Left ventricular pseudoaneurysm as a complication of silent myocardial infarction in a patient with a history of pulmonary sarcoidosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Left ventricular pseudoaneurysm as a complication of silent myocardial infarction in a patient with a history of pulmonary sarcoidosis
Left ventricular pseudoaneurysms (LVPAs) are rare findings, typically arising from myocardial infarctions (MIs) or vascular interventions. Factors contributing to the formation of LVPA include steroid treatment, hypertension, infection, inflammation, and trauma.1 Even in asymptomatic cases, there is a significant risk of life‑threatening conditions, such as PA rupture, which can lead to hemorrhage, cardiogenic shock, and thromboembolic complications. Therefore, prompt treatment is essential.2
A 65‑year‑old asymptomatic man with type 2 diabetes on insulin therapy and a history of sarcoidosis was admitted to a hospital due to a suspicion of a lung tumor. Control chest X‑ray identified a round shadow measuring 70 mm × 60 mm in the lower field of the left lung, partially obscured by the silhouette of the heart (Figure 1A).
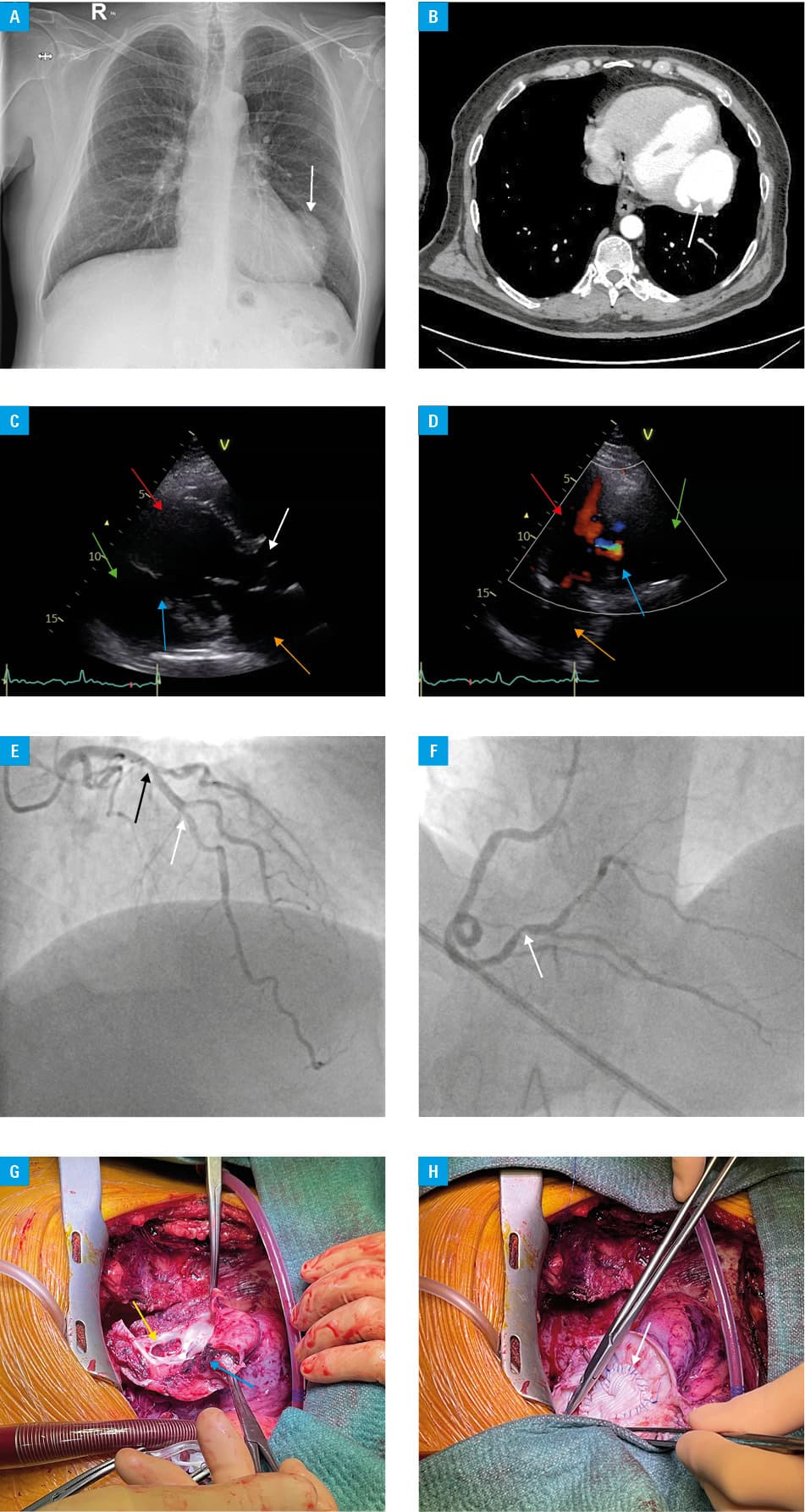
Computed tomography showed a massive false aneurysm measuring 74 mm × 48 mm × 73 mm in the posterior wall of the left ventricle (LV; Figure 1B), numerous nodular changes with accompanying fibrosis, and enlarged surrounding lymph nodes.
Echocardiography identified hypokinesis of the basal segment of the posterior wall of the LV, an akinetic middle segment with scar tissue, a massive PA with thrombus (20 mm × 20 mm), and a visible flow into the LV cavity (Figure 1C and 1D).
Coronary angiography showed multivessel coronary disease (MVD) with multiple stenoses in the left main coronary artery (by 40%), left anterior descending artery (LAD; by 30%; Figure 1E), and the dominant right coronary artery (RCA; by 70%, Figure 1F). The fractional flow reserve of the RCA and LAD showed values of 0.8. Based on the clinical picture, MI of the inferolateral wall, caused by RCA stenosis, was suspected as the most probable cause of PA.
The patient was qualified for intraventricular LV reconstruction using a round patch (Dor procedure) with coronary artery bypass grafting to the posterior descending artery. The PA was excised, and the LV was repaired using a Dacron patch (Figure 1G and 1H).
The postoperative course and wound healing were uneventful, and the patient was discharged home in a good general condition.
While true aneurysms usually involve the anterior wall, false aneurysms are commonly located on the inferolateral wall of the LV, representing only 2% of postinfarction aneurysms.3 These structures develop due to a small rupture in the ventricular wall. The surrounding tissues exert pressure at the rupture site, preventing tamponade and potential death. Instead, a thrombus forms. PAs can be a result of a silent heart attack, which is a common life‑threatening condition, accounting for up to 50% of all MIs. Silent myocardial ischemia is considerably more frequent in patients with diabetes.4
Patients of advanced age with multimorbidity, including diabetes, hypertension, and MVD, often show vascular frailty, which makes them particularly susceptible to the development of PAs. These aneurysms can remain undetected and, consequently, untreated for prolonged periods, significantly raising the risk of mortality. The 1‑year risk of rupture for untreated LVPA is approximately 40%.5 Therefore, regular follow‑up examinations for patients at a high risk of cardiovascular events is crucial for detecting early complications, even in asymptomatic cases, as illustrated in this example.
- Torchio F, Garatti A, Ronco D, et al. Left ventricular pseudoaneurysm: the niche of post‑infarction mechanical complications. Ann Cardiothorac Surg. 2022; 11: 290‑298. | Crossref
- Zachwyc J, Kobusiak‑Prokopowicz M, Guziński M, et al. An unusual long‑term follow‑up of a patient with a left ventricular pseudoaneurysm after myocardial infarction. Kardiol Pol. 2024; 82: 239‑240. | Crossref
- Kaźmierski M, Korzeniowska B, Jaskuła W, et al. Large post‑infarction left ventricular aneurysm. Folia Cardiol Excerpta. 2005; 12: 315‑319.
- Cosson E, Attali JR, Valensi P. Markers for silent myocardial ischemia in diabetes: are they helpful? Diabetes Metab. 2005; 31: 205‑213. | Crossref
- Subban V, Kurian VM, Ajit MS, et al. Hybrid trans‑apical device closure of left ventricular pseudoaneurysm under trans‑oesophageal echocardiographic guidance. Heart Lung Circ. 2012; 21: 734‑736. | Crossref
ARTICLE INFORMATION