Safety and outcomes of endovascular treatment with stent implantation in patients with malignant superior vena cava syndrome: single-center experience
Key words: endovascular treatment, malignancy, superior vena cava syndrome

 CC BY 4.0
CC BY 4.0
Safety and outcomes of endovascular treatment with stent implantation in patients with malignant superior vena cava syndrome: single-center experience
Introduction: Superior vena cava syndrome (SVCS) comprises a range of symptoms and signs of mechanical obstruction of the SVC lumen.
Objectives: The study aimed to investigate the effectiveness and safety of endovascular treatment (EVT) with stent implantation in patients with SVCS due to malignancy.
Patients and methods: This retrospective observational study included patients with malignant SVCS who received EVT with stent implantation between July 2014 and November 2024. The efficacy of the procedure was evaluated based on technical success, clinical symptom relief, periprocedural complication rate, and recurrence rate, with follow‑up conducted 1 month postprocedure.
Results: A total of 56 stents were implanted in 40 patients (57.5% women) in 47 procedures. Thirty‑three patients (81.5%) underwent conventional anticancer treatment prior to the procedure (previously treated patients [PTPs]) and 7 (17.5%) were naive to prior anticancer treatment (not previously treated patients [NPTPs]). The EVT with stent implantation was technically successful in 39 patients (97.5%). At least moderate reduction in symptoms was observed in 81.8% of the individuals in the PTP group and in 85.7% in the NPTP group (P = 0.67). In 28 patients (70%), only 1 stent was required. The overall complication rate was 12.5%. The primary stent patency rate was 92.3% (90.6% vs 100%; P = 0.41 for the PTP vs NPTP group, respectively).
Conclusions: The EVT with stent placement is effective in symptomatic patients with SVCS due to malignancy. The procedure is associated with acceptable complication and reocclusion rates.
What's new?
As there is a paucity of societal guidelines regarding management of superior vena cava syndrome due to malignancy, this paper provides new evidence on high effectiveness and safety of balloon angioplasty with stent implantation. The endovascular treatment was equally effective in anticancer treatment–naive patients and patients who previously received chemotherapy or radiotherapy. The endovascular approach provided an immediate reduction of pressure gradient through the stenosis and a significant reduction of clinical symptoms in the following hours. The primary stent patency rate was 92.3%, and the overall complication rate was 12.5%. The paper updates the committed physicians and interventionalists taking care of patients suffering from this life‑threatening condition on possible therapeutic options.
Introduction
Superior vena cava syndrome (SVCS) encompasses a range of clinically relevant symptoms and signs of complete or partial mechanical obstruction of the SVC lumen.1,2 This may occur as a result of external compression, vascular neoplastic invasion, or thrombus‑induced internal occlusion. SVC obstruction typically causes an increase in venous pressure proximal to the lesion, therefore leading to congestion in the head and upper extremities. Currently, approximately 70% of cases are caused by malignancy, whereas benign disorders, such as catheter‑related thrombosis, are responsible for the remaining 30%.2-4 The most common malignant causes include small cell lung cancer (SCLC) and non‑SCLC (NSCLC).2 Typical symptoms and signs of SVCS may vary significantly, from conditions such as head and neck edema and orthopnea to life‑threatening airway obstruction, stupor, and coma, if left untreated.1 Thus, the primary objective of SVCS management is symptom relief. Over the last 2 decades, there have been considerable advances in the management of patients with SVCS. Until recently, the basis of treatment was radiation therapy, which had an effectiveness rate of only about 70%. Currently, endovascular treatment (EVT) with or without stent implantation is the primary therapy for most patients, especially those with malignant SVC obstruction.5 Although observational data published to date point to a significant technical achievement with a high rate of symptomatic relief in patients treated endovascularly, there is still a considerable paucity of data and clinical guidelines concerning the EVT of malignant SVCS. In this study, we investigated the safety and outcomes of EVT with stent implantation in the oncology population with SVCS.
Patients and methods
Patient recruitment and data recording
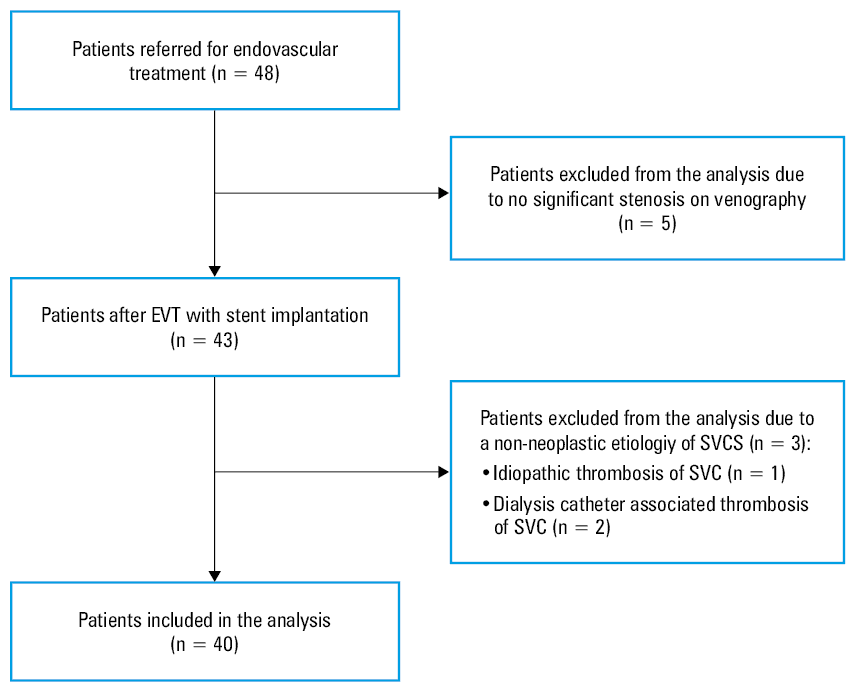
This single‑center, observational, retrospective study included patients with active malignancy who had EVT with stent implantation due to SVCS conducted in a cardiology unit between July 2014 and November 2024. The hospital database was examined for all consecutive patients discharged following the implementation of EVT for SVCS. The active malignancy was specified as 1) current requirement for anticancer therapy or 2) at least qualification for such a therapy within the previous 30 days, as well as 3) disqualification from anticancer treatment due to a lack of further therapeutic options. The exclusion criteria were: 1) the absence of a significant stenosis in the SVC on venography and / or 2) a non‑neoplastic etiology of SVCS. The flowchart for patient enrolment is presented in Figure 1. Baseline characteristics were recorded for each confirmed case, including patient demographics, comorbidities, the type of cancer, anticancer treatment that had been received, and the type of SVC occlusion in accordance with the Stanford and Doty Classification.6 Clinical symptoms were recorded before the procedure in accordance with the Kishi scoring system, and indications for stent implantation were defined as the Kishi score above 4.7 Symptom assessment, including the Kishi scoring system, was conducted 48 hours after the procedure to evaluate the clinical improvement. Improvement in clinical symptoms was defined as follows: 1) complete relief, no symptoms of SVCS; 2) moderate relief, still symptomatic with improvement in the Kishi score by more than 2 points; 3) mild relief, still symptomatic and improvement in the Kishi score of 2 points or less; and 4) no clinical change. Outcome measures specific to stent implantation, including complication rate during the procedure, were noted. After the procedure, the patients were followed‑up for 30 days for recurrent reocclusion and / or death. All the information was derived from medical records with all their limitations.
Procedural details
The stents were implanted following a routine protocol as detailed below. The procedure was performed under local anesthesia. In all cases, a combination of the right transjugular and right transfemoral access was successfully obtained under ultrasound guidance. First, venography was performed to accurately assess the stenosis and to select the optimal stent length and diameter. Vessel diameter and length, as well as significance of the stenosis were assessed on intravascular ultrasound examination (Philips Volcano Eagle Eye or Philips Volcano P18, San Diego, California, United States). In the case of tight stenosis, predilatation with a balloon catheter was performed. The following self‑expanding stents were used: Zilver 635 (Cook Medical, Bloomington, Indiana, United States), S.M.A.R.T Control (Cordis Corp., Miami, Florida, United States), and Venovo (Becton Dickinson, Franklin Lakes, New York, United States). Technical success was defined according to the Society of Interventional Radiology guidelines,8 as the full coverage of the stenosis (the stent extending 10 mm beyond the edges of the stenosis on both sides). A routine postdilatation procedure with a balloon catheter was performed following placement of the stent in order to guarantee proper stent apposition. In all patients, pressure measurements in the SVC were performed before and after the stent implantation. All patients were administered 3000 IU of unfractionated heparin during the procedure. After the procedure, all patients received low‑molecular‑weight heparin (LMWH) at 1 mg/kg on a continuous basis.
Statistical analysis
IBM SPSS Statistics package, version 27.0 (IBM, Sheffield, United Kingdom) was applied for statistical analysis. The results for categorical variables were expressed as numbers and percentages, while for continuous variables they were reported as mean and SD or median with interquartile range (IQR), depending on the type of distribution. The t test was used for continuous variables with a normal distribution, while the Mann–Whitney test was applied for those without a normal distribution, to determine the differences between the groups. The Fisher exact test was applied for all contingency Tables (both 2 × 2 and those with more than 2 categories), to establish group differences. In the cases involving paired data, the Wilcoxon matched‑pairs test was conducted to evaluate the significance of the observed differences (eg, blood pressure measurements before and after the procedure). A P value below 0.05 was considered significant.
Results
Patient characteristics
A total of 48 consecutive patients with SVCS underwent EVT with stent implantation between July 2014 and November 2024 at the Department of Pulmonary Circulation, Thromboembolic Diseases and Cardiology at the European Health Center in Otwock. All patients were referred to our center for interventional treatment of SVCS. After exclusions, 40 patients were included in the analysis. A total of 56 stents were implanted in 47 procedures performed in patients with malignancy.
The most prevalent causes of SVCS in the whole study population were NSCLC (67.5%) and SCLC (20%). The majority of patients (60.6%) were at stage 3B or 4 of the disease, whereas all patients with SCLC had an extensive stage of the disease. There were 33 patients (82.5%) who had previously received anticancer treatment (previously treated patients [PTP]) and 7 patients (17.5%) who had not received any anticancer treatment prior to the procedure (not previously treated patients [NPTP]). The PTP group received the following anticancer treatment: 60.6% were treated with both chemotherapy and radiotherapy, 30.3% with chemotherapy alone, and 9.1% with radiotherapy alone. More than 80% of the patients were treated pharmacologically for SVCS, of those, 54.5% received both glucocorticosteroids and diuretics, 12.1% received only diuretics, and 33.3% received only glucocorticosteroids. Thirty‑seven participants (92.5%) received a prophylactic dose of LMWH. There were no significant discrepancies in cancer stage between the PTP and NPTP groups.
In 18 cases (45%) obstruction concerned a single vessel (SVC in 15 cases, right or left brachiocephalic vein [BCV] in 3 cases), in 20 cases (50%) obstruction concerned 1 BCV and SVC, and in 2 cases (5%) both BCVs and SVC were obstructed. All patients in the NPTP group had obstruction involving 2 vessels (SVC and 1 BCV). A summary of all baseline patient parameters is presented in Table 1.
Characteristics | Overall (n = 40) | Previous anticancer treatment (n = 33) | No previous anticancer treatment (n = 7) | P value |
Data are presented as number (percentage) or mean (SD).
Abbreviations: GCS, glucocorticosteroid; ED, extensive disease; NSCLC, non–small‑cell lung cancer; SCLC, small‑cell lung cancer; others, see Figure 1 | ||||
Men | 17 (42.5) | 12 (36.4) | 5 (71.4) | 0.11 |
Women | 23 (57.5) | 21 (63.6) | 2 (28.6) | |
Age, y, mean (SD) | 63.3 (9.4) | 63.2 (9) | 63.9 (11.9) | 0.17 |
Comorbidities | ||||
Nicotinism | 19 (47.5) | 15 (45.5) | 4 (57.2) | 0.69 |
Hypertension | 12 (30) | 9 (27.3) | 3 (42.9) | 0.41 |
Chronic kidney disease | 8 (20) | 5 (15.2) | 3 (42.9) | 0.13 |
Diabetes mellitus | 6 (15) | 3 (6.8) | 3 (42.9) | 0.06 |
Atrial fibrillation | 4 (10) | 1 (3) | 3 (42.9) | 0.01 |
Obesity | 4 (10) | 2 (6.1) | 2 (28.6) | 0.13 |
Coronary disease | 3 (7.5) | 0 | 3 (42.9) | 0.01 |
Heart failure | 2 (5) | 1 (3) | 1 (14.3) | 0.32 |
Chronic obstructive pulmonary disease | 2 (5) | 1 (3) | 1 (14.3) | 0.32 |
Tumor type | ||||
Lung cancer | 35 (87.5) | 29 (87.9) | 6 (85.7) | >0.99 |
NSCLC | 27 (67.5) | 21 (63.6) | 6 (85.7) | 0.39 |
SCLC | 8 (20) | 8 (24.2) | 0 | 0.31 |
Thymus cancer | 3 (7.5) | 2 (6.9) | 1 (14.3) | 0.49 |
Metastases | ||||
Colon | 2 (5) | 2 (6.1) | 0 | >0.99 |
Unknown primary | 2 (5) | 2 (6.1) | 0 | >0.99 |
Tumor stage | ||||
3A | 6 (15) | 4 (12.1) | 2 (28.6) | 0.28 |
3B | 7 (17.5) | 7 (21.2) | 0 | 0.32 |
3C | 6 (15) | 4 (12.1) | 2 (28.6) | 0.28 |
4 | 13 (32.5) | 10 (30.3) | 3 (42.9) | 0.66 |
ED (SCLC) | 8 (20) | 8 (24.2) | 0 | 0.31 |
Medical treatment of SVCS | ||||
None | 7 (17.5) | 7 (21.2) | 0 | – |
GCS | 11 (27.5) | 10 (30.3) | 1 (14.3) | |
Diuretics | 4 (10) | 4 (12.1) | 0 | |
GCS + diuretics | 18 (45) | 12 (36.4) | 6 (85.7) | |
Anticoagulation | 37 (92.5) | 30 (90.9) | 7 (100) | – |
Stanford classification | ||||
Grade 1 | 0 | 0 | 0 | – |
Grade 2 | 27 (67.5) | 23 (69.7) | 4 (57.1) | 0.41 |
Grade 3 | 9 (22.5) | 6 (18.2) | 3 (42.9) | |
Grade 4 | 4 (10) | 4 (12.1) | 0 | |
The median (IQR) Kishi score in the studied population was 6 (6–7), and there was no difference in the Kishi score between the PTP and NPTP groups (6 [6–7] vs 7 [6–8], respectively; P = 0.13). The symptoms of SVCS along with the frequency of their occurrence are presented in Table 2.
Symptoms of SVCS | Overall (n = 40) | Previous anticancer treatment (n = 33) | No previous anticancer treatment (n = 7) | P value |
Data are presented as number (percentage) or median (interquartile range).
Abbreviations: see Figure 1 | ||||
Kishi score before EVT | 6 (6–7) | 6 (6–7) | 7 (6–8) | 0.13 |
Facial swelling | 35 (87.5) | 29 (87.9) | 6 (85.7) | >0.99 |
Upper extremity swelling | 15 (37.5) | 13 (39.4) | 2 (28.6) | 0.69 |
Neck vein or arm vein distention, upper body plethora | 18 (45) | 14 (42.4) | 4 (57.1) | 0.68 |
Neurologic symptoms | 9 (22.5) | 7 (21.2) | 2 (28.6) | 0.65 |
Cough | 2 (5) | 2 (6.1) | 0 | >0.99 |
Shortness of breath | 27 (67.5) | 22 (66.7) | 5 (71.4) | >0.99 |
Procedure efficacy and clinical follow‑up
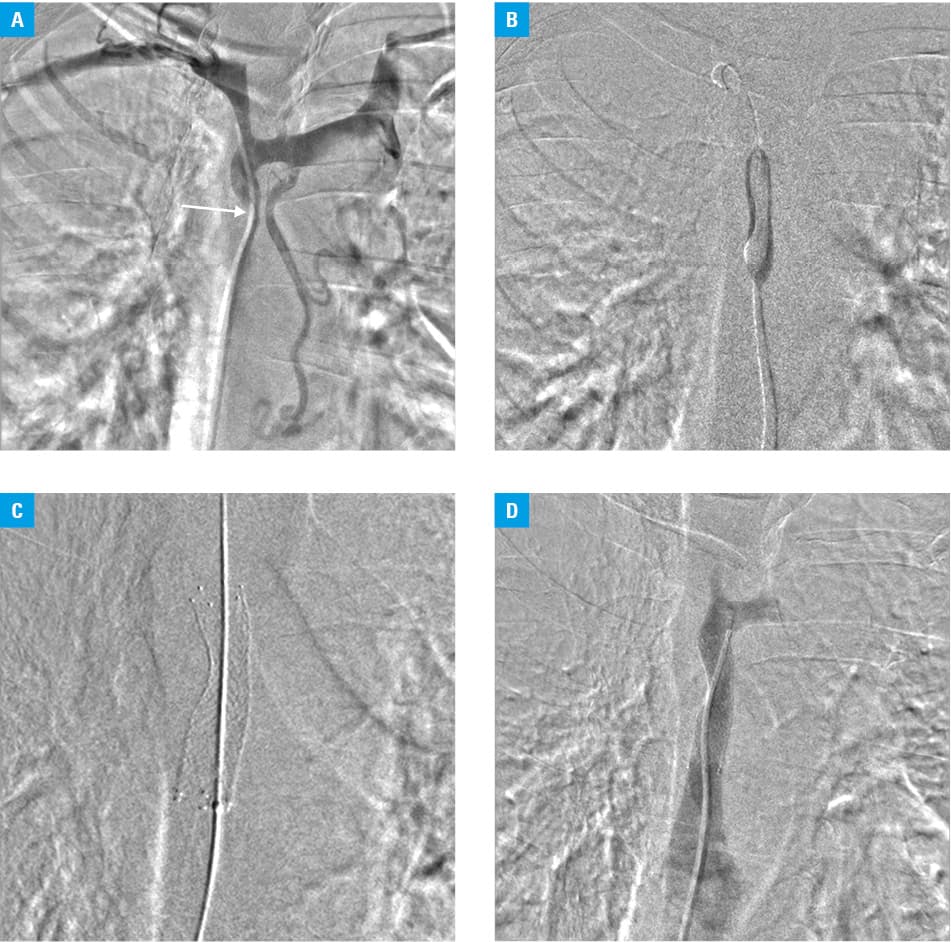
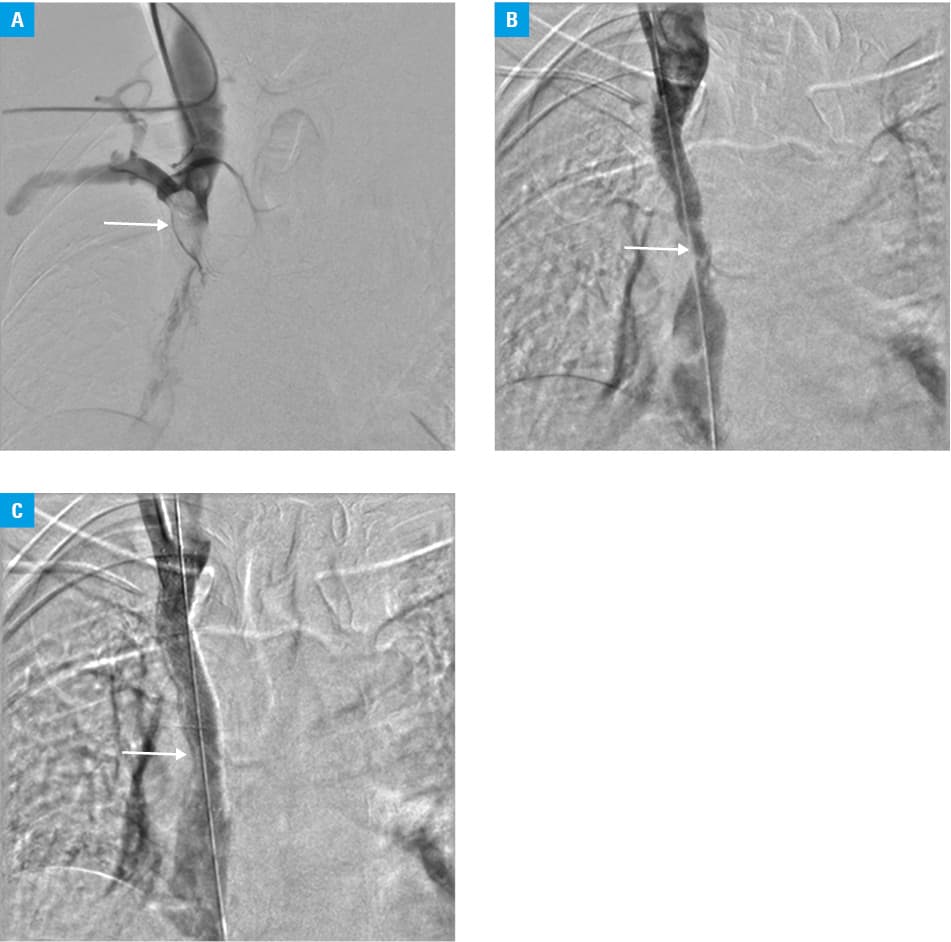
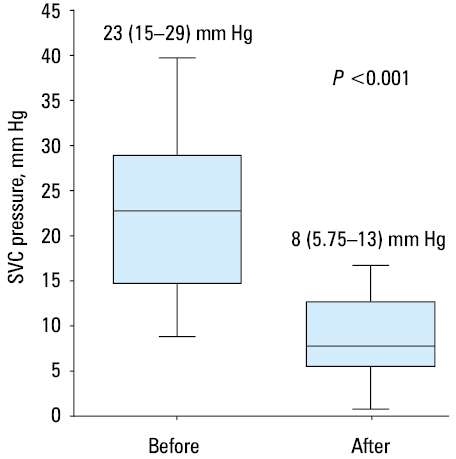
The procedure was successful in 97.5% of the cases (39 of 40 patients). In 1 patient, who had previously been treated with chemotherapy, the SVC obstruction could not be crossed with the guidewire. Predilatation with a balloon catheter was performed prior to 28 stent placements (56%; Figure 2). In all the procedures with at least 1 stent implanted, the postdilatation with a balloon catheter was performed, thus there were no cases with residual stenosis exceeding 30%. In 21 patients (52.5%), residual stenosis smaller than 30% was noted, despite postdilatation with a balloon catheter. The majority of patients (70% of the total study population) had only 1 stent implanted. In all other cases, more than 1 stent was necessary owing to the complexity of the lesion (Figure 3). No significant differences were found between the size of the stents and the balloon catheters depending on whether or not the patient had previously received anticancer treatment. All the procedural details are presented in Table 3. There was a considerable decrease in the median (IQR) pressure measured in the SVC following stent implantation, as compared with the values before the procedure in the entire study population (23 [15–29] vs 8 [5.75–13] mm Hg; P <0.001; Figure 4).
Characteristic | Overall | Previous anticancer treatment | No previous anticancer treatment | P value |
Data are presented as number (percentage) or median (interquartile range).
Abbreviations: PTA, percutaneous angioplasty | ||||
Stents per patient, n (%) | ||||
Group size | n = 40 | n = 33 | n = 7 | – |
0 | 1 (2.5) | 1 (3) | 0 | – |
1 | 28 (70) | 23 (69.7) | 5 (71.4) | |
2 | 6 (15) | 5 (15.2) | 1 (14.3) | |
3 | 4 (10) | 4 (12.1) | 0 | |
4 | 1 (2.5) | 0 | 1 (14.3) | |
Stent diameter, % per stent | ||||
Group size | n = 56 | n = 45 | n = 11 | – |
10 mm | 4 (7.2) | 4 (8.9) | 0 | 0.39 |
12 mm | 41 (73.2) | 34 (75.6) | 7 (63.6) | |
14 mm | 11 (19.6) | 7 (15.6) | 4 (36.4) | |
Stent length, % per stent | ||||
Group size | n = 56 | n = 45 | n = 11 | – |
40 mm | 13 (23.2) | 11 (24.4) | 2 (18.2) | 0.76 |
60 mm | 24 (42.9) | 18 (40) | 6 (54.5) | |
80 mm | 19 (33.9) | 16 (35.6) | 3 (27.3) | |
Stent model, % per stent | ||||
Group size | n = 56 | n = 45 | n = 11 | – |
S.M.A.R.T Control | 44 (78.6) | 38 (84.4) | 6 (54.5) | 0.06 |
Zilver 635 | 11 (19.6) | 6 (13.3) | 5 (45.5) | |
Venovo | 1 (1.8) | 1 (2.2) | 0 | |
PTA before stent implantation, % per stent | ||||
Group size | n = 56 | n = 45 | n = 11 | – |
Performed | 44 (78.6) | 38 (84.4) | 6 (54.5) | 0.045 |
None | 12 (21.4) | 7 (24.4) | 5 (45.5) | |
Diameter of PTA balloon if performed, % per stent | ||||
Group size | n = 44 | n = 34 | n = 10 | – |
10 mm | 13 (29.5) | 9 (26.5) | 4 (40) | 0.17 |
12 mm | 27 (61.4) | 23 (67.6) | 4 (40) | |
14 mm | 4 (9.1) | 2 (5.9) | 2 (20) | |
Imaging parameters | ||||
Group size | n = 47 | n = 40 | n = 7 | – |
Contrast, ml, per procedure | 100 (60–120) | 100 (70–125) | 120 (95–135) | 0.63 |
Acquisition, mGy | 279 (148–422) | 273 (106–421) | 304 (204–393) | 0.69 |
Within 48 hours of the procedure, clinical improvement of the symptoms was achieved in 38 patients (95%). No clinical changes were noticed in 2 patients who had previously received anticancer treatment (Table 4). During 30 days of follow‑up, 3 cases of stent (S.M.A.R.T Control) reocclusion were observed. All these patients had previously been treated with radio- and chemotherapy. Two patients (a 70‑year‑old woman, NSCLC stage 3C and a 65‑year‑old woman, NSCLC stage 3B) experienced compression of the stents due to tumor progression. In both cases, dilatation with a balloon catheter was performed initially, followed by implantation of 1 additional stent in 1 case and 2 additional stents in the other case, restoring the flow through the vessel. In the third case (a 50‑year‑old man with stage 3B thymus cancer), stent reocclusion was observed within 14 days of the procedure. In this patient, a recanalization attempt was unsuccessful, because the lesion could not be passed through with the guidewire. The patient died 2 weeks after the second procedure.
Outcomes | Overall | Previous anticancer treatment | No previous anticancer treatment | P value |
Data are presented as number (percentage) or median (interquartile range).
a Kishi score difference before and after EVT
Abbreviations: see Figure 1 | ||||
Symptom response | ||||
Group size | n = 40 | n = 33 | n = 7 | 0.67 |
Complete relief of symptoms | 12 (30) | 11 (33.3) | 1 (14.3) | |
Moderate clinical improvement | 21 (52.5) | 16 (48.5) | 5 (71.4) | |
Mild clinical improvement | 5 (12.5) | 4 (12.1) | 1 (14.3) | |
No clinical change | 2 (5) | 2 (6.1) | 0 | |
Kishi score after EVT | 3 (2–4) | 3 (2–4) | 3 (3–4.5) | 0.2 |
Kishi score differencea | –4 (–4 to –3) | –4 (–4 to –3) | –4 (–4 to –3) | 0.93 |
Complications | ||||
Group size | n = 40 | n = 33 | n = 7 | – |
None | 35 (87.5) | 30 (91) | 5 (71.4) | |
Death <24 h after EVT | 1 (2.5) | 1 (3) | 0 | |
Stent migration | 1 (2.5) | 1 (3) | 0 | |
Stent rupture | 1 (2.5) | 0 | 1 (14.3) | |
Associated with vascular access | 2 (5) | 1 (3) | 1 (14.3) | |
Length of hospitalization, d | 3 (3–4) | 3 (3–4) | 3 (3–3) | 0.32 |
Stent patency | ||||
Group size | n = 39 | n = 32 | n = 7 | >0.99 |
Primary | 36 (92.3) | 29 (90.6) | 7 (100) | |
Secondary | 38 (97.4) | 31 (96.9) | 7 (100) | |
In the total study population, the primary rate of patency in the follow‑up period was 92.3% (36 of 39 patients), and the rate of secondary patency reached 97.4% (38 of 39 patients).
After the procedure, all patients received anticoagulant treatment with subcutaneous LMWH at 1 mg/kg body weight.
Complications
The study population experienced 4 types of complications (Table 4). In 1 patient, cardiac arrhythmia (sustained ventricular tachycardia) was noted in the catheter laboratory immediately after the procedure of the stent (S.M.A.R.T Control) implantation, and the patient died. The patient (a 65‑year‑old woman) had no significant comorbidities, including no history of cardiac arrhythmia or heart failure. In the second case (a 68‑year‑old man), the stent (S.M.A.R.T Control; 12 mm in diameter, 60 mm in length) slipped into the right atrium shortly after placement. Nevertheless, the stent was partially relocated using a balloon catheter (12 mm in diameter, 60 mm in length) back to the SVC. The new position of the stent was secured with a second stent (80 mm in length, 12 mm in diameter, S.M.A.R.T Control). In the third case (an 81‑year‑old man), the stent (Zilver 635) rupture was noted during balloon catheter postdilatation with small extravasation of contrast most likely into the tumor mass, accompanied by cough without desaturation. Immediate balloon catheter inflation was performed to stop the leakage, with resolution of the symptoms. In the other 2 cases (a 50‑year‑old man and a 75‑year‑old woman), there were complications related to vascular access (hematoma and pseudoaneurysm). However, they did not require further intervention. A comprehensive overview of all outcomes of the stent implantation procedures, including complications, is presented in Table 4.
Discussion
This is one of the few studies assessing effectiveness and safety of EVT with stent implantation of SVCS caused by diverse cancers. The key conclusions of this investigation are as follows: 1) EVT of SVCS with stent implantation is a successful method in terms of both technical and clinical outcomes; 2) the stent implantation procedure is associated with a low complication rate; and 3) EVT with stent implantation can be both the first‑line treatment and a subsequent intervention in cases where previous conventional therapy has failed.
Over the past decade, the efficacy of stent implantation in patients with malignant SVCS has been evaluated in a single randomized study, a number of prospective and retrospective cohort studies, as well as in several case series. Takeuchi et al9 performed a phase II trial and phase III randomized control trial (RCT), evaluating endovascular SVC stenting with bare metal stents. Twenty‑eight patients with uncontrollable symptoms and undergoing medical treatment for malignant SVCS were enrolled in the phase II trial. In that study, the effectiveness of stent placement was measured based on reduction in symptom score within 14 days after the procedure. The results showed a significant reduction in the median symptom number from 10.5 prior to the procedure to 3 following stent placement (P <0.0001). A noticeable improvement in venous stenosis determined on postprocedural digital subtraction venography was reported in 27 patients (96.4%), and a significant reduction in collateral vessels was identified in 24 individuals (85.7%). Moreover, the stent implantation was successfully performed in all patients, demonstrating a 100% technical feasibility. These results were confirmed in the phase III trial, in which significant advantages of the stent implantation were noticed in the trial group (n = 16) in comparison with the control group (n = 16; P <0.0001).9 However, there was no difference in the survival rate between the 2 groups of patients. Then, in a prospective study of 104 patients with malignant SVCS, Chan et al10 found no significant association between the stent implantation procedure and patient survival. Our results are in line with those from the phase II and phase III RCTs with a high technical success rate of 97.3%, as well as satisfactory symptom response—complete relief of symptoms achieved in 30% of cases and moderate or mild symptom relief in 65% of cases. Nevertheless, our study did not include the analysis of survival.
The data from several retrospective observational studies are also consistent with our results and contribute to the observed trend of high efficacy of EVT in patients with malignant SVCS. The largest retrospective observational study published to date, conducted by Fagedet et al,11 enrolled 164 patients with malignant SVCS. The authors reported that EVT with bare metal stent implantation was clinically effective in 95% of patients. Moreover, they also examined the predictive factors associated with the efficacy of EVT. Thus, the only independent factor responsible for the failure of EVT was SVC thrombosis. Within our study population, there were no patients with primary SVC thrombosis, and this may be one of the reasons for the high success rate of the procedure.11 Similarly, Tanigawa et al12 observed a 93% success rate in the case of SVCS due to external compression, and only a 50% success rate of EVT for intraluminal tumors. Altogether, clinical and technical success rates in published studies ranged from 93% to 100% and 83% to 100%, respectively. Improvement in clinical symptoms was achieved within 1 to 5 days, most often between 48 and 72 hours following the stent placement.10,11,13-20 In comparison, chemotherapy or radiotherapy typically requires several weeks to take effect.21
Regarding the conventional anticancer treatment, the majority of patients investigated in our study had previously undergone chemo- and / or radiotherapy. Our results seem to confirm that stent implantation is also effective in patients in whom conventional treatment has been ineffective or who have experienced refractory symptoms. A similar observation was made a few years ago by Leung et al.16 They conducted an analysis comparing salvage stenting after conventional treatment against primary stenting in SVCS. The authors reported no significant difference in the rate of clinical or technical achievement, relapse, and complications.16
Similarly to the technical success or clinical outcome, the complication rate of about 10% in our study is consistent with the data from the existing literature. The overall complication rate from previous observational studies ranges from 0% to 19%.10,11,13-21 In general, the complications associated with EVT seem to be comparable to those observed in patients who have undergone radio- and chemotherapy.22 The most common EVT‑related major complications included stent migration or malposition, bleeding, pulmonary embolism, infections, arrhythmia, perforation, or complications related to vascular access. As stated previously, the prospective phase II trial conducted by Takeuchi et al9 showed that the complication rate associated with stent‑related grade 3 or higher adverse events was 14.3%, including pulmonary embolism, pain in the lower back, and hypotension. Fagedet et al11 observed 21 complications (12.8%) during the follow‑up period. Of them, only 4.9% were directly linked to the procedure. Interestingly, these authors found that the use of stents larger than 16 mm in diameter was the sole significant risk factor for all complications (16 complications with 54 stents; P = 0.008).11 In our study, the stent diameter did not exceed 14 mm, which may contribute to the satisfactory safety level of the stent placement.
However, it should be noted that EVT with the stent implantation is a form of symptomatic and palliative therapy. The recurrence of symptoms may manifest at varying frequency depending on the advancement of the neoplastic disease. Thus, the recurrence of SVCS was observed in 10% to 21.9% of patients during the follow‑up period in the studies conducted in the past decade.10,19-21,23-28 In most patients with recurrence, repeat intravascular interventions, such as angioplasty alone or angioplasty in combination with additional stent implantation were sufficient to achieve symptom resolution.10,19-21,23-28 In our study, we observed 3 cases of SVCS recurrence—1 due to thrombosis in a previously malpositioned stent and 2 cases associated with cancer progression. However, the patients were only followed‑up for 1 month from the day of intervention, which may have contributed to the underestimated relapse rate in the study population.
It is important to note that a comparison of different clinical trials should be interpreted with caution due to some inconsistencies in the definition of complications, the length of follow‑up, and different types of stents used. Another comparison of different stent types has been conducted by Duvnjak and Andersen.13 They compared 3 different types of stents: 2 venous dedicated stents (Zilver Vena; Cook Medical and Sinus‑XL; Optimed, Ettlingen, Germany) and 1 nonvascular dedicated stent (E’Luminexx; Bard / Angiomed, Karlsruhe,Germany). The study showed a similar efficacy for all types of stents, with only minimal superiority observed for 1 of the venous dedicated stents. However, it is worth noting that the study was a case series with a sample size of 30 patients.13 We used a variety of stent types, that is, 2 types of nonvenous dedicated stents and 1 type of venous dedicated stent. Despite the application of nonvenous dedicated stents in the majority of cases, the technical success rate was high, with a primary patency rate of 92.3% at 1 month. Thus, it can be concluded that in patients with malignant SVCS and anticipated short life expectancy, the nonvenous dedicated stents appear as effective and safe as the venous dedicated stents. This is important when considering the accessibility of this form of palliative therapy, since venous dedicated stents are several times more expensive than those not designed for use in veins.
Finally, it seems that anticoagulation should be administered after stent implantation, due to high thrombogenic effect of the stent, until the neoendothelium covers its intravascular surface. However, the optimal anticoagulation regimens for patients with SVCS have not yet been established in any guidelines. At our institution, we recommend anticoagulation mostly with LMWH, administered on a continuous basis. This is due to both higher prothrombotic susceptibility in patients with malignancy29,30 and supposed risk of in‑stent thrombosis.31,32 In the existing literature, a wide range of different anticoagulation strategies has been proposed,5 but to date, there has been no consensus in this area. Therefore, further studies in this field are required.
Limitations
This study is subject to several limitations. Firstly, it was of retrospective, single‑center, and noncontrolled design. This may be the reason for the incomplete observations, which may result from a lack of a follow‑up protocol or a lack of detailed data on cancer diagnosis as well as observational bias. Secondly, due to the heterogeneity of the population, survival analysis was not possible, and only in‑hospital deaths were included in the analysis. Thirdly, the study is limited by a small sample size. Fourthly, the examined population was divergent both in terms of the type of cancer and the treatment that had been administered prior to the study. Hence, it is a challenge to generalize and draw broad conclusions from the results we have obtained.
Conclusions
To sum up, EVT with stent placement is an effective type of treatment in terms of symptom relief in patients with SVCS due to underlying malignancy. The procedure is characterized by an acceptable incidence of complications, whether it is the primary or subsequent treatment in patients who have previously undergone radio- and / or chemotherapy.
- Plekker D, Ellis T, Irusen EM, et al. Clinical and radiological grading of superior vena cava obstruction. Respiration. 2008; 76: 69‑75. | Crossref
- Rice TW, Rodriguez RM, Light RW. The superior vena cava syndrome: clinical characteristics and evolving etiology. Medicine (Baltimore). 2006; 85: 37‑42. | Crossref
- Wilson LD, Detterbeck FC, Yahalom J. Clinical practice. Superior vena cava syndrome with malignant causes. N Engl J Med. 2007; 356: 1862‑1869. | Crossref
- Friedman T, Quencer KB, Kishore SA, et al. Malignant venous obstruction: superior vena cava syndrome and beyond. Semin Intervent Radiol. 2017; 34: 398‑408. | Crossref
- Azizi AH, Shafi I, Shah N, et al. Superior vena cava syndrome. JACC Cardiovasc Interv. 2020; 13: 2896‑2910. | Crossref
ARTICLE INFORMATION