Association between atrial fibrillation and cognitive performance in older individuals
Key words: dementia, elderly, silent atrial fibrillation

 CC BY 4.0
CC BY 4.0
Association between atrial fibrillation and cognitive performance in older individuals
Introduction: Atrial fibrillation (AF) coexists with dementia in older population. AF often remains undiagnosed in its asymptomatic, silent form, that is, silent AF (SAF).
Objectives: The aim of the study was to evaluate the relationships between cognitive performance and both symptomatic and asymptomatic AF, diagnosed via a long‑term (up to 30 days) wearable noninvasive electrocardiography monitoring system in a representative Polish population younger than 65 years.
Patients and methods: A sample of 2203 participants from the cross‑sectional NOMED‑AF (Noninvasive Monitoring for Early Detection of Atrial Fibrillation) study were enrolled in the analyses (mean [SD] age, 77.1 years; 48.4% women), out of which 491 (22.3%) were diagnosed with AF (41.3%, with SAF).
Results: Mean (SD) number of points obtained by the respondents in the Mini‑Mental State Examination (MMSE) was 25.8 (0.1), and it was lower in the patients with AF than those with sinus rhythm (25.2 [0.22] vs 26 [0.11]; P <0.001). Moreover, there was a difference in the number of points obtained by the patients with symptomatic AF and SAF, with the latter group having the lower score (25.8 [0.26] vs 24.3 [0.38]; P = 0.001). Finally, in a multivariable logistic regression model, the impact of SAF (but not that of symptomatic AF) on MMSE scores was demonstrated.
Conclusions: In the older population, AF is associated with a lower MMSE score. In the case of SAF, this relationship is independent of other risk factors. This suggests the need for an active search for SAF in the group of patients with dementia and, on the other hand, screening for cognitive disorders in older patients with accidentally detected SAF.
What's new?
To the best of our knowledge, this is the first study showing an association between silent atrial fibrillation and a higher probability of dementia in a broad, representative population of older adults. The association seems to be independent of other factors, including history of stroke. The above phenomenon requires further research. However, regardless of the nature and direction of the relationship between arrhythmia and cognitive impairment, the results indicate the need for active search for asymptomatic atrial fibrillation (AF) in patients with dementia and screening for cognitive disorders in older individuals with accidentally diagnosed silent AF.
Introduction
Atrial fibrillation (AF) is the most common form of arrhythmia in the older population, and advancing age is the most prominent risk factor both for AF and its complications.1 In recent years, we have observed not only an increase in the absolute number of AF patients, but also a rise in its prevalence, and mortality rates, which is mainly due to the aging of the general population and the rise in the incidence of age‑related diseases conducive to the development of AF.2 It is estimated that individuals aged 60–69, 70–79, and 80–89 years are at a 4.98, 7.35, and 9.33‑fold higher risk of developing AF, respectively, as compared with those aged 50–59 years.3 Most patients with AF are over 65 years old.3 For this reason, proper management of AF patients requires taking into account the complexity of typical geriatric problems.4
The data regarding the prevalence of AF in this population appear to be significantly underestimated due to possible oligo- or asymptomatic course of arrhythmia. About one‑third of patients are unaware of AF symptoms.5 It seems that older adults are at a high risk of not being diagnosed with AF,6,7 probably due to the masking influence of comorbidities and their treatment, lack of physical activity that might enhance symptoms, or simply worse medical care. According to current knowledge, silent AF (SAF) is still associated with an increased risk of ischemic stroke, major adverse cardiovascular events, and cardiovascular death, thus requiring assessment of cardioembolic risk and consideration of anticoagulation therapy.8 Moreover, in the case of asymptomatic AF, no diagnosis means no treatment, so in the long run, undiagnosed patients are at a higher risk of complications.5
Emerging evidence has shown a consistent association between AF and cognitive impairment or dementia, even without a history of stroke.9-16 Although AF and dementia share many common risk factors, this association appears to be independent of their presence.11,15 It is unclear, whether silent and symptomatic AF have similar associations with dementia.
Based on the cross‑sectional epidemiological NOMED‑AF (Non‑invasive Monitoring for Early Detection of Atrial Fibrillation) study,17 we investigated the real AF prevalence in a representative Polish population aged 65 years or more via long‑term continuous electrocardiography (ECG) telemonitoring.17,18 In the presented ancillary analysis of the NOMED‑AF trial,17 we aimed to evaluate the relationships between cognitive impairment and both symptomatic and silent AF. To the best of our knowledge, this is the first study to investigate a possible association between SAF and cognitive performance, identified via long‑term ECG monitoring in a large, cross‑sectional population of older adults without implanted devices.
Patients and methods
The study was conducted as a subanalysis of the NOMED‑AF trial,17 a cross‑sectional observational study aiming to evaluate the prevalence of AF and its associated comorbidities in a representative, community‑dwelling Polish sample of adults aged 65 years or more. The detailed study protocol has been published elsewhere.11 The NOMED‑AF trial17 used a long‑term wearable noninvasive ECG monitoring system linked with an online platform for data analysis and storage. The studied group comprised of 3014 individuals, and the recruitment was performed between March 15, 2017 and March 10, 2018.
The enrollment was based on a random sample of individuals aged 65 years or more. The entire territory of the country was divided into 59 geographical strata. The regions from each stratum were then randomly selected by the proportional probability. At the end, the participants from the previously chosen areas were selected at random, based on their personal identity number. A similar number of men and women were assigned to each 5‑year age group.
The NOMED‑AF study17 was approved by the local bioethical committee (26/2015) and registered at clinicaltrials.gov (NCT03243474). Written informed consent was obtained from all participants.
Data collection
The patients were visited 3 times in their place of residence by a trained nurse. On the first visit, the data on demographic information, previously diagnosed AF, symptoms, and a history of AF and other cardiovascular and metabolic diseases were collected using a questionnaire. The participants were assessed using the Polish versions of the 15‑item Geriatric Depression Scale (GDS) and the Mini‑Mental State Examination (MMSE). Also, during the study visits, anthropometric measurements (body mass, height) and blood pressure measurements (using validated automated oscillometric devices) were taken, and biological samples (blood and urine) were collected.
Long‑term electrocardiography monitoring
Each study participant, regardless of their AF history, was equipped with a continuous ECG recording system. The set consisted of a vest fitted with ECG leads, 2 exchangeable recorders, and a docking station, which was developed and manufactured together with a transmission system, database, and analysis software (Comarch Healthcare, Kraków, Poland) specifically for the purpose of the study. The study participants were encouraged to wear the vest for the maximum time possible for up to 30 days, with short breaks for either hygienic or other necessary reasons. At regular time intervals, ECG data were transmitted from one of the recorders, through a docking station, to the central database using GSM technology, while the other recorder was connected to the vest and continued recording. All episodes automatically classified as AF by the platform’s software were verified and confirmed by trained cardiologists.
Outcomes
According to the current European Society of Cardiology 2020 guidelines,8 only AF episodes that lasted longer than 30 seconds, detected on long‑term ECG monitoring could be included in the analysis. SAF was defined as AF that was detected and confirmed in asymptomatic individuals.
Screening for cognitive impairment was performed using the Polish version of the MMSE. With a maximum score of 30 points, a score of 24–26 points was indicative of mild cognitive impairment, and a score below 24 points, as a suspicion of dementia.
Depressiveness was assessed using the 15‑item GDS, and a score of 6 points and higher was regarded as a suspicion of depression. Screening for depressiveness was performed only in patients with an MMSE score of 15 points or higher.
Hypertension was diagnosed if the average blood pressure values from 2 measurements during each visit were equal to or greater than 140 mm Hg (systolic) and / or equal to or greater than 90 mm Hg (diastolic), or if the patient had taken antihypertensive drugs in the previous 2 weeks due to an earlier diagnosis of hypertension.
Diabetes mellitus was diagnosed when glycated hemoglobin level was equal to or greater than 6.5%, or if the patient was taking glucose‑lowering agents because of an earlier diabetes diagnosis.
Chronic kidney disease (CKD) was defined as an estimated glomerular filtration rate below 60 ml/min/1.73 m2 or equal to or greater than 60 ml/min/1.73 m2 with coexisting albuminuria (albumin‑to‑creatinine ratio ≥30 mg/g).
The presence of coronary artery disease (CAD), heart failure (HF), and a history of stroke or transient ischemic attack were based on patient history or available medical records.
Body mass index (BMI) was calculated as weight in kilograms divided by squared height in meters (kg/m2).
Ethics
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the local bioethical committee (26/2015). Informed consent was obtained from all the study participants.
Statistical analysis
Although we achieved the oversampling of the oldest participant, it was corrected at the stage of statistical analysis, using weights to get population estimates. Continuous variables were presented as mean (SD) for normally distributed variables, or as median (interquartile range) for non‑normally distributed variables, while categorical variables were presented as counts and percentages. The significance between the groups was tested using the χ² test for categorical variables and the t test or the Mann–Whitney test for continuous variables. Normality was assessed using the Kolmogorov–Smirnov test.
To assess the prognostic effect of both clinical forms of AF on cognitive performance, main demographic variables, comorbidities, smoking status, a history of falls, and the GDS score were introduced to the multivariable logistic regression analysis. Due to a high risk of collinearity between the variables, the analysis was conducted based on 2 models, gradually expanding the range and number of covariates. In model 1, AF was adjusted to sex, age, and education level, while model 2 additionally included comorbidities, smoking status, occurrence of falls, and the GDS score. The results are presented as odds ratios (ORs) and 95% CIs. A 2‑sided P value below 0.05 was considered significant.
The analysis was performed using SPSS, version 19 (IBM Corp., Armonk, New York, United States).
Results
The study included 2203 participants who were assessed for cognitive impairment using the MMSE. Mean (SD) age of the respondents was 77.1 (7.87) years, 51.6% of whom were men.
In the analyzed population, AF was confirmed in 491 patients (22.3%). The respondents with AF were older, more often men, hypertensive, with diabetes mellitus, CAD, HF, CKD, or a history of stroke. They were less likely to suffer from hypercholesterolemia.
The silent form of arrhythmia was recognized in 203 AF patients (41.3%). The participants with SAF were more likely to be men and less likely to have a history of hypertension or HF. We did not observe differences in age, marital status, BMI, and comorbidities between the AF and SAF patients.
Baseline characteristics of the analyzed population are presented in Table 1.
Parameter | Overall (n = 2203) | AF absent (n = 1712) | AF present (n = 491) | P value | Symptomatic AF (n = 288) | Silent AF (n = 203) | P value |
Data are presented as number (percentage) unless provided otherwise.
Abbreviations: AF, atrial fibrillation; BMI, body mass index; CAD, coronary artery disease; CKD, chronic kidney disease; DM, diabetes mellitus; GDS, geriatric depression scale; HF, heart failure; IQR, interquartile range | |||||||
Age, y, mean (SD) | 77.1 (7.87) | 76.4 (7.83) |
| <0.001 | 79.2 (7.53) | 80.3 (7.32) | 0.11 |
BMI, kg/m2, mean (SD) | 28.1 (4.81) | 27.9 (4.72) | 28.6 (5.1) | 0.004 | 28.7 (5.45) | 28.5 (4.58) | 0.63 |
Men | 1136 (51.6) | 839 (49) | 297 (60.5) | <0.001 | 158 (54.9) | 139 (68.5) | <0.001 |
Current smokers | 263 (11.9) | 236 (13.8) | 27 (5.5) | <0.001 | 17 (5.9) | 10 (4.9) | 0.64 |
Former smokers | 833 (37.8) | 627 (36.7) | 206 (42) | 0.03 | 122 (42.4) | 84 (41.4) | 0.83 |
Falls | 452 (22.5) | 342 (21.9) | 110 (24.7) | 0.21 | 69 (26.6) | 41 (22) | 0.27 |
Married | 1265 (57.6) | 970 (56.9) | 295 (60.2) | 0.19 | 173 (60.1) | 122 (60.4) | 0.24 |
Education, n (%) | |||||||
Primary | 790 (36) | 609 (35.7) | 181 (36.9) | 0.96 | 98 (34.1) | 83 (40.9) | 0.19 |
Vocational | 461 (21) | 359 (21) | 102 (20.8) | 67 (23.3) | 35 (17.2) | ||
Secondary | 658 (29.9) | 513 (30.1) | 145 (29.6) | 82 (28.6) | 63 (31) | ||
Higher | 288 (13.1) | 226 (13.2) | 62 (12.7) | 40 (13.9) | 22 (10.8) | ||
Comorbidities, n (%) | |||||||
Hypercholesterolemia | 1711 (77.7) | 1363 (79.6) | 348 (70.9) | <0.001 | 213 (74) | 135 (66.5) | 0.07 |
CAD | 497 (22.7) | 337 (19.8) | 160 (32.9) | <0.001 | 99 (34.9) | 61 (30) | 0.27 |
Hypertension | 1777 (80.8) | 1359 (79.5) | 418 (85.1) | 0.005 | 259 (89.9) | 159 (78.3) | <0.001 |
HF | 499 (22.7) | 301 (17.6) | 198 (40.3) | <0.001 | 128 (44.4) | 70 (34.5) | 0.03 |
DM | 661 (30) | 475 (27.7) | 186 (37.9) | <0.001 | 108 (37.5) | 78 (38.4) | 0.84 |
CKD | 733 (33.7) | 509 (30.1) | 224 (46.2) | <0.001 | 121 (42.9) | 103 (50.7) | 0.09 |
History of stroke | 207 (9.4) | 136 (8) | 71 (14.5) | <0.001 | 38 (13.2) | 33 (16.3) | 0.35 |
Neoplasms | 305 (13.9) | 228 (13.3) | 77 (15.7) | 0.19 | 43 (14.9) | 34 (16.7) | 0.59 |
Thyroid diseases | 302 (13.8) | 215 (12.6) | 87 (17.8) | 0.004 | 53 (18.5) | 34 (16.7) | 0.62 |
GDS, points, median (IQR) | 3 (1–5) | 3 (1–5) | 3 (2–6) | 0.004 | 3 (2–5) | 3 (2–6) | 0.38 |
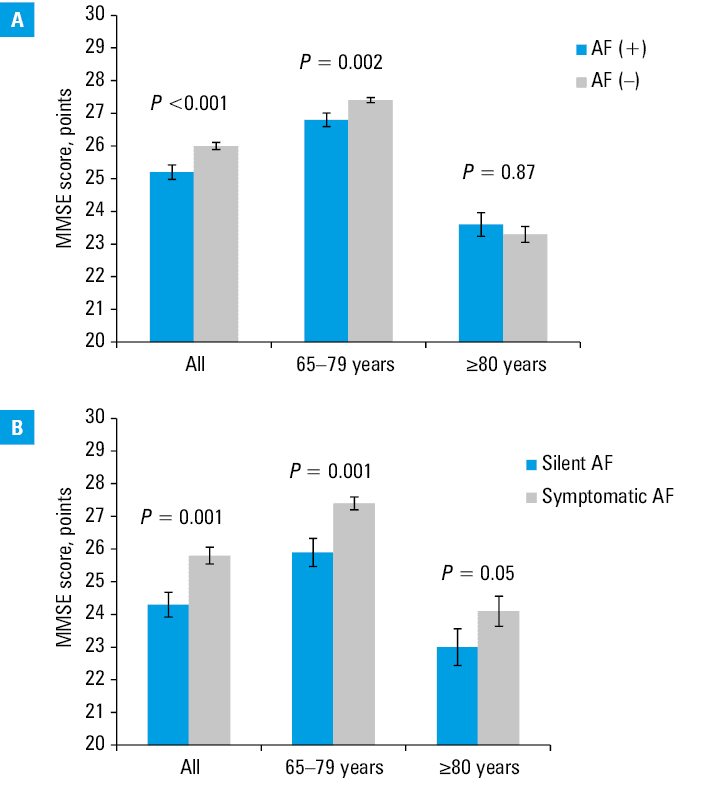
Mean (SD) number of points obtained by the respondents in the MMSE was 25.8 (0.1), and it was lower in patients with AF (25.2 [0.22]), as compared with those free of AF (26 [0.11]; P <0.001). This difference between the participants with and without AF was notable in the subgroup aged 65–79 years (26.8 [0.21] vs 27.4 [0.08]; P = 0.002), and absent in the patients aged 80 years and older (23.6 [0.36] vs 23.3 [0.24]; P = 0.87). Moreover, there was a difference in the number of points between the patients with symptomatic and asymptomatic AF, with the lower score obtained by the latter group (25.8 [0.26] vs 24.3 [0.38]; P = 0.001). This difference was significant in the patients aged 65–69 years (27.4 [0.2] vs 25.9 [0.43]; P = 0.001), but not in those aged 80 years and older (24.1 [0.46] vs 23 [0.56]; P = 0.05).
The number of points in the MMSE questionnaire is presented in Figure 1.
In the group diagnosed with AF, we had treatment data for 449 patients. Of those 261 (58.1%) were taking long‑term oral anticoagulation. There was no difference in the number of points obtained in the MMSE between the patients taking and not taking oral anticoagulants (25.2 [4.8] vs 25.3 [5.64]; P = 0.8).
Finally, in the hierarchic multivariable logistic regression model, the impact of individual factors on the probability of achieving an MMSE score below 24 points was assessed. The association of SAF (but not of symptomatic AF) with the MMSE score indicating the possibility of dementia turned out to be independent of other important demographic and clinical variables, such as age, sex, education, comorbidities, smoking status, the occurrence of falls, and the likelihood of depression (Table 2).
Parameter | Odds ratios (95% CI) | ||
Crude model | Model 1 | Model 2 | |
Model 1 adjusted for: age, sex, education
Model 2 adjusted for: age, sex, education, comorbidities, smoking status, falls, GDS
a P <0.05
Abbreviations: see Table 1 | |||
Symptomatic AF | 1.02 (0.68–1.53) | 0.7 (0.45–1.09) | 0.67 (0.42–1.08) |
Silent AF | 2.75 (1.86–4.06)a | 1.89 (1.22–2.91)a | 1.74 (1.1–2.73)a |
Men | – | 0.9 (0.67–1.21) | 1.34 (0.95–1.9) |
Age (per 1 year) | – | 1.12 (1.10–1.14)a | 1.1 (1.08–1.12)a |
Falls | – | – | 1.24 (0.9–1.71) |
GDS | – | – | 1.13 (1.08–1.18)a |
Current smoker | – | – | 0.75 (0.45–1.25) |
Ex‑smoker | – | – | 0.52 (0.36–0.76)a |
Education (vs higher) | |||
Primary | – | 11.2 (5.17–24.25)a | 9.9 (4.51–21.7)a |
Vocational | – | 7.69 (3.44–17.2)a | 7.78 (3.44–17.6)a |
Secondary | – | 3.71 (1.67–8.26)a | 3.75 (1.67–8.45)a |
Comorbidities | |||
Hypertension | – | – | 1.18 (0.79–1.75) |
HF | – | – | 0.83 (0.57–1.21) |
CAD | – | – | 0.82 (0.58–1.17) |
DM | – | – | 1.2 (0.88–1.64) |
CKD | – | – | 1.23 (0.9–1.67) |
Stroke | – | – | 1.85 (1.19–2.89)a |
Discussion
In our large cross‑sectional study of an older population, the patients with AF scored lower on a test assessing cognitive abilities. Interestingly, the individuals with SAF seemed to have a higher probability of dementia than those with a symptomatic form of arrhythmia.
Over the last 25 years, the amount of data on the relationship between AF and mild cognitive impairment and dementia, even in the absence of a clinically overt previous stroke, has been growing.9-16 Furthermore, these data indicate an association between AF and both vascular dementia and Alzheimer disease.12,13 The vast majority of observational data come from studies that determine the presence of AF based on medical history, medical records, or single ECG records, thus excluding patients with latent and asymptomatic arrhythmia. To the best of our knowledge, this study is the first to investigate a possible association between SAF and cognitive performance assessed with a screening tool.
Interestingly, although the MMSE score was lower among the elderly AF patients, after taking into account other factors (age, sex, marital status, comorbidities), only the silent form of arrhythmia was associated with a result indicating dementia. This may mean that the patient population identified by long‑term ECG monitoring differs from the groups analyzed so far in this respect. It seems that the adopted methodology allowed for the detection of an additional number of patients with paroxysmal arrhythmia. Chen et al19 indicate a relationship between dementia and only the persistent form of AF. Our results also suggest that age is such a strong prognostic factor for AF and dementia that it is difficult to recognize relationships between them which are independent of it.
The possible link between SAF and poorer performance in cognitive screening can be interpreted in many ways. First, patients with SAF are less likely to benefit from AF treatment protecting against the development of dementia. In fact, there are data on the beneficial effects of anticoagulant treatment20 and AF ablation21 on the development of cognitive disorders. Second, patients with SAF are generally likely to receive less medical care, which can lead to a lack of prophylaxis and / or delayed diagnosis and treatment of dementia. An opposite mechanism should also be considered. Patients with dementia less often report symptoms of arrhythmia, so arrhythmia in this group could be diagnosed only with systematic screening. Finally, it cannot be ruled out that SAF has a specific hemodynamic / prothrombotic / inflammatory phenotype, which predisposes a patient to specific neurological damage. This final aspect, of course, requires additional research.
In fact, it is still debatable whether the relationship between AF and cognitive impairment is causal. The basic impediment to resolving this issue is the impact of common risk factors, including, in particular, age and vascular or inflammatory diseases.22 Among the factors responsible for the influence of AF on the development of dementia, are, obviously, microembolisms or silent infarcts,23,24 but also hemodynamic disturbances related to irregular / fast heart rate,25,26 a decrease in cardiac output related to the loss of atrioventricular synchrony,27 and damage to the blood‑brain barrier due to the inflammatory process accompanying AF.28-30 Both the hemodynamic alterations and vascular inflammation could favor amyloid β-protein accumulation and phosphorylation of τ protein leading to Alzheimer disease.30,31 The possibility of complications resulting from microbleeding within the central nervous system in AF patients who use anticoagulants should also be considered. As already mentioned, stroke prophylaxis is associated with a reduction of the risk of dementia in AF, but interestingly enough, it seems that direct oral anticoagulants carrying a lower risk of intracranial bleeding are more effective in this respect than vitamin K antagonists.32 Our study did not show any differences in the results of the screening test assessing cognitive performance between the patients receiving and not receiving cardioembolic stroke prophylaxis. It should be highlighted, however, that we did not have complete data on this treatment in the study group, which could have influenced the results.
Another interesting aspect indicating a relationship between arrhythmia and cognitive impairment is the influence of AF on the development of cognitive disorders in younger patients. Our study showed that the relationship between the presence of AF in long‑term monitoring and a lower MMSE score was visible in the subgroup of patients aged 65–79 years, but lost relevance in the older subgroup, as confirmed by other studies.16,33 We might speculate about the additional influence of risk factors of neurodegeneration in the patients aged 80 years and older.
The beneficial effects of education and the relationship between a history of stroke and the likelihood of cognitive disorders are undisputed. However, the protective effect of smoking in the past is interesting. In fact, quitting smoking has been shown to reduce the risk of dementia.34 Perhaps in this case, giving up the addiction was an element of a larger process of health‑promoting changes in the respondents.
This study indicates a substantial frequency of SAF in the group of patients of over 65 years and its relationship with worse performance in the cognitive testing. It seems to point to the need for systematic AF screening in this age group and implementation of efficient treatment. The extent to which this strategy may reduce the development of dementia requires further research.
The study has certain limitations. The cross‑sectional nature of the analysis did not allow for drawing conclusions as to the direction of the causal relationship. The lack of data on the antiocoagulation treatment used did not permit a fully reliable assessment of its impact on the issue under study. Additionally, the selection of patients may have been biased due to the high heterogeneity of the study population and low representation of participants with moderate and severe dementia.
Conclusions
In the older population, the presence of AF is associated with a lower MMSE score. In the case of SAF, this relationship is independent of other risk factors. This suggests the need for an active search for asymptomatic AF in the group of patients with dementia and, on the other hand, screening for cognitive disorders in older patients with accidentally detected asymptomatic AF.
- Staerk L, Sherer JA, Ko D, et al. Atrial fibrillation: epidemiology, pathophysiology, and clinical outcomes. Circ Res. 2017; 120: 1501‑1517. | Crossref
- Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a global burden of disease 2010 study. Circulation 2014; 129: 837‑847. | Crossref
- Chyou JY, Hunter TD, Mollenkopf SA, et al. Individual and combined risk factors for incident atrial fibrillation and incident stroke: an analysis of 3 million at‑risk US patients. J Am Heart Assoc. 2015; 4: e001723. | Crossref
- Polidori MC, Alves M, Bahat G, et al. Atrial fibrillation: a geriatric perspective on the 2020 ESC guidelines. Eur Geriatr Med. 2021; 2: 1‑14. | Crossref
- Dilaveris PE, Kennedy HL. Silent atrial fibrillation: epidemiology, diagnosis, and clinical impact. Clin Cardiol. 2017; 40: 413‑418. | Crossref
ARTICLE INFORMATION