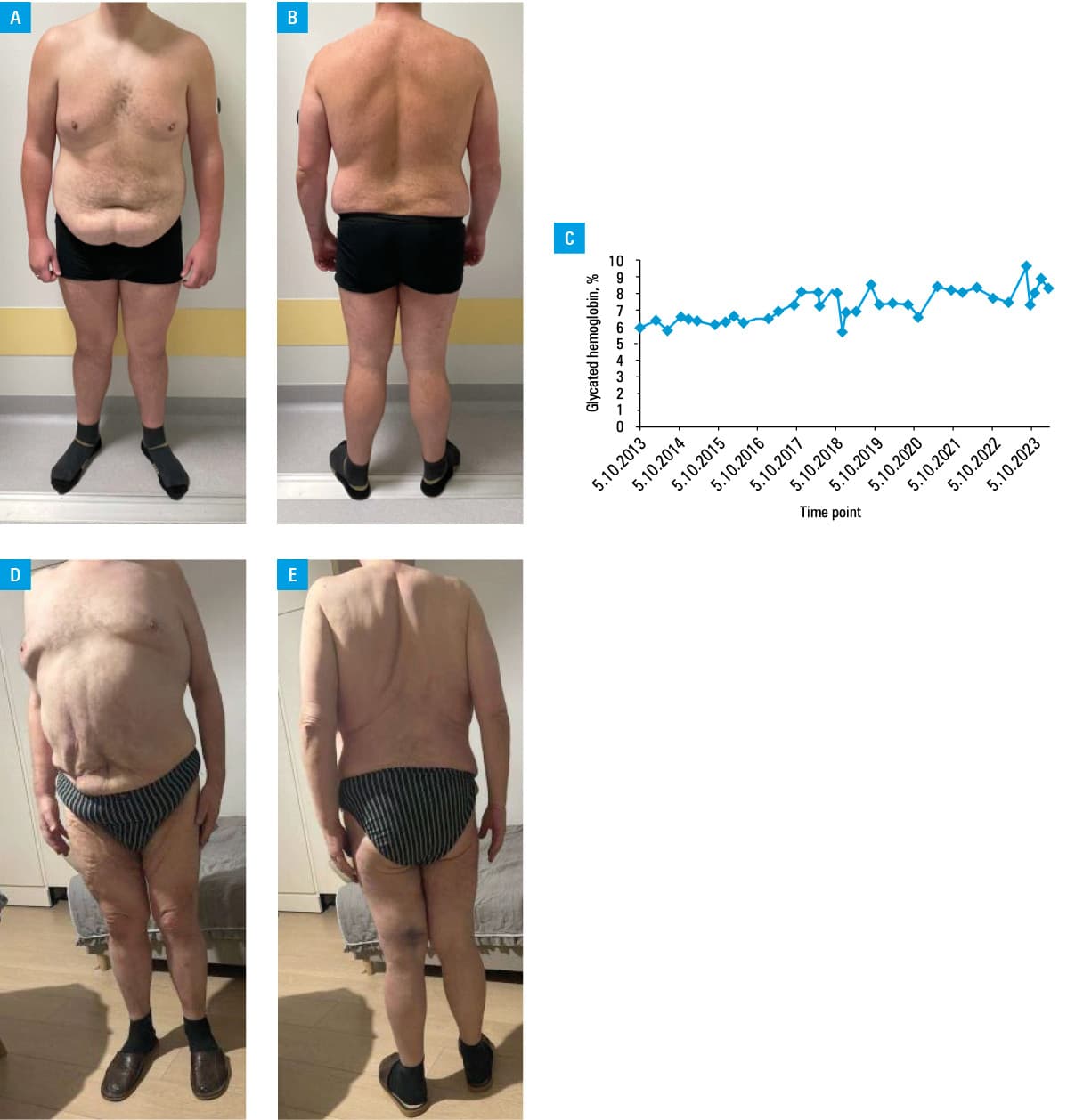
At this point, the diagnosis of T2DM was formally added to the primary diagnosis of T1DM, due the presence of insulin resistance, obesity, hypertension, hypercholesterolemia, and family history of T2DM. The patient’s insulin therapy was modified. Novorapid was substituted with subcutaneous Fiasp (30–60 IU/ml), and isophane insulin was replaced with subcutaneous insulin glargine (30–60 IU/ml; Toujeo). The treatment regimen was augmented with the addition of oral metformin (Glucophage) at a dosage of 1000 mg (once daily), oral empagliflozin (Jardiance) at 5 mg (once daily), and subcutaneous semaglutide (Ozempic) at 0.5 mg (once a week). In 2023, the dosage of semaglutide was increased to 1 mg, and in 2024 to 1.5 mg. Two years following the implementation of the mentioned treatment modifications, the patient’s BMI declined notably, from 40.22 to 33.9 kg/m² (Figure 1A and 1B), and the most recent glycated hemoglobin level was 8.3% (Figure 1C).
The term “double diabetes” is not formally defined. However, it is applied to patients with T1DM who also exhibit T2DM traits, such as obesity, family history of T2DM, insulin resistance, hypertension, or metabolic syndrome.4 The question arises as to whether these features result from overinsulinization. Nevertheless, the patient’s high insulin needs from the first year suggest primary insulin resistance. Consequently, this case likely represents true double diabetes.
Olamoyegun et al5 described a case of a 17‑year‑old woman who developed T2DM 6 years after a diagnosis of T1DM. The patient presented with primary symptoms including weight gain and acanthosis in the neck and axillae. In contrast to our patient, she did not have a family history of T2DM, although 2 of her siblings had been diagnosed with T1DM. The treatment regimen included metformin, but not empagliflozin or semaglutide. This case demonstrates the importance of monitoring T1DM patients with T2DM family history, as early detection facilitates treatment optimization and improves outcomes.
The images above present our patient (T1DM/T2DM; Figure 1A and 1B) and his father (T2DM; Figure 1D and 1E), both obese with similar fat distribution.
- Petersmann A, Müller‑Wieland D, Müller UA, et al. Definition, classification and diagnosis of diabetes mellitus. Exp Clin Endocrinol Diabetes. 2019; 127: S1‑S7. | Crossref
- Zieleniewska NA, Szum‑Jakubowska A, Chlabicz M, et al. The prevalence of diabetes and prediabetes: a population‑based study. Pol Arch Intern Med. 2023; 133: 16407. | Crossref
- Gregory GA, Robinson TIG, Linklater SE, et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: a modelling study. Lancet Diabetes Endocrinol. 2022; 10: 741‑760. | Crossref
- Bielka W, Przezak A, Molęda P, et al. Double diabetes—when type 1 diabetes meets type 2 diabetes: definition, pathogenesis and recognition. Cardiovasc Diabetol. 2024; 23: 62. | Crossref
- Olamoyegun MA, Ala OA, Ugwu E. Coexistence of type 1 and type 2 diabetes mellitus: a case report of “double” diabetes in a 17‑year‑old Nigerian girl. Pan Afr Med J. 2020; 37: 35. | Crossref
ARTICLE INFORMATION