Beyond a broken heart: a case of intraventricular thrombus formation in a patient with Takotsubo syndrome



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Beyond a broken heart: a case of intraventricular thrombus formation in a patient with Takotsubo syndrome
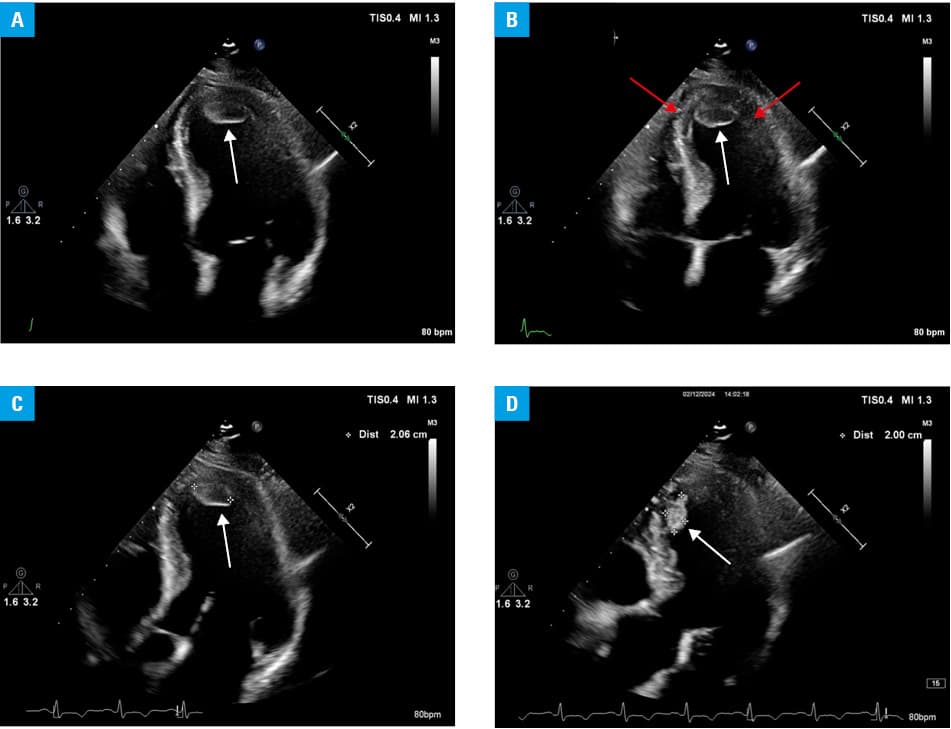
A 44‑year‑old woman with a medical history of untreated hypertension, active nicotine use, congenital adrenal hyperplasia, type 2 diabetes, and obesity, was admitted to a hospital with chest pain. She reported several days of recurrent left subcostal pain that was initially relieved with drotaverine, but became persistent on the morning of admission. The patient denied any recent stressful events; however, she admitted a high level of chronic occupational stress. Laboratory tests performed on admission and on the second day of hispitalization showed elevated levels of cardiac troponin I (0.296 and 0.899 ng/ml; reference range [RR] ≤0.06 ng/ml), N‑terminal pro–B‑type natriuretic peptide (4642 pg/ml; RR ≤125 pg/ml), glucose (297 mg/dl; RR, 70–140 mg/dl), C‑reactive protein (29.3 mg/l; RR, 0–5 mg/l), and D‑dimer (1332 μg/ml; RR <0.5 μg/ml). A 12‑lead electrocardiogram showed ST‑segment depression in leads I, aVL, V5, and V6. Urgent cardiac catheterization did not indicate significant coronary stenosis, with no slow‑flow present, and subsequent left ventriculography demonstrated hypokinesis of the apical segments, characteristic of Takotsubo syndrome (TTS). Transthoracic echocardiography (TTE) identified akinesis of the mid and apical segments of the anterior left ventricular (LV) wall, hypokinesis of the apex and apical segments of all the other LV walls, preserved right ventricular systolic function, mild tricuspid regurgitation, and 2 apical LV thrombi, measuring 20 mm × 13 mm and 20 mm × 11 mm (Figure 1). Left ventricular ejection fraction (LVEF) was estimated at 40%. The patient was transferred to an intensive care unit where continuous intravenous heparin was administered to prevent thromboembolism. Serial echocardiographic assessments were performed at intervals of 2–3 days. By day 10, TTE showed 1 mobile apical thrombus (11 mm × 12 mm) and improved LVEF, estimated at 55%. Cardiovascular surgeons qualified the patient for conservative intraventricular thrombus treatment. Due to congenital adrenal hyperplasia and clinical symptoms of Cushing syndrome, the patient underwent computed tomography of the adrenal glands (unremarkable) and the low‑dose dexamethasone suppression test (inconclusive result). She received diabetes treatment according to the recommendations of the Polish Diabetes Association.1 Last TTE performed after 17 days of hospitalization demonstrated complete resolution of the wall motion abnormalities (LVEF, 52%) with no signs of intraventricular thrombus. The patient was discharged on oral anticoagulation therapy (apixaban) and referred for further thrombophilia screening, the result of which is not yet available. Cardiac resonance performed 2 weeks after discharge showed no signs of active myocarditis (LVEF, 59%). TTE performed during the 4‑week follow‑up visit identified no residual LV dysfunction (LVEF, 59%) and no signs of intraventricular thrombi.
TTS predominantly affects postmenopausal women, but it is known that men (even younger men as our patient) can also develop this condition.2-4 According to the German Italian Stress Cardiomyopathy Registry, 12 out of 541 TTS patients (2.2%) developed LV thrombi, with the youngest one being 61 years old at the time of diagnosis.5 Formation of intraventricular thrombi is one of the rarest TTS complications, with incidence reate of approximately 2% within 6 months, and rising to 8% within 5 years, occasionally leading to further thromboembolic events, including cerebral ischemic stroke or arterial embolism.2-4 This case underscores the importance of continuous echocardiographic monitoring in patients with TTS, particularly those with extensive regional wall motion abnormalities. Anticoagulant therapy plays a pivotal role in preventing thromboembolic complications and ensuring thrombus resolution. Oral anticoagulation is generally recommended if an intraventricular thrombus is detected in the absence of high bleeding risk.4 However, the role of prophylactic anticoagulation is yet to be determined, and therapeutic low‑molecular‑weight heparin can be considered in the cases with extensive segmental akinesia or atrial fibrillation.4,6
- Clinical guidelines on diabetes management ‑ 2024. Position statement of the Polish Diabetes Association [in Polish]. Curr Top Diabetes. 2023; 4.
- Templin C, Ghadri JR, Diekmann J, et al. Clinical features and outcomes of takotsubo (stress) cardiomyopathy. N Engl J Med. 2015; 373: 929‑938.
- Budnik M, Opolski G. Takotsubo syndrome [in Polish]. Warszawa: Item Publishing; 2019: 76‑77.
- Lyon AR, Bossone E, Schneider B, et al. Current state of knowledge on Takotsubo syndrome: a position statement from the taskforce on Takotsubo syndrome of the Heart Failure Association of The European Society of Cardiology. Eur J Heart Fail. 2016; 18: 8‑27. | Crossref
- Santoro F, Stiermaier T, Tarantino N, et al. Left ventricular thrombi in Takotsubo syndrome: incidence, predictors, and management: results from the GEIST (German Italian Stress Cardiomyopathy) Registry. J Am Heart Assoc. 2017; 6: 12 | Crossref
ARTICLE INFORMATION